EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [위암학회 KINGCA 2016]
[위암학회 KINGCA 2016]

일시: 2016년 4월 21일 (목)- 4월 23 (토)
장소: 소공동 롯데호텔


학회 프로그램 책은 매우 간단했습니다. 대신 핸드폰에 앱을 설치하면 모든 초록을 볼 수 있어 편했습니다.
 김진복 교수님을 기리기 위하여 임원들이 사진을 찍었습니다.
김진복 교수님을 기리기 위하여 임원들이 사진을 찍었습니다.
![]() 1. Symposium 1. GEJ cancer
1. Symposium 1. GEJ cancer
1) Staging and classification (Andrew Barbour, University of Queensland, Australia)
- PET : upstaging 15%, FDG-avid 10%, 예후인자로 쓰일 수 있다. 치료방침 선정에 이용될 수 있는지는 약간 불명확하다.
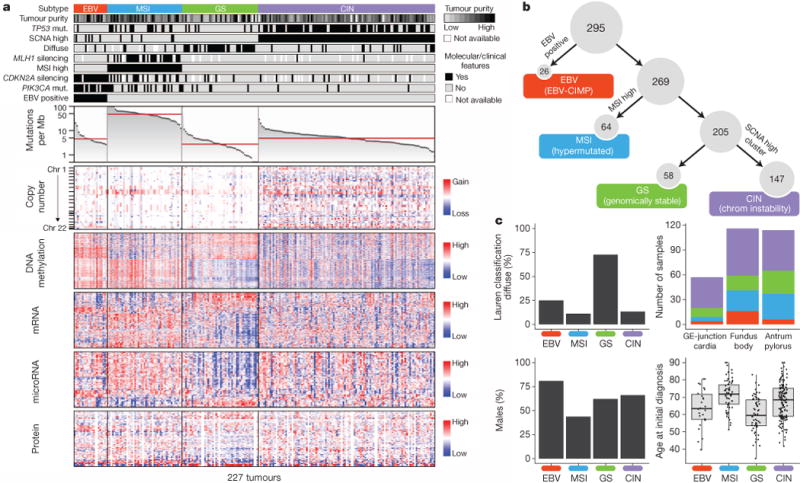
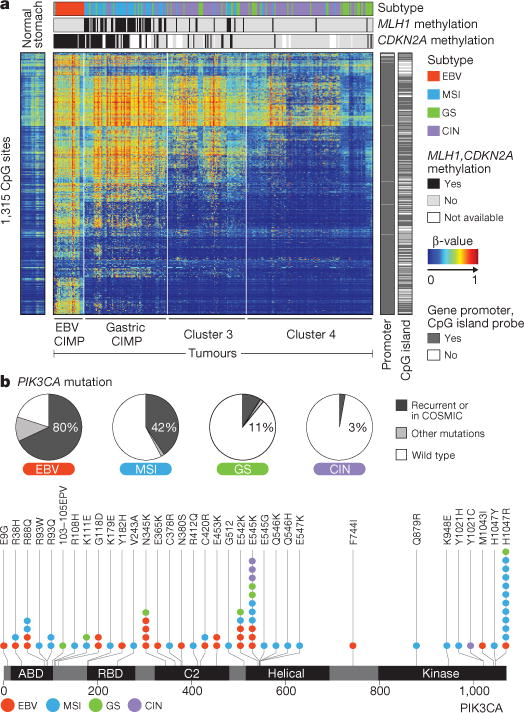
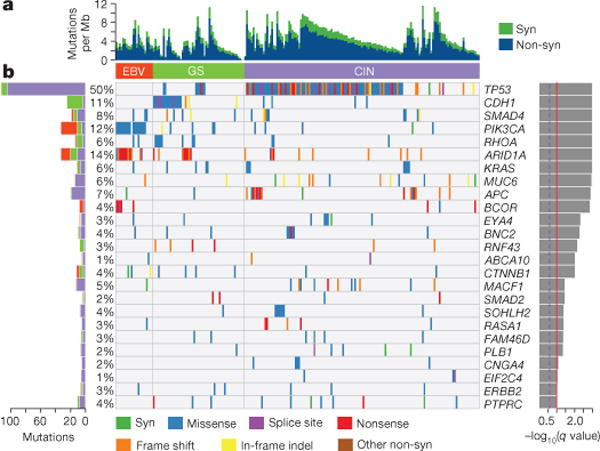
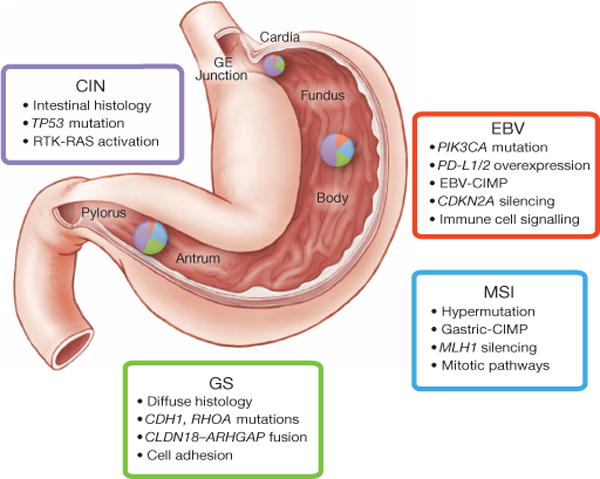
- Molecular classification: GEJ cancer는 catastrophic genomic event가 많다.
* 참고: Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014


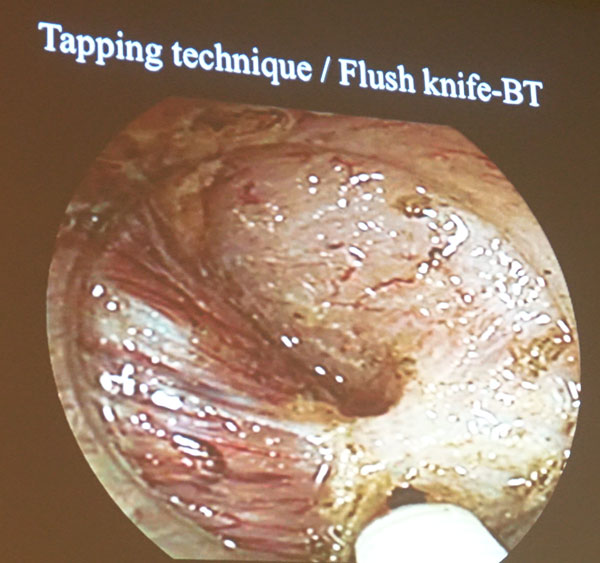
2) Endoscopic treatment for GEJ cancer (Toyonaga, Kobe U, Japan)
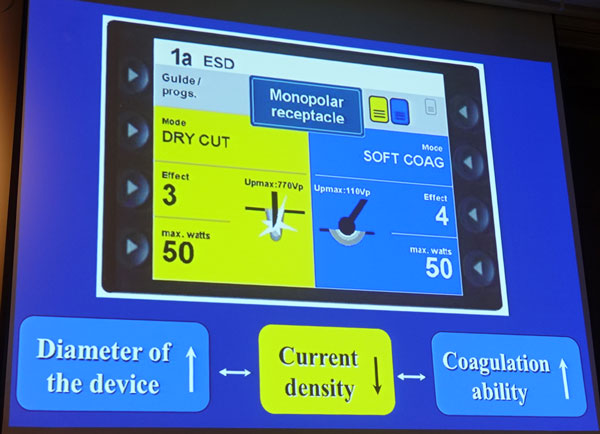
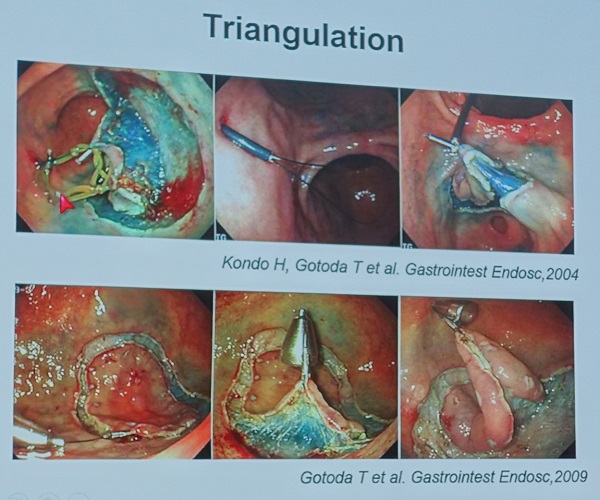
출혈을 최소화하기 위하여 정확한 깊이의 시술이 중요합니다. Branch vessel, penetrating vessel을 잘 coagulation하는 것이 중요합니다. "Submucosal dissection = vessel treatment"입니다.

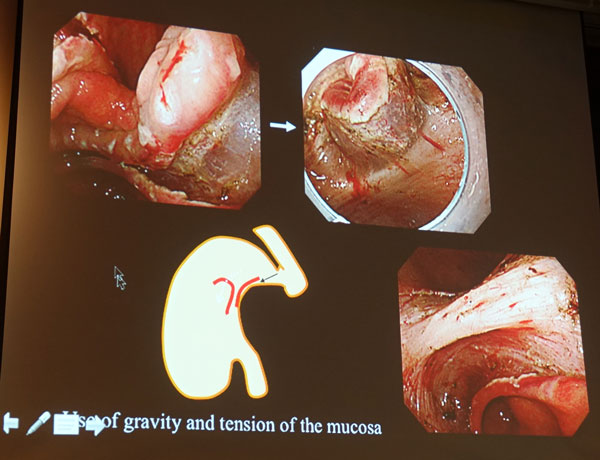
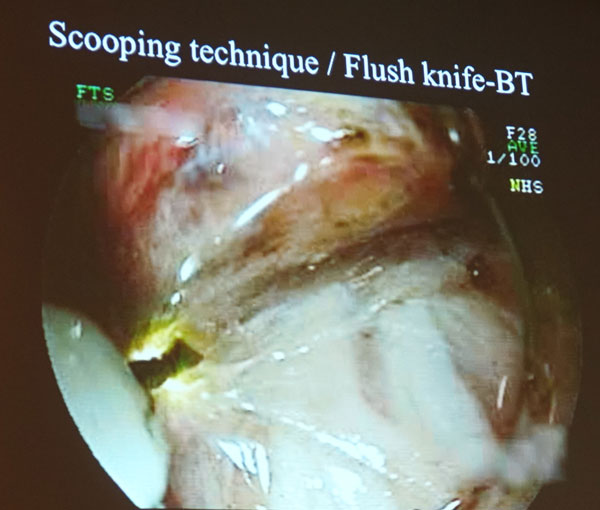
중력을 잘 이용해야 한다는 점을 강조하면서 흥미로운 그림을 보여주셨습니다. 뒤집어진 위 보이세요?
Fibrosis에서 사용하는 몇 가지 방법이 소개되었습니다. 정확히 이해할 수 없었습니다.
EGJ cancer에 대해서는 따로 분석한 자료는 보여주지 않고 문헌을 소개하셨습니다.

저는 협착에 대하여 질문을 했습니다. EGJ cancer의 내시경 치료 후 stricture는 식도 ESD 후보다 덜한 것 같다고 합니다. 경우에 따라서 oral steroid를 사용한다네요.
3) CCRT for EGJ cancer (Sun Young RHA, Yonsei U)
EGJ cancer에 대한 CCRT에 대한 연구는 많지 않습니다. 교수님께서는 위암의 항암치료 일반에 대하여 설명해주셨습니다.
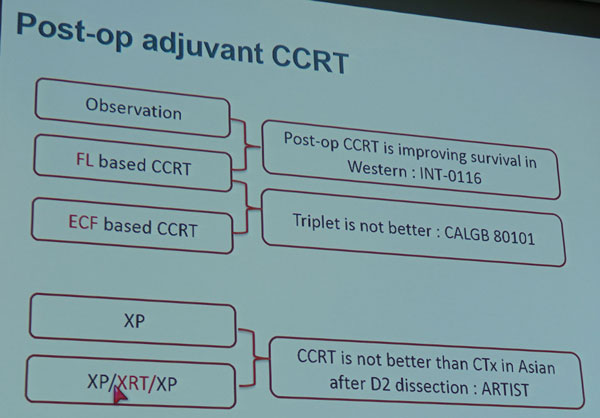
서양에서는 수술의 quality가 낮기 때문에 CCRT가 도움이 될 수 있습니다. 그러나 우리나라에서는 D2 dissection 후 CCRT는 chemo alone보다 우월하지는 않았습니다 (삼성서울병원의 ARTIST trial입니다. Lee J. J Clin Oncol 2012). 다만 local recurrence는 줄어들기 때문에 환자 선택이 중요합니다.
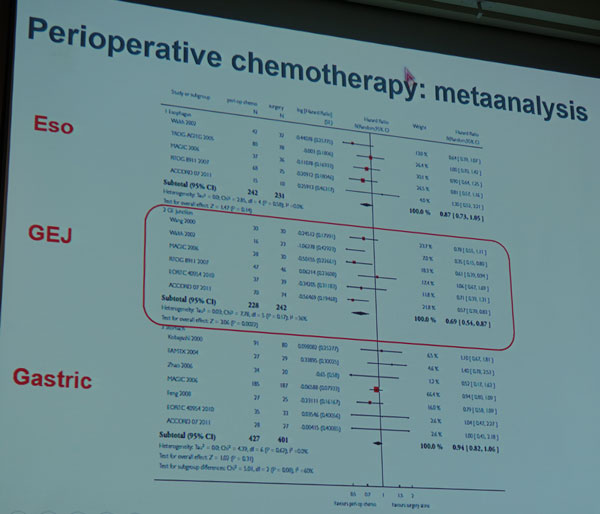
위암에서도 perioperative chemotherapy가 도움이 될 것이라는 일부 연구가 있습니다. 특히 EG junction cancer는 perioperative chemotherapy가 도움이 된다는 Cochrane 분석도 있습니다.
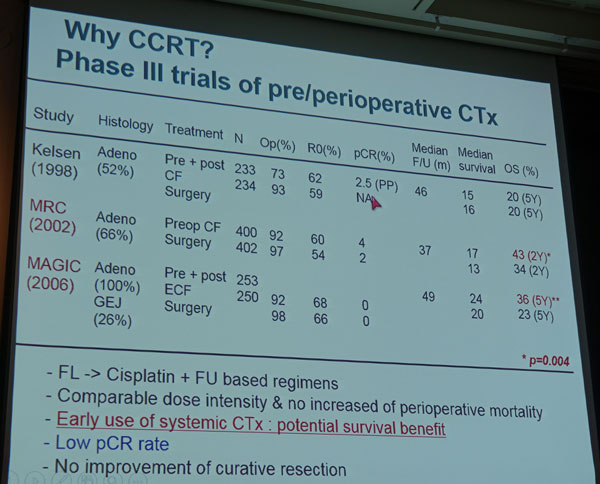
연세대에서 보만 4형이나 8 cm 이상 큰 보만 3형을 대상으로 preop CCRT 연구를 진행중이라고 합니다. 54명 중 12명이 laparoscopy에서 seeding이 있어서 screening failure를 보였지만, 아래 증례와 같이 dramatic response를 보이는 경우도 있었다고 합니다.
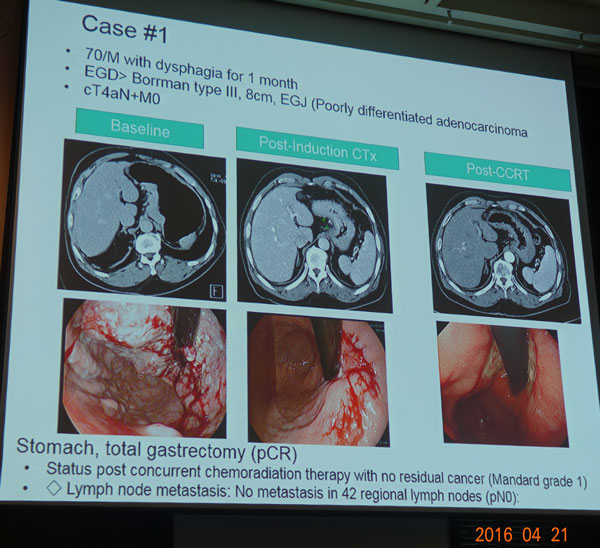
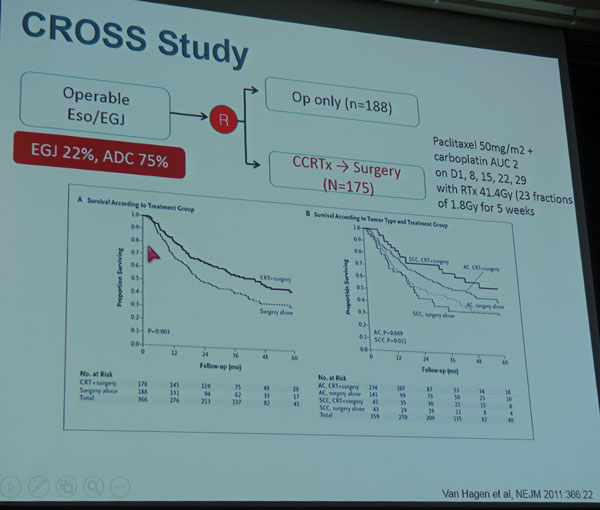
CROSS study에서 squamous cell carcinoma에 주로 도움이 되었지만 adenocarcinoma도 약간 도움이 되었다는 것에 주목합시다.
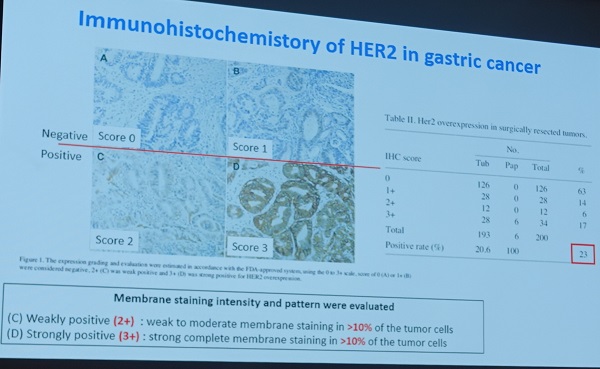
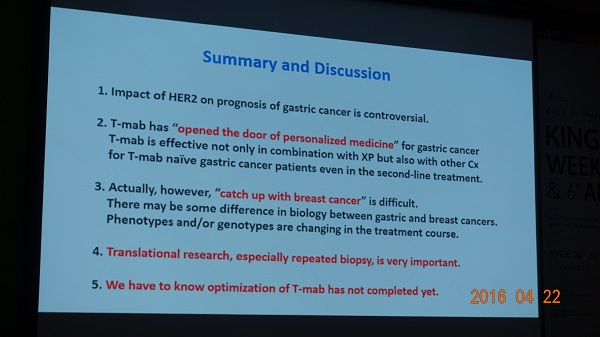
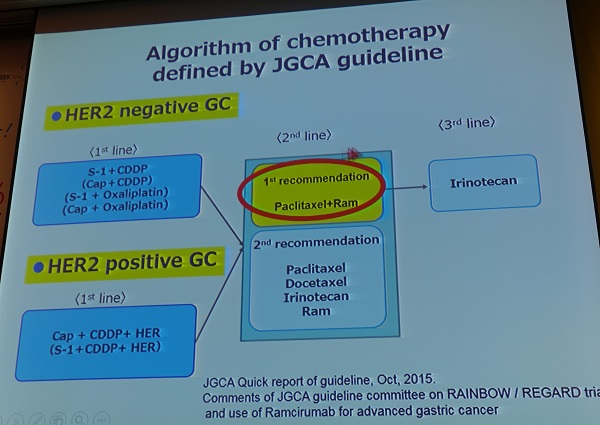
4) Innovotive treatments and emerging drugs (Lordick, Leipzig U, Germany)
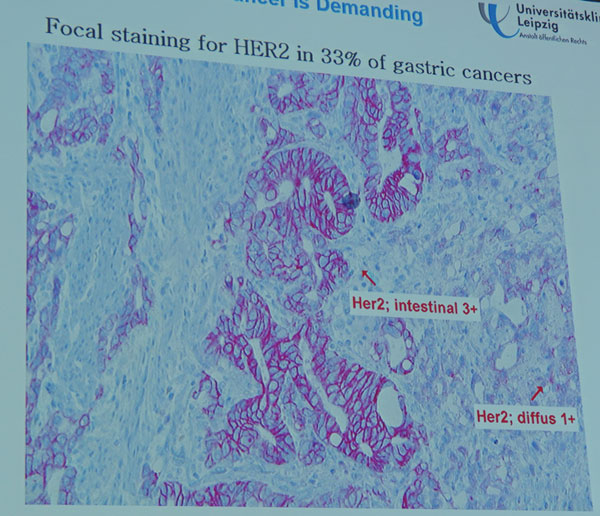
HER-2에 대한 염색에서 Focal staining을 보이는 경우가 33% 정도이므로 해석에 주의해야 합니다.
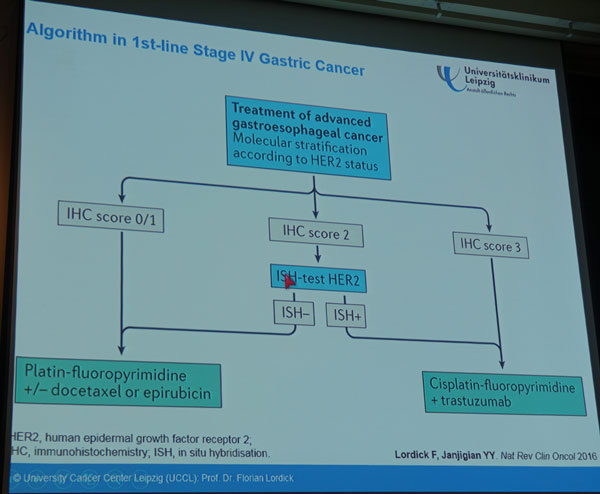
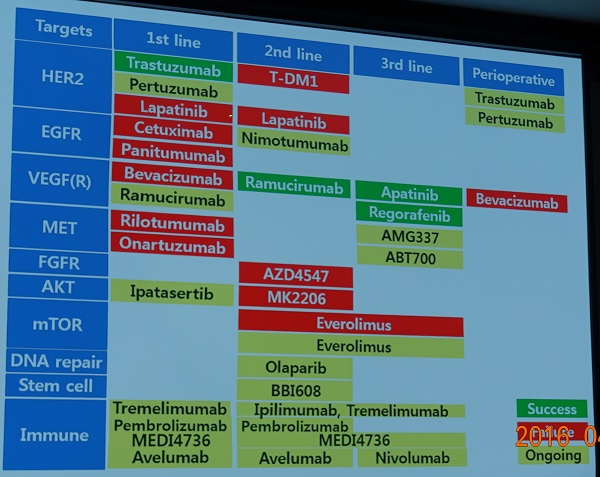
HER-2를 고려한 현재의 치료 algorithm은 아래와 같습니다.
치료 과정에서 여러번 검사해야 할 것 같습니다. 조직검사를 반복하기 어려우므로 liquid biopsy를 적용하는 방향으로 연구되고 있습니다.
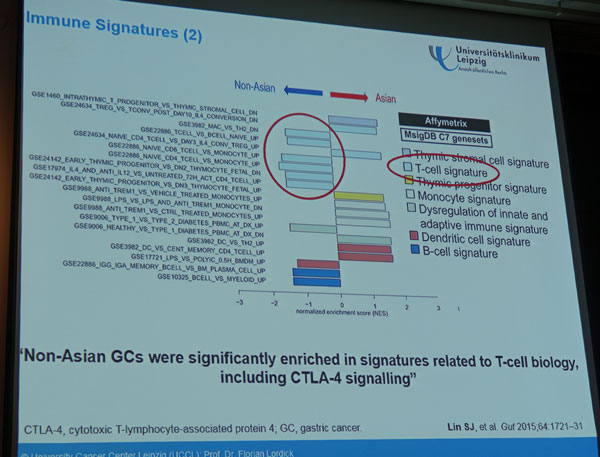
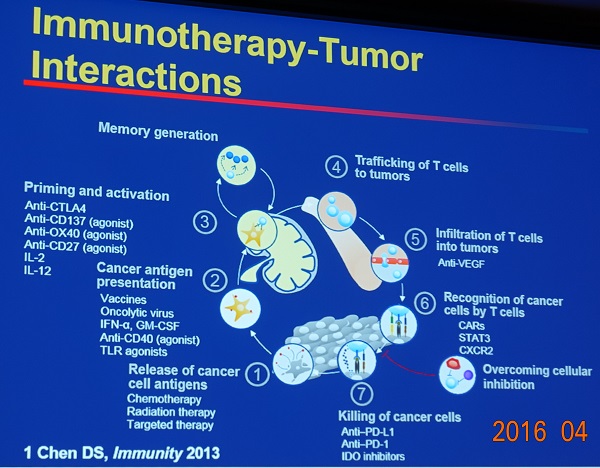
Immune therapy에 대한 관심이 높습니다. Immune checkpoint inhibition 같은 것이지요. 동양인과 서양인의 immune signature도 다르다고 합니다. Angiogenesis inhibition, cancer stem cell 등 다양한 분야의 연구가 시도되고 있습니다.
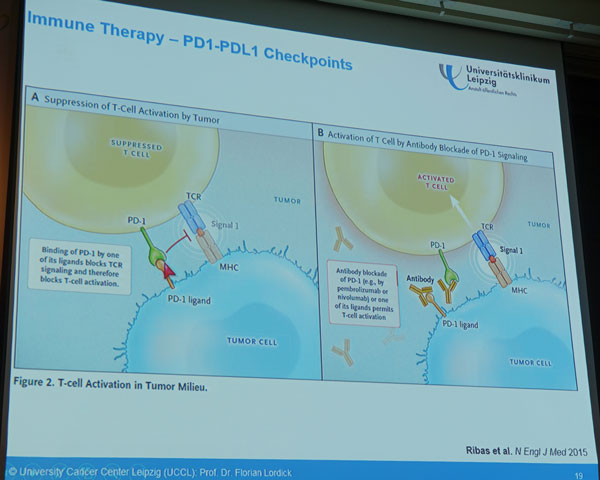
Tumor stroma as a drug target
- Immune therapy (anti-PD) : first data
- Anti-angiogenic therapy : Ramucirumab approved
![]() 2. JS MIN memorial lecture: Carcinoma of EG junction, past, present and future (Takashi Aikou, Kagoshima U, Japan)
2. JS MIN memorial lecture: Carcinoma of EG junction, past, present and future (Takashi Aikou, Kagoshima U, Japan)
2대 위암학회 회장님이셨던 민진식 교수님을 추모하는 memorial lecture였습니다. 외과에서는 이런 종류의 memorial lecture를 여는 전통이 있습니다. 좋아보였고 부러웠습니다. 양한광 이사장께서 Aikou 선생님을 소개하면서 2014년 폭풍 와중에도 우리나라 위암학회에 와 주신 점을 고맙다고 하셨는데, Aikou 선생님 강의도 이에 대한 언급이 있었습니다. 남자의 약속을 지킬 수 있어서 다행이라고 하면서 emergency dinner 사진을 보여주셨습니다. ^^

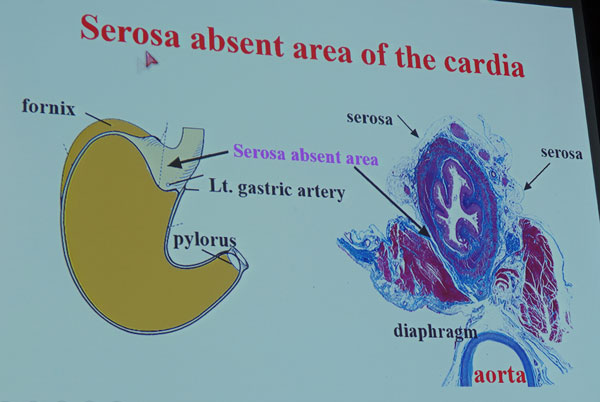
EGJ을 터널 입구에 비교한 점은 재미있었습니다.
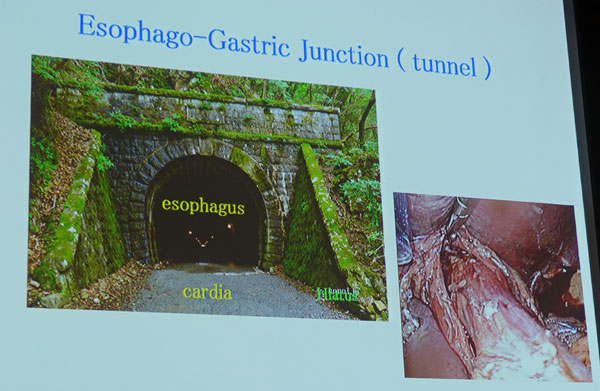
EGJ 의 일부는 serosa가 없습니다.
![]() 3. Symposium 2. Expanded indication of ESD
3. Symposium 2. Expanded indication of ESD
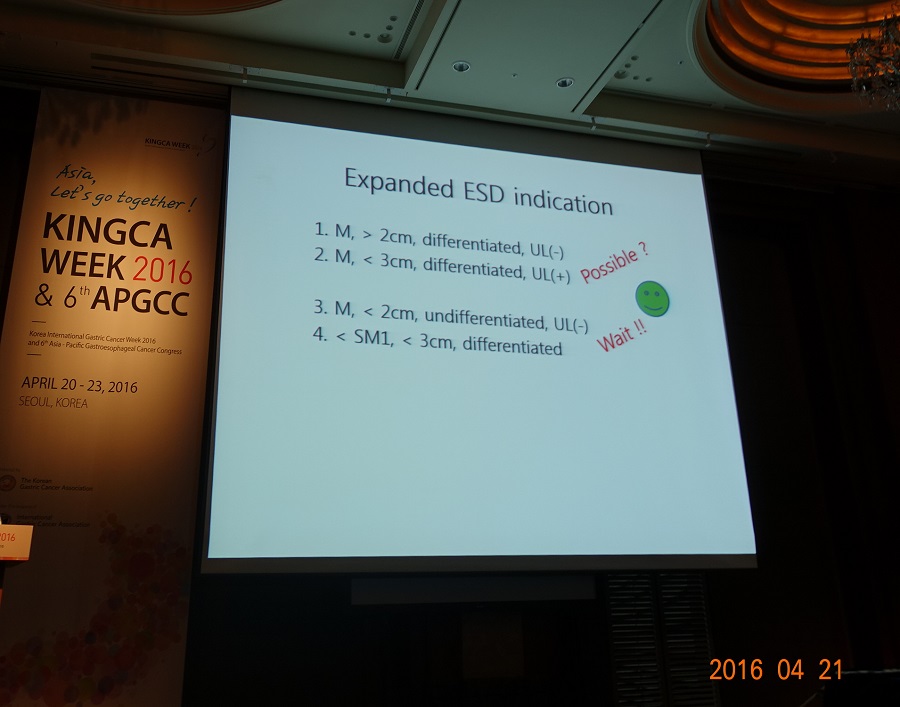
1) Expanded indication for differentiated-type EGC (최일주)
최일주 선생님은 최근 발표된 동경암센터의 longterm data로 이야기를 시작하셨습니다 (Suzuki. Gastric Cancer 2016). (이준행 comment: 사실 너무 성적이 좋아서 selection bias가 많을 것으로 판단되는 자료입니다.)

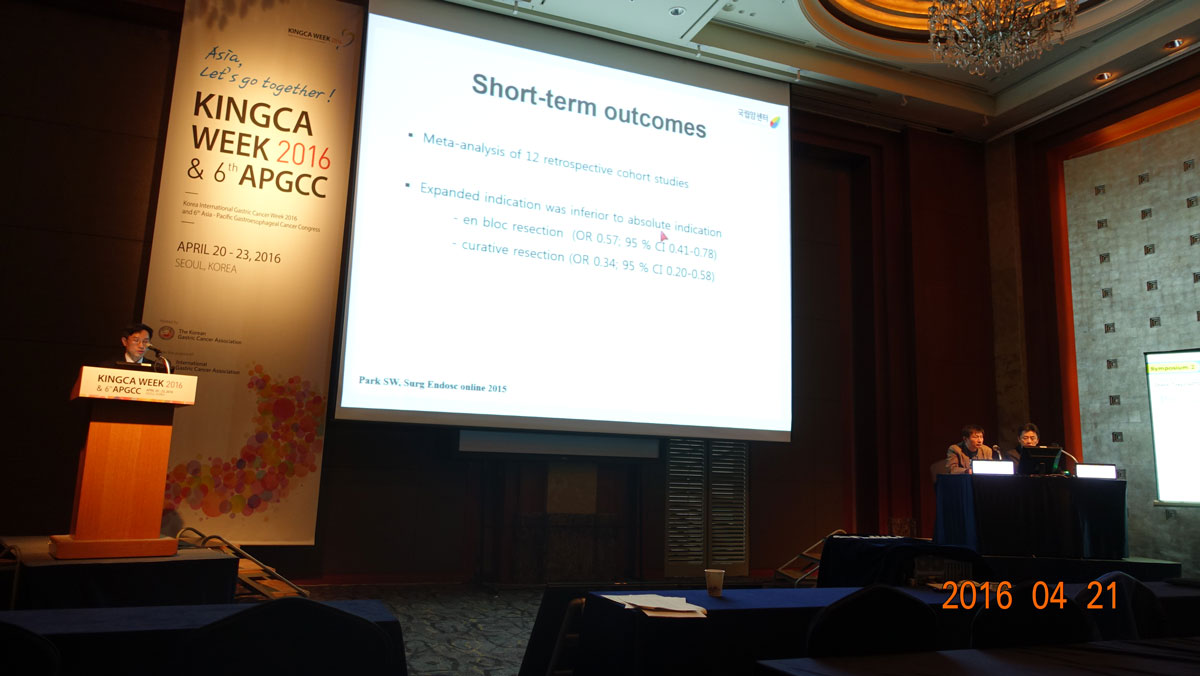
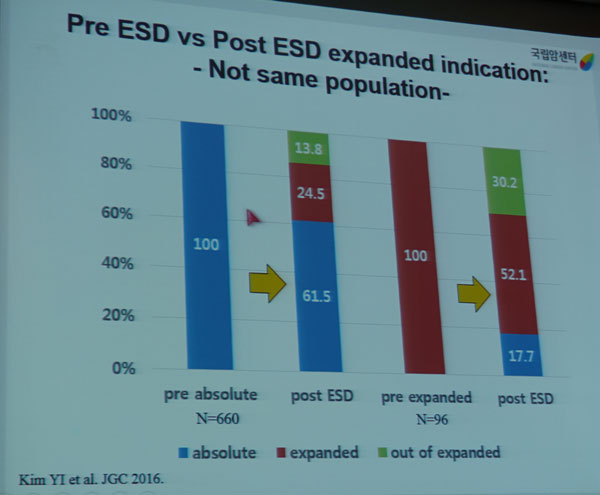
최근 Journal of Gastric Cancer에 발표하신 자료를 상세히 설명해 주셨습니다 (Kim YI. J Gastric Cancer 2016).
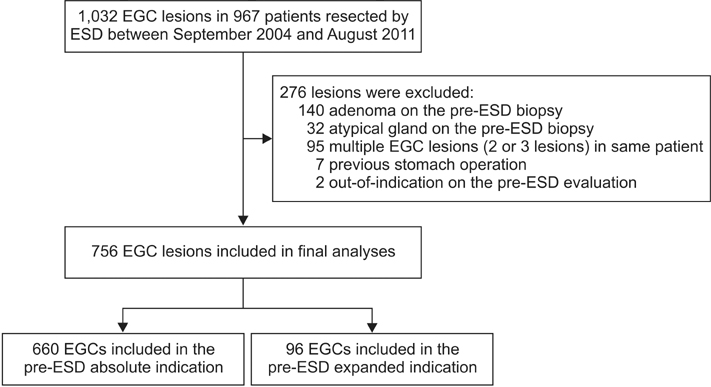
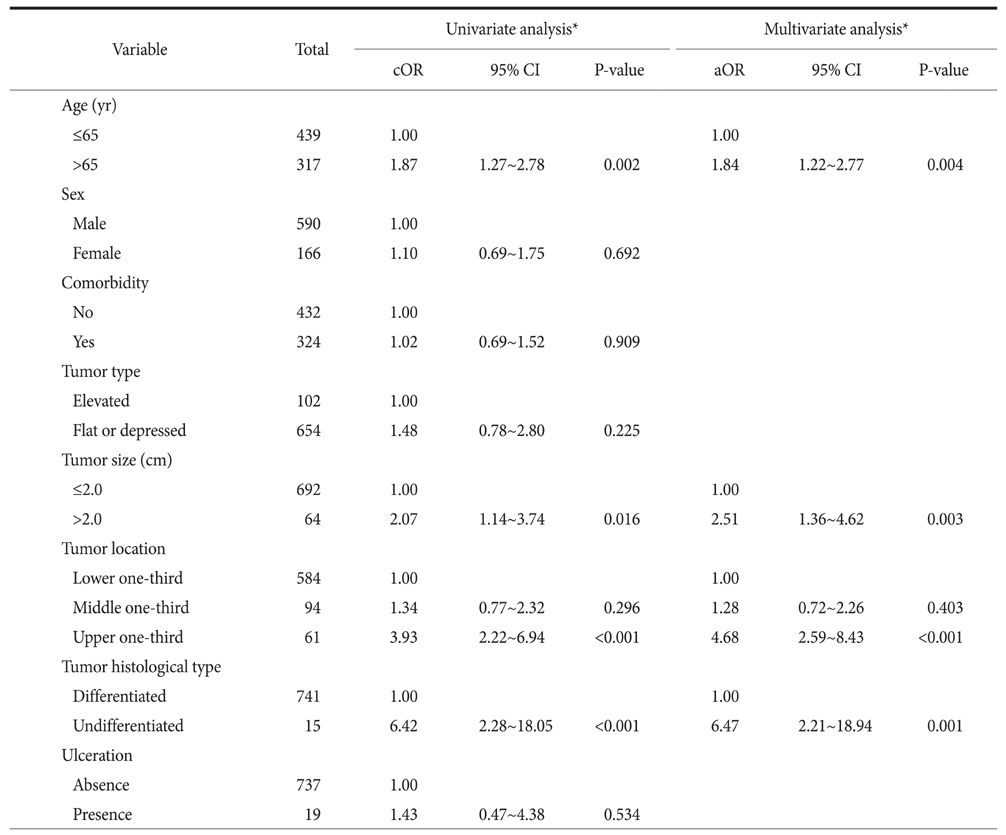
PURPOSE: Early gastric cancer cases that are estimated to meet indications for treatment before endoscopic submucosal resection are often revealed to be out-of-indication after the treatment. We investigated the short-term treatment outcomes in patients with early gastric cancer according to the pretreatment clinical endoscopic submucosal resection indications. MATERIALS AND METHODS: We retrospectively reviewed the medical records of patients with early gastric cancer that met the pretreatment endoscopic submucosal resection indications, from 2004 to 2011. Curative resection rate and proportion of out-of-indication cases were compared according to the pre-endoscopic submucosal resection indications. Pre-endoscopic submucosal resection factors associated with out-of-indication in the final pathological examination were analyzed. RESULTS: Of 756 cases, 660 had absolute and 96 had expanded pre-endoscopic submucosal resection indications. The curative resection rate was significantly lower in the patients with expanded indications (64.6%) than in those with absolute indications (81.7%; P<0.001). The cases with expanded indications (30.2%) were revealed to be out-of-indication more frequently than the cases with absolute indications (13.8%; P<0.001). Age of >65 years, tumor size of >2 cm, tumor location in the upper-third segment of the stomach, and undifferentiated histological type in pre-endoscopic submucosal resection evaluations were significant risk factors for out-of-indication after endoscopic submucosal resection. CONCLUSIONS: Non-curative resection due to out-of-indication occurred in approximately one-third of the early gastric cancer cases that clinically met the expanded indications before endoscopic submucosal resection. The possibility of additional surgery should be emphasized for patients with early gastric cancers that clinically meet the expanded indications.

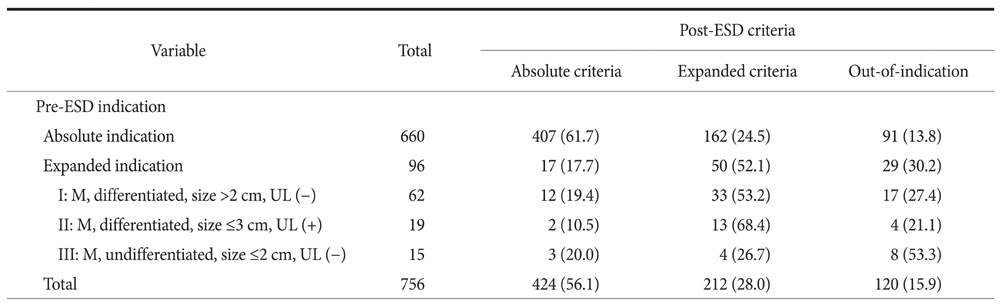
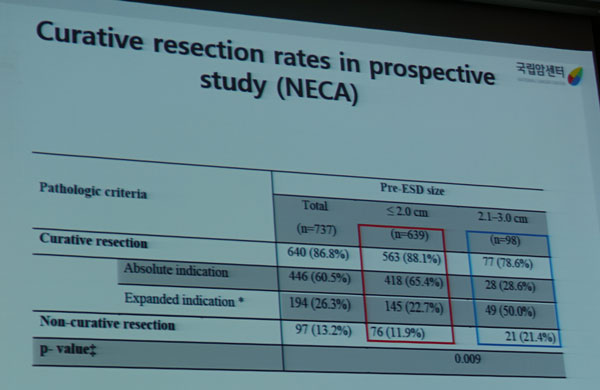
국립암센터 자료에서 확인할 수 있듯이 ESD 전 absolute indication으로 판단된 경우와 ESD 전 expanded indication으로 판단된 경우의 curative resection rate는 상당한 차이가 있습니다. 다기관 prospective registry인 NECA 연구에서도 거의 비슷한 측면이 있었습니다.
이러한 discrepancy를 보이는 이유는 상당히 많습니다. 최일주 선생님은 아래와 같은 점들을 지적하셨습니다.

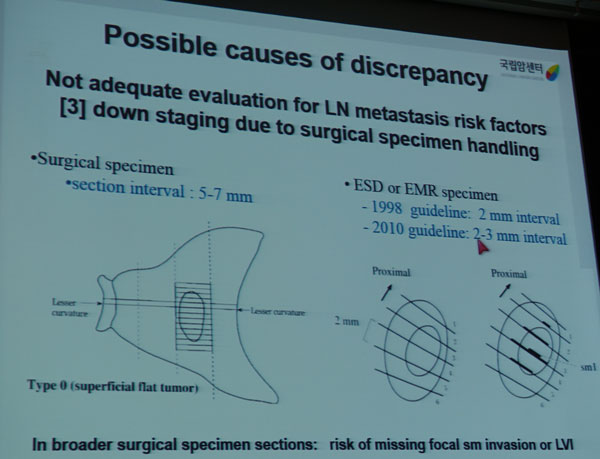
최일주 선생님에 따르면 국립암센터에서는 expanded indication criteria에 해당하면 immunohistochemistry 검사를 한다고 합니다. 다음은 이번 강의의 결론 슬라이드입니다. 전적으로 동의합니다. 이 부분은 전적으로 전문가의 영역이라고 생각합니다. 아무나 할 일이 아닙니다.
"Pre ESD expanded indication can be applied in specialized centers with experienced endoscopists, surgeons, and pathologists after providing detailed information to the patients."
좌장이셨던 Gotoda 선생님은 일본에서는 모든 ESD 샘플에 대한 immunohistochemical staining을 추천한다고 comment하셨습니다. 그러나 병리학자들 사이의 관찰자가 크기 때문에 lymphatic involvement에 대한 병리 결과는 incomplete하다고 덧붙였습니다. 동의합니다.
★ [이준행 comment] 최일주 선생님께서는 이번 발표를 통하여 Pre-ESD expanded indication 증례들과 Post-ESD expanded indication 증례는 서로 다르다는 점을 명확히 설명해 주셨습니다.
저도 pre-ESD expanded indication과 post-ESD expanded indication이 서로 다르다는 점을 발표한 바 있습니다 (Lee JH. Surg Endosc 2015 - Epub). 저는 이런 현상을 Diagnostic Group Classificaion이라는 개념으로 설명하고 있습니다.
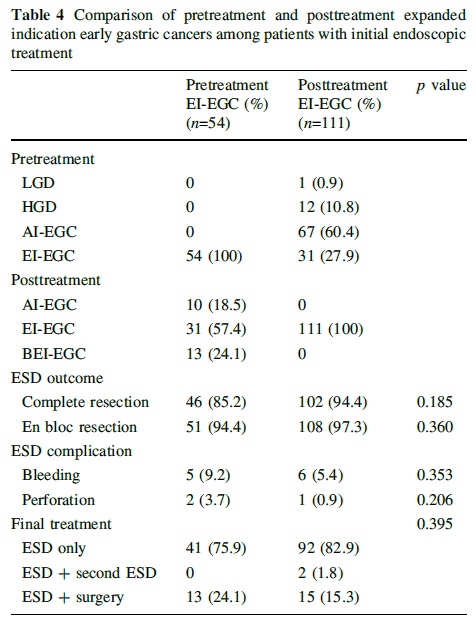
실제로 ESD 전 absolute indication이라고 생각하였던 환자의 상당수는 시술 후 expanded indication 혹은 beyond expaded indication으로 바뀌었습니다. 아래는 2012년 삼성서울병원의 자료입니다 (Lee JH. Surg Endosc 2015 - Epub).

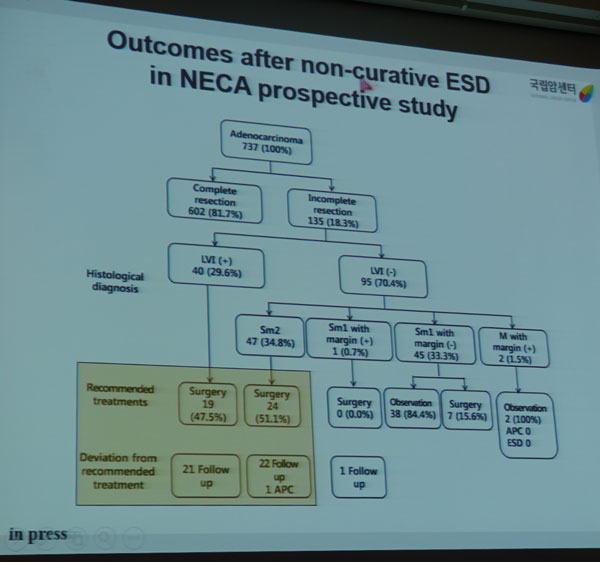
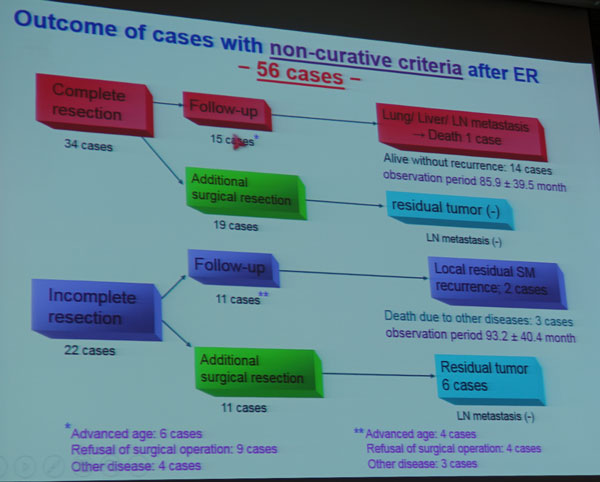
Submission 상태인지라 그림을 옮길 수 없었지만 최일주 선생님께서는 "Outcome of ESD alone without additional surgery after non-curative resection was poorer than those of initial surgery"라는 점을 강조하셨습니다. 이는 일본의 결과와는 상당히 다른 것인 반면 삼성서울병원의 결과(아래 그림)와는 거의 유사합니다 (EndoTODAY noncurative resection).

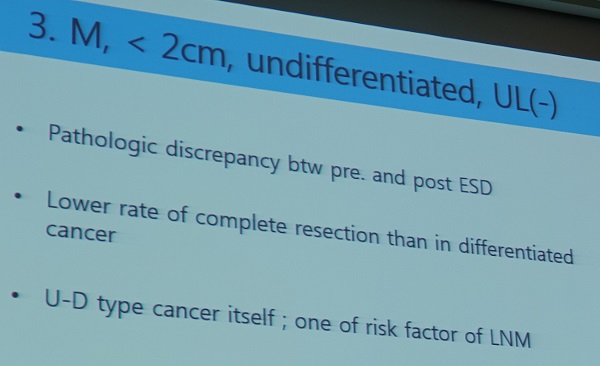
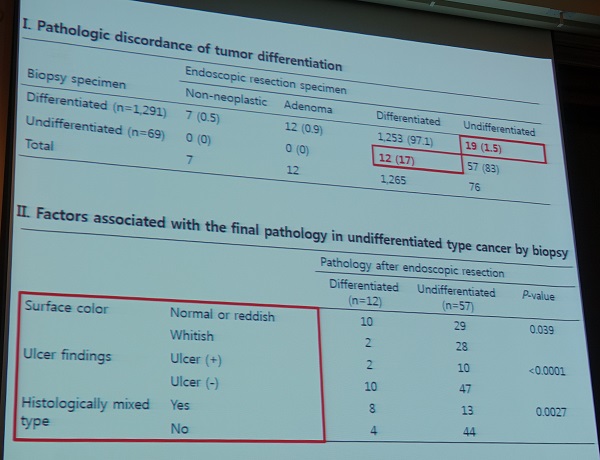
2) Expanded indication for undifferentiated-type EGC (Oka, Hirishima U, Japan)
Oka 선생님은 2014년 Surgical Endoscopy에 undifferentiated type EGC의 내시경 치료 성적을 보고하였습니다 (Oka. Surg Endosc 2014). 제가 EndoTODAY에 아래와 같이 정리하여 소개한 바 있습니다.
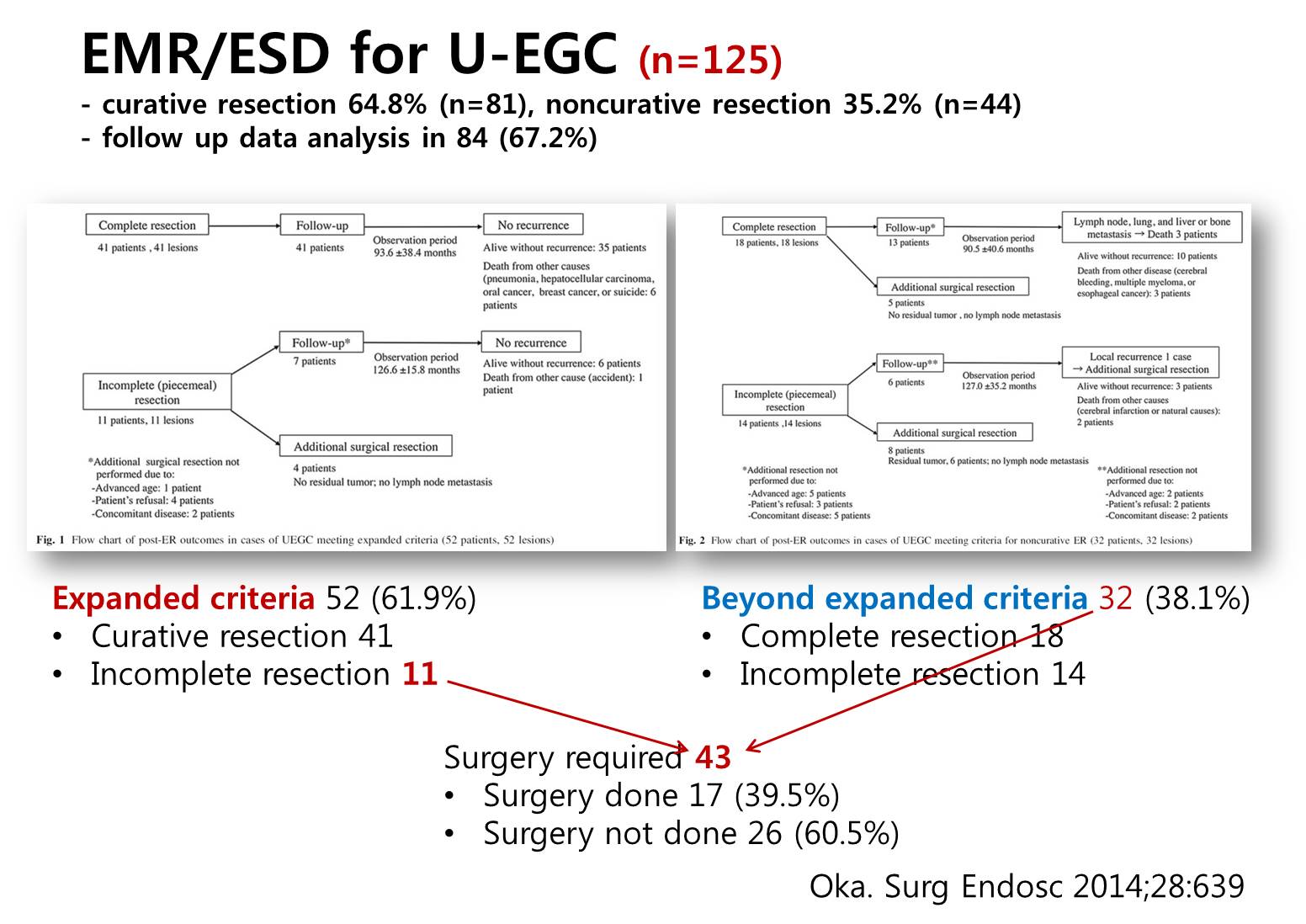
이번 강의에서 Oka 선생님의 같은 대상 환자의 최근 update를 보여주셨습니다.

Oka 선생님은 일본에서 조기위암 내시경치료 web registry에 2010년부터 2012년까지 시술한 환자 10,821명이 등록되어 있는데 곧 결과가 나온다는 점을 설명하면서 강의를 마쳤습니다.
저는 우리나라에서는 아직 undifferentiated cancer는 수술로 치료해야한다고 생각하는 surgeon이 많은데 일본은 어떤지 질문하였습니다. Oka 선생님은 Hiroshima U에서는 small undifferentiated EGC에 대한 내시경 치료에 대하여 외과의사들도 동의한다고 답하였습니다. Gotoda 선생님은 ESD candidate 선정할 때 늘 외과의사와 상의하기 때문에 서로 의견이 다르지는 않다고 언급하셨습니다. 다만 poorly differentiated와 signet ring cell carcinoma는 매우 다르다는 점, 내시경으로 볼 때 1.5 cm 이하만을 시술할 것을 comment하였습니다. 이점에 대해서 Oka 선생님은 2.0 cm라고 말했는데, 저는 1.0 cm이 좋겠다고 commnent 하였습니다 (참고자료 - 2016년 KINGCA 이준행 구연). 일전에 연세대학교 윤영훈 교수님도 1.0 cm를 기준으로 한다는 의견을 주신 바 있습니다.
3) Surgeons' view on expanded indication of ESD (동아대학교 김민찬)
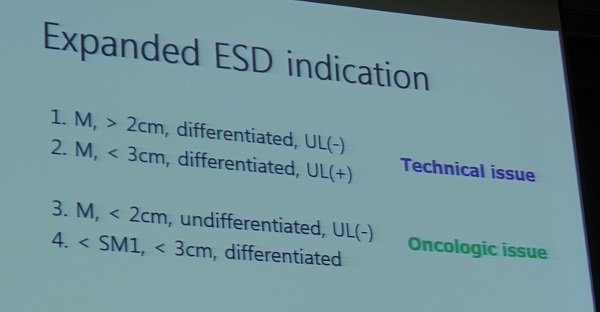
김민찬 교수님은 아래와 같은 세 가지 topic을 제시하면서 expanded indication을 technical issue와 oncologic issue로 나누었습니다.
- SM cancer and small UD cancer
- Mixed histology mucosal cancer
- Poorly differentiated component in the SM layer of differentiated EGC
김민찬 교수님은 undifferentiated type EGC에 대한 내시경치료에 대하여 상당히 우려하는 입장을 보였습니다.
특히 2016 Ann Surg 서울대 논문을 보여주신 부분은 상당히 흥미로웠고 충격적이었습니다.
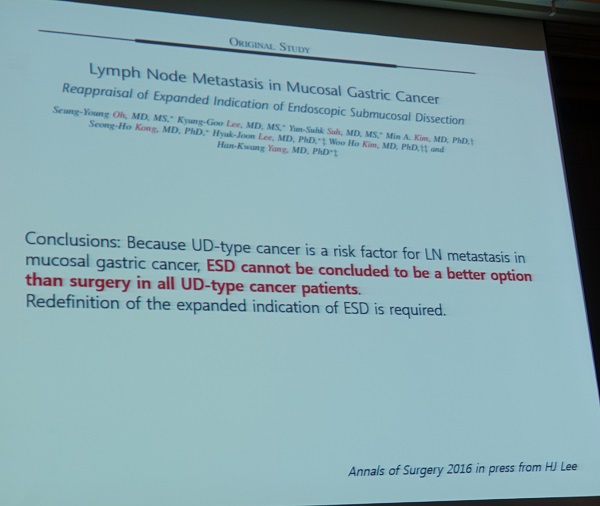
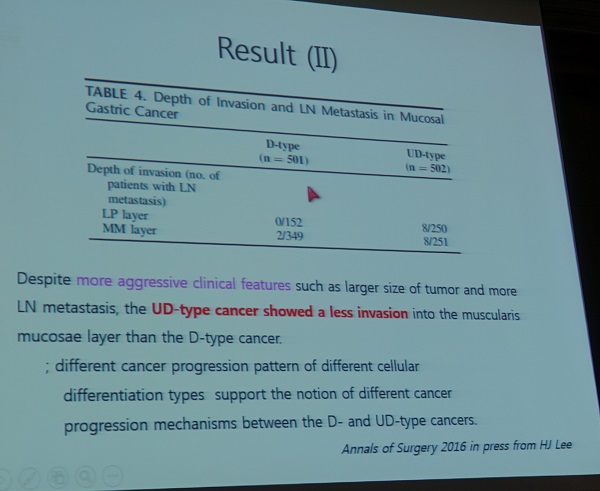
김민찬 교수님의 결론 슬라이드는 현재 우리나라 외과의사의 일반적인 입장을 대변하는 것 같습니다. 충분히 타당한 지적이라고 생각합니다. Undifferentiated type에 대해서는 더욱 그러합니다.
4) Gastroenterologist's view on expanded indications (전남대학교 이완식)
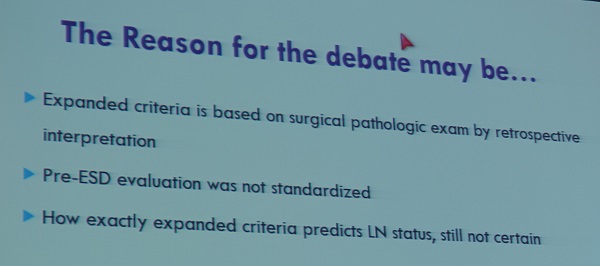
이완식 교수님은 아래 3가지의 debates를 제시하였습니다.
- Gross findings (size, gross appearance) - lack of accuracy
- Pathology - discrepancy
- Undifferentiated type EGC
Gross finding이 depth of invasion을 정확히 예측하기 어렵습니다. 아래 세 사진을 보면 gross 모양을 보고 depth of invasion을 짐작한다는 것이 얼마나 어려운지 실감할 수 이습니다.

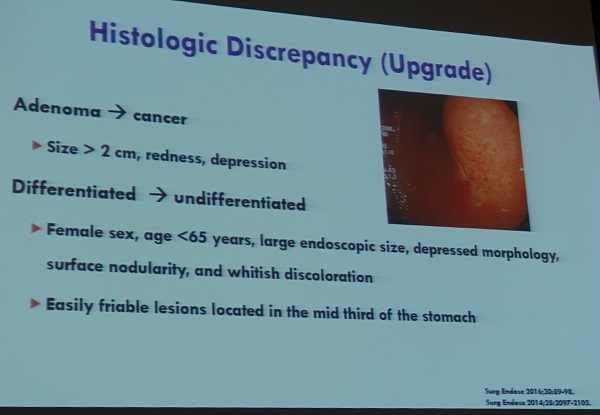
Histologic discrepancy (upgrade)도 문제입니다. 대부분 조직검사에서 differentiated type이 수술병리에서는 undifferentiated type으로 나오는 것이 문제입니다.
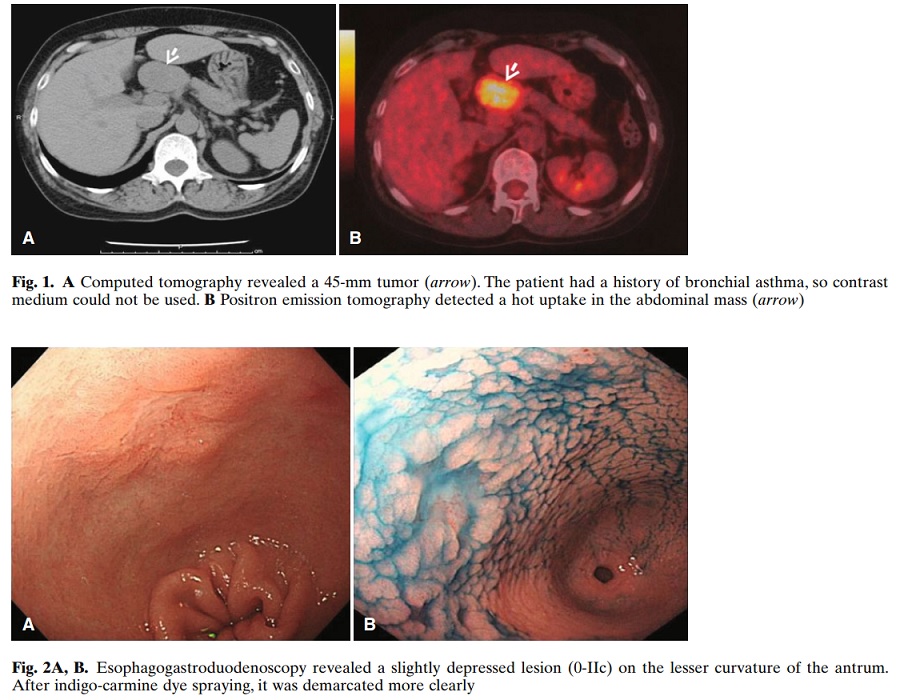
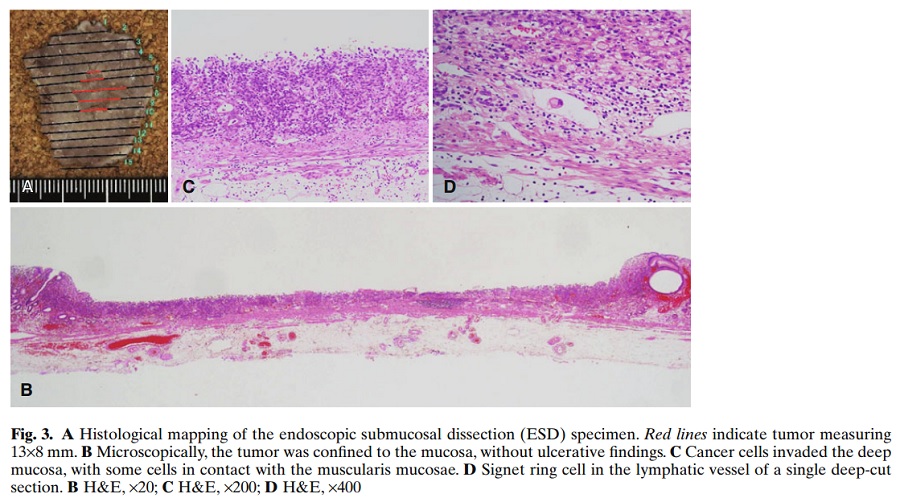
Expanded indication에 해당하는 undifferentiated type EGC에 대하여 curative resection을 하였으나 림프절 전이가 있었던 교훈적인 증례입니다 (Hirasawa. Gastric Cancer. 2010). 13mm mixed type이었습니다 ("a poorly differentiated adenocarcinoma and signet ring cell carcinoma confined to the mucosa without lymphatic-vascular capillary involvement or ulceration"). Routine ESD 병리검사에서 lymphatic invasion이 없어서 엄청 추가 cut를 해 보았더니 그제서야 lymphatic involvement를 발견했다는 것이었습니다 (" 60 additional deep-cut sections from the resected specimen were performed, with one section showing lymphatic involvement in the mucosa on hematoxylin and eosin staining").
SRC는 내시경으로 크기 및 경계 판정이 어렵고, 결국 ESD에서 lateral margin 양성으로 나타난다고 해석됩니다. 이완식 교수님은 SRC를 병리학적 growth pattern을 바탕으로 expanding type과 infiltrative type으로 나누어 분석한 연세대학교 강남세브란스병원의 자료를 인용하였습니다 (Kim H. Gut Liver 2015).
The expanding type was defined as a tumor that had a margin that was clearly lined from the non-neoplastic mucosa, that is, epithelial spreading pattern.
The infiltrative type was defined as a tumor that showed diffuse spreading tumor cells, that is, supepitheial spreading pattern.
Signet ring cell carcinoma intramucosal spreading types. Expansive type. (A) Tumor cells (circle) were exposed at a superficial part of the mucosa. A tumor with a margin was distinct from the nonneoplastic mucosa (H&E stain, ×40). (B) Tumor cells (circles) were located in the intermediate or deeper parts of the nonneoplastic mucosa. Diffuse-spreading tumor cells were evident (H&E stain, ×40).
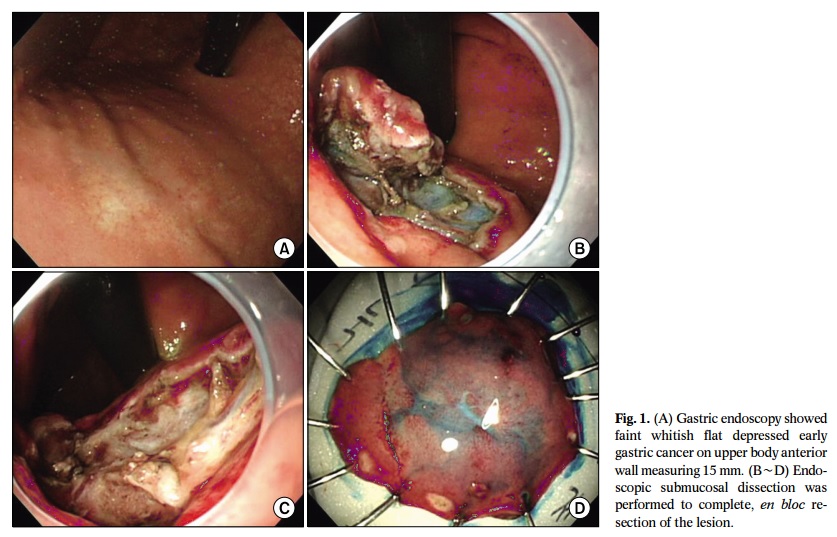
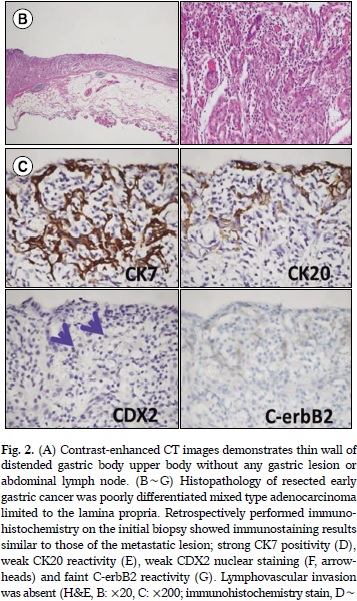
2016년 대한상부위장관헬리코박터학회지에 보고된 증례도 소개하셨습니다 (Son DJ. KJHUGR 2016). Mixed type adenocarcinoma with poorly differentiated histology, 15 mm 크기, lamina propria까지 침윤된 EGC IIb였고 시술도 잘 되었는데 7년 후 다발성 재발을 보였습니다.
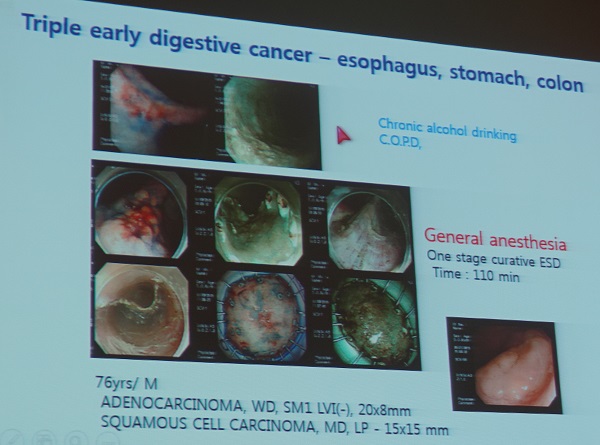
이완식 교수님은 Individual approach 를 강조하셨습니다. 식도, 위, 대장에 암이 있었는데 모두 내시경으로 치료한 증례와 반대로 ESD 후 noncurative resection으로 나와 수술을 하였는데 안타깝게도 postoperative complication으로 사망한 증례를 소개하셨습니다.
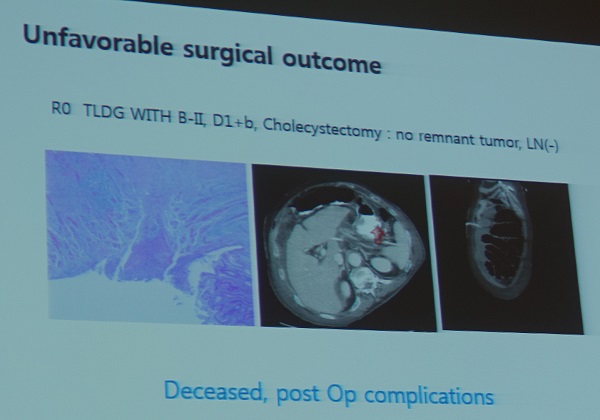
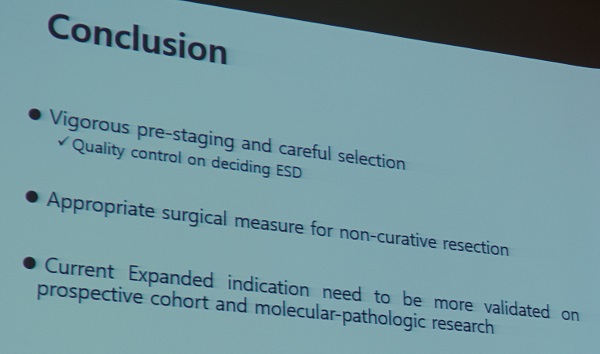
다음 두 장은 이완식 교수님의 conclusion입니다.
배재문 선생님은 연자께서 말씀하신 no standardization before ESD 이외에도 technique of ESD의 표준화도 중요하다고 comment 하셨습니다. Video 혹은 picture review program이 있는지 문의하셨는데 매우 타당한 질문이었다고 생각합니다.
![]() 4. 런천
4. 런천
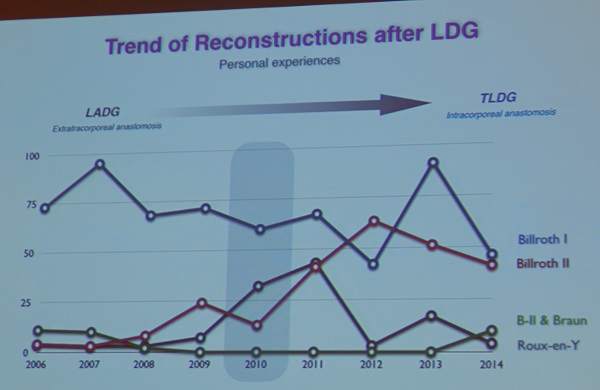
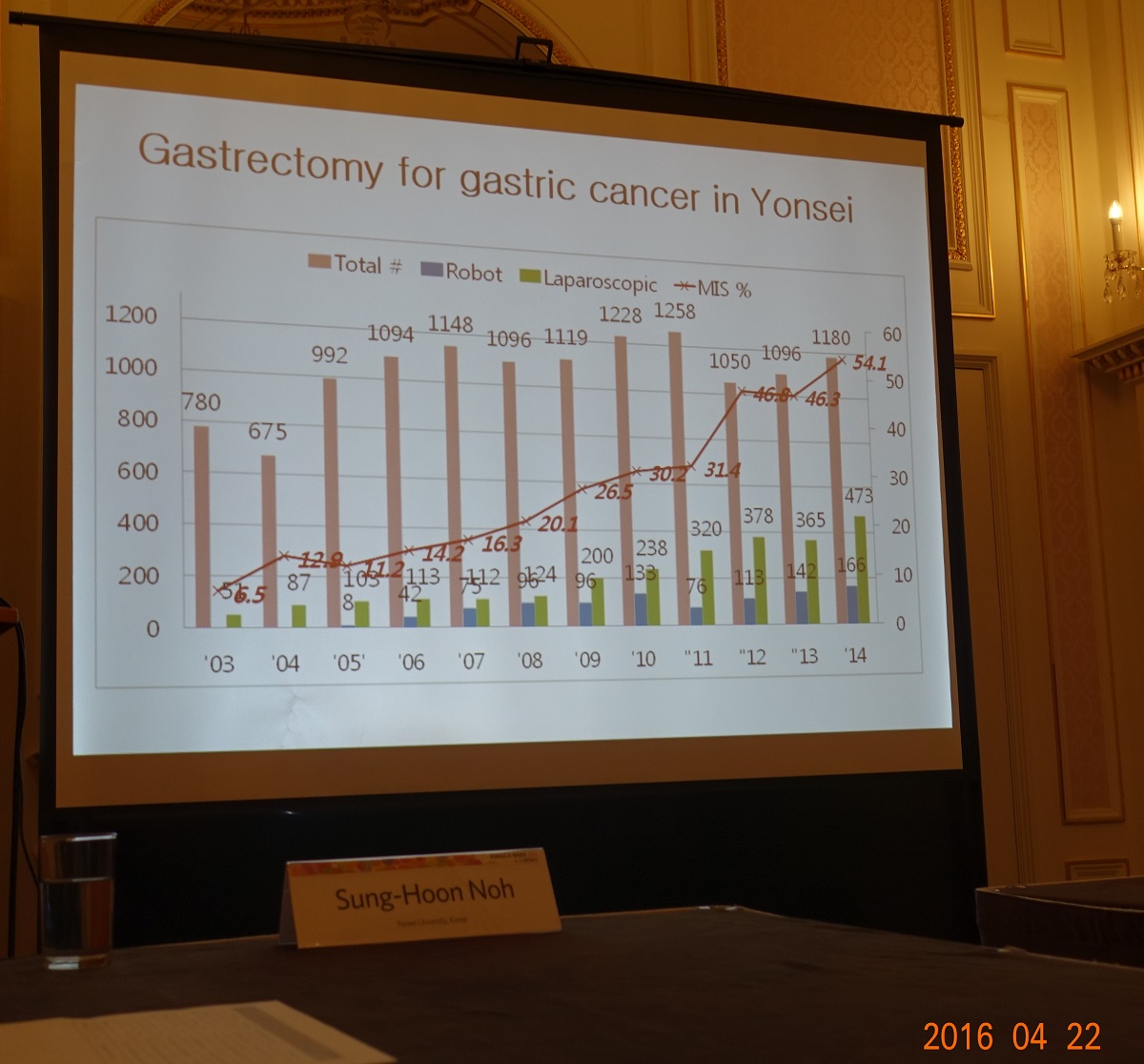
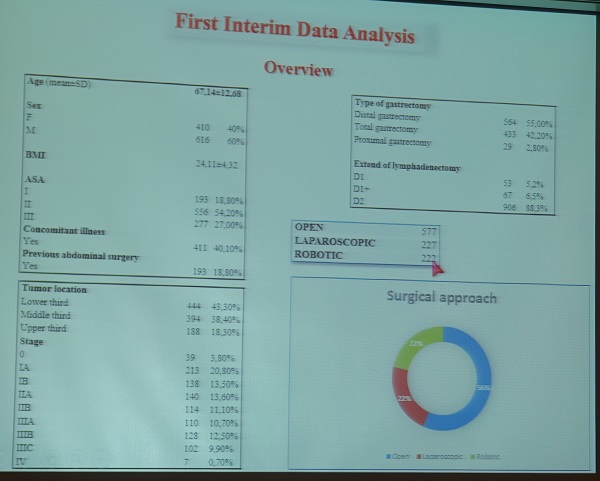
아주대 한상욱 선생님께서 수술 술기에 대하여 강의하셨습니다. 내과 의사로서는 아래의 내용을 주의깊게 살펴보았습니다.

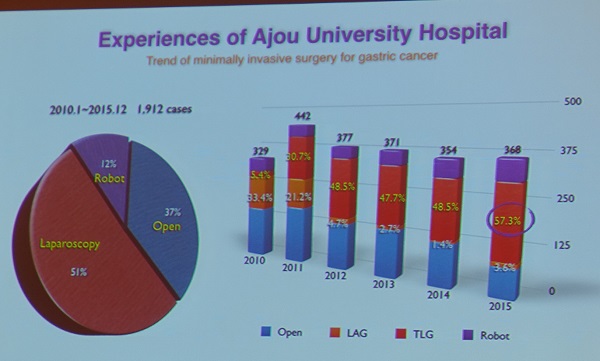 절반 이상을 복강경으로 시술하고 있다고 합니다. 로봇까지 합하면 3/4 이상이 less invasive surgery가 적용되고 있습니다.
절반 이상을 복강경으로 시술하고 있다고 합니다. 로봇까지 합하면 3/4 이상이 less invasive surgery가 적용되고 있습니다.
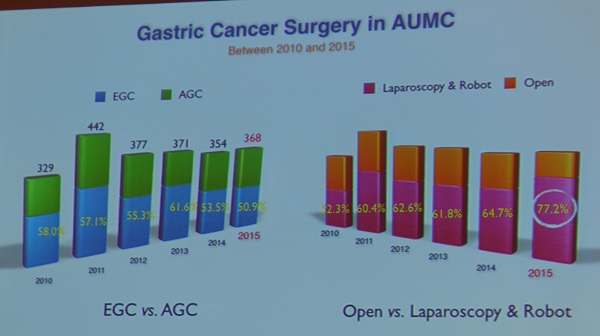 수술 환자 중 조기위암이 줄고 있다는 흥미로운 데이타입니다. 상당수의 조기위암이 내시경으로 치료되고 있어서 외과의사에게까지 가지 않는 모양입니다. 환자 입장에서는 좋은 일입니다.
수술 환자 중 조기위암이 줄고 있다는 흥미로운 데이타입니다. 상당수의 조기위암이 내시경으로 치료되고 있어서 외과의사에게까지 가지 않는 모양입니다. 환자 입장에서는 좋은 일입니다.
![]() 5. Endoscopy Session: Gastroscopy for surgeons (좌장: 정훈용, Jimmy So)
5. Endoscopy Session: Gastroscopy for surgeons (좌장: 정훈용, Jimmy So)
1) Education and training of endoscopy for surgeons: why? (가톨릭대학교 송교영)
저는 아래와 같은 comment를 했습니다.
I am CEO, chief endoscopy officer or chief education officer of the endoscopy unit at Samsung Medical Center and I am in charge of endoscopy training. I think insertion technique is just 10% of knowledge or experience required for independent endoscopist. More than 90% is interpretation of findings. Outpatient endoscopy and introperative endoscopy is quite different. I am very positive about surgeon endoscopists, but I worry a lot about lack of case studies for resident doctors. I propose to work together. Please send your resident doctors to the endoscopy conference usually held every week in every training hospital.
2) Endoscopy in gastric cancer (Takuji Gotoda, Nihon university, Japan)
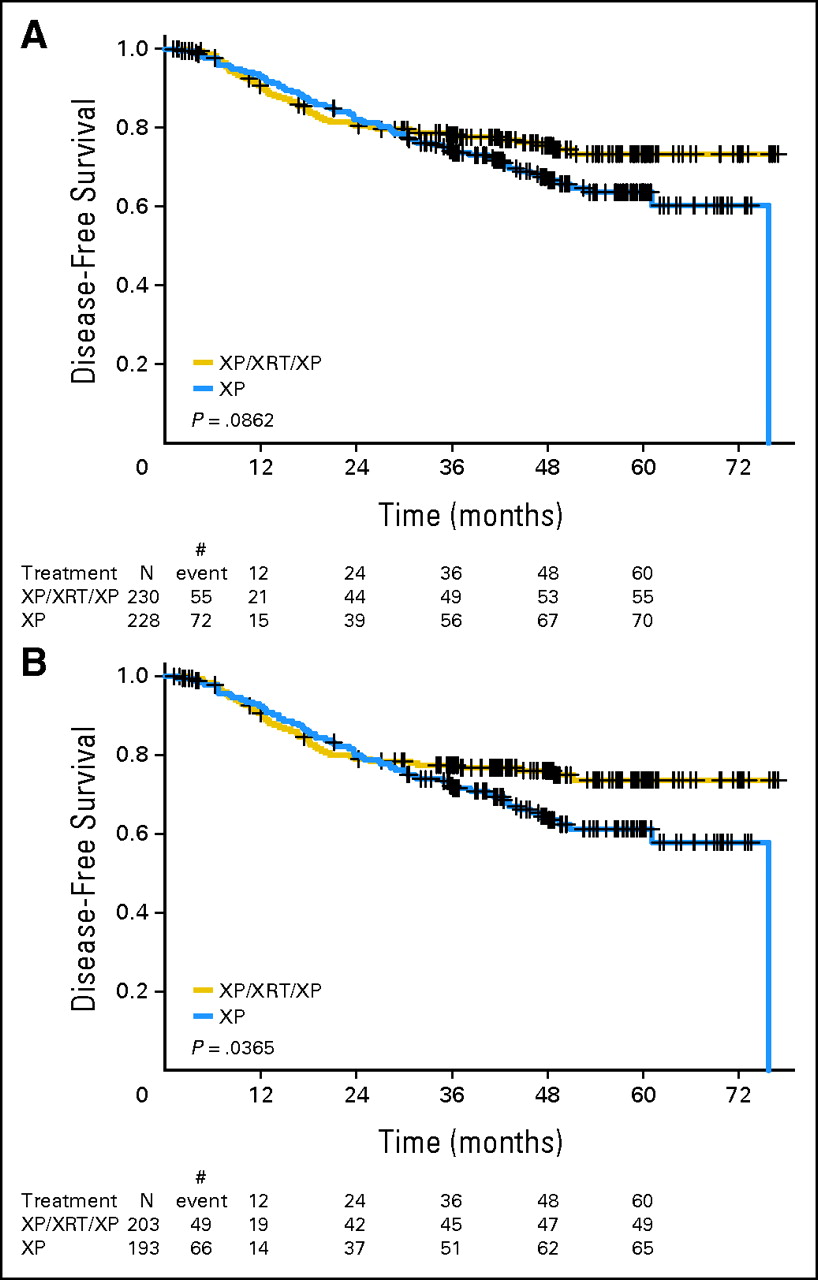
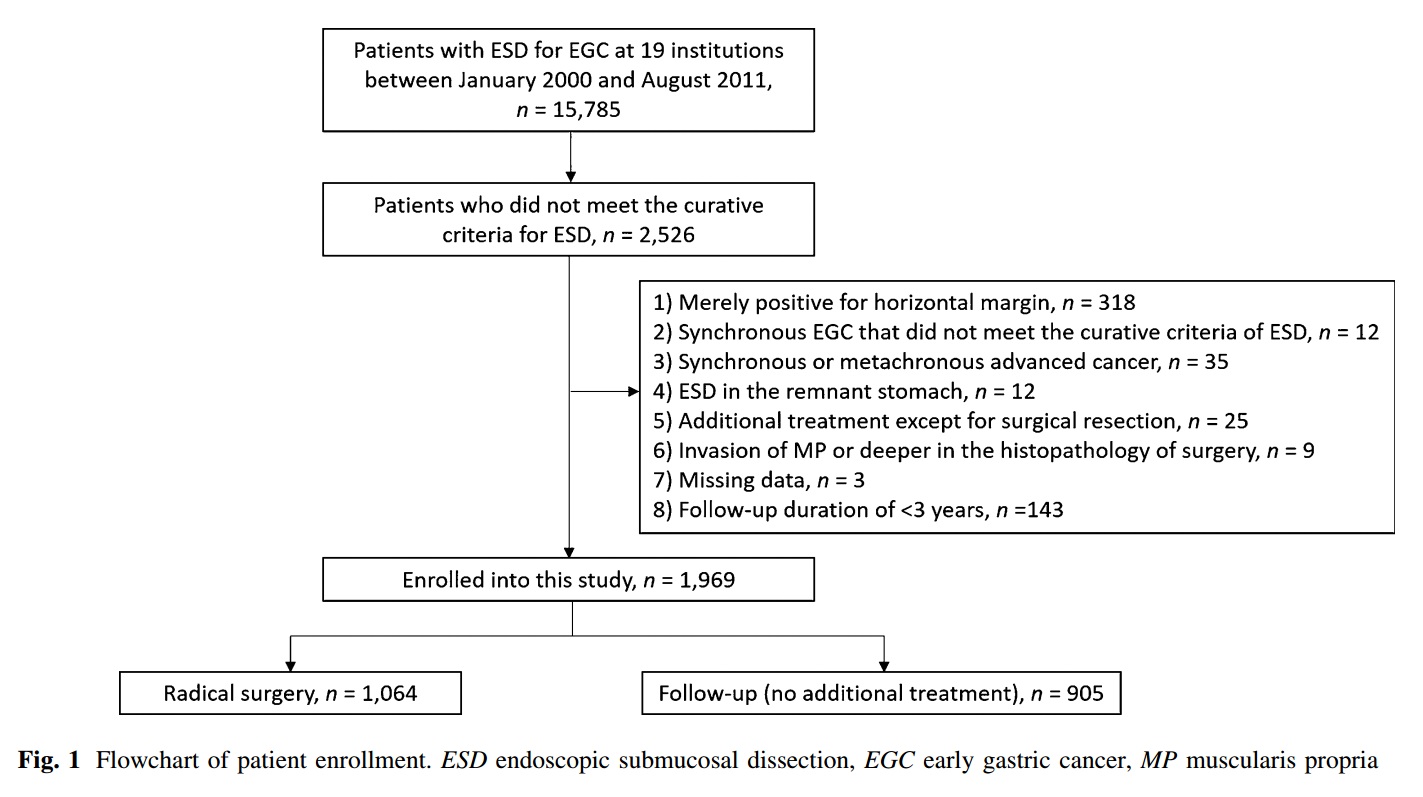
Gotoda 선생님은 2016년 4월 20일 Epub된 뜨끈뜨끈한 자료를 중심으로 강의를 하셨습니다 (Hatta W. J Gastroenterol 2016 - Epub). 일본 19개 기관의 자료를 모은 다기관 후향적 연구였습니다.
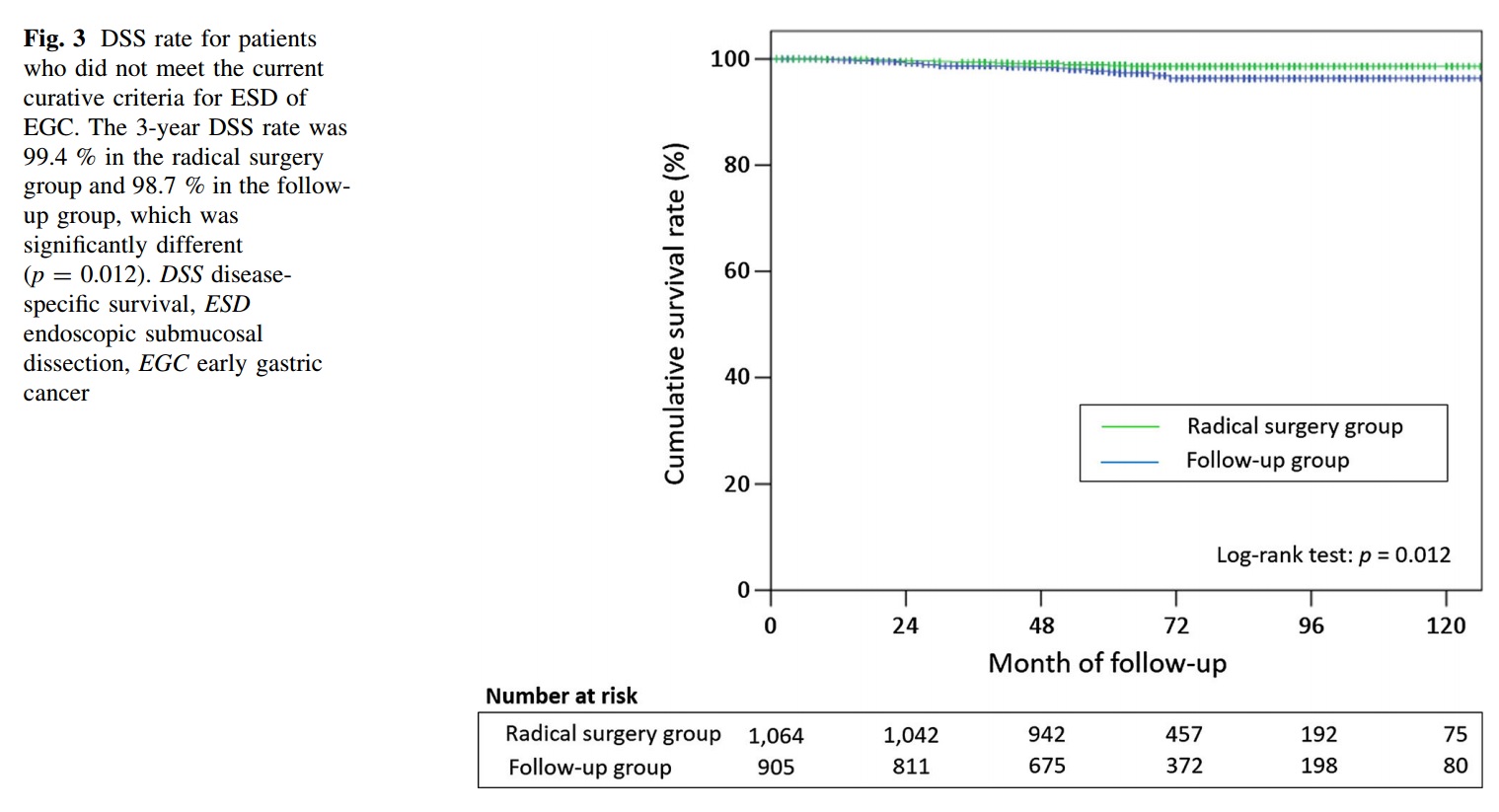
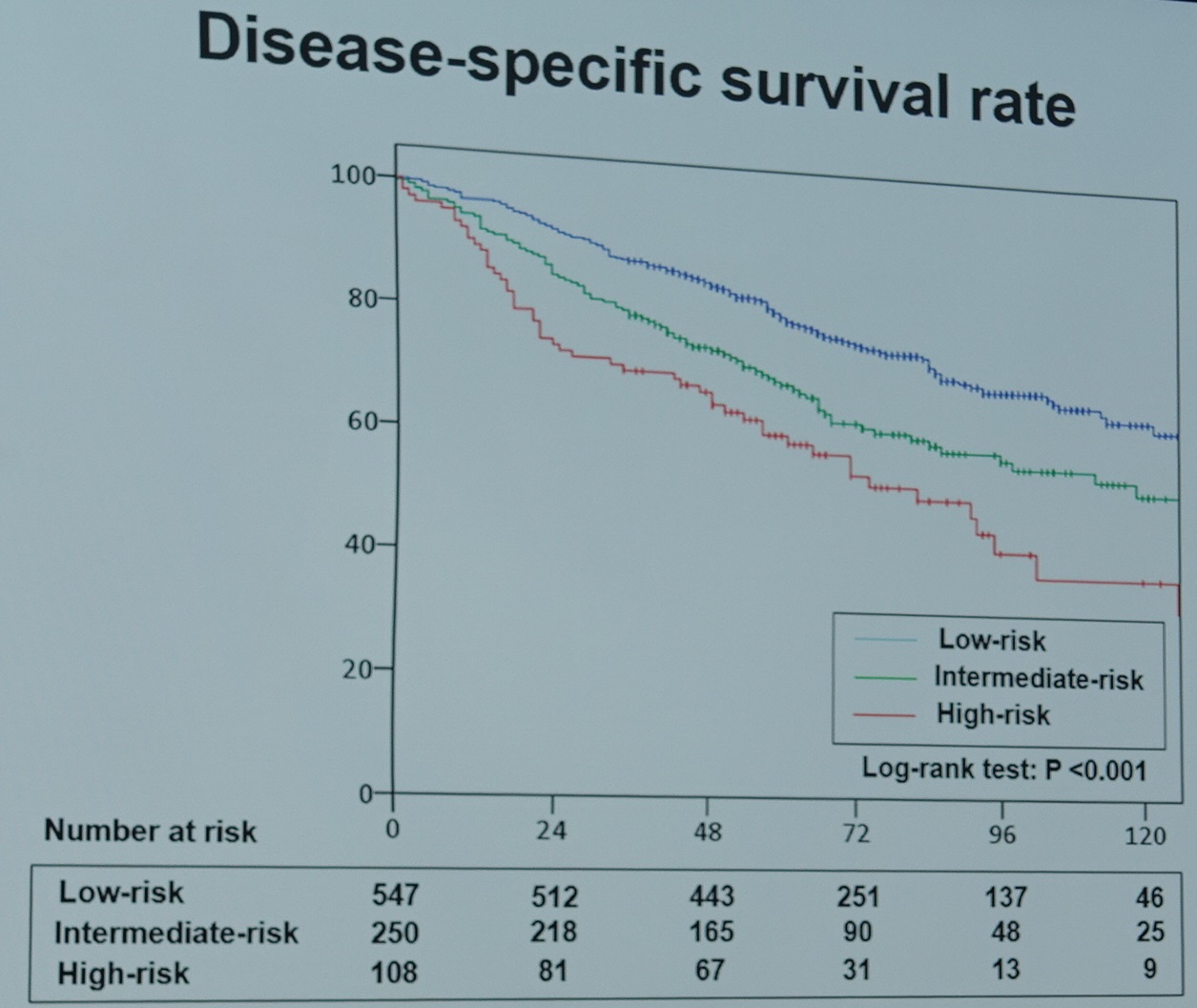
RESULTS: Overall survival (OS) and disease-specific survival (DSS) were significantly higher in the radical surgery group than in the follow-up group (p < 0.001 and p = 0.012, respectively). However, the difference in 3-year DSS between the groups (99.4 vs. 98.7 %) was rather small compared with the difference in 3-year OS (96.7 vs. 84.0 %). LNM was found in 89 patients (8.4 %) in the radical surgery group. Lymphatic invasion was found to be an independent risk factor for recurrence in the follow-up group (hazard ratio 5.23; 95 % confidence interval 2.01-13.6; p = 0.001).
CONCLUSIONS: This multi-center study, representing the largest cohort to date, revealed a large discrepancy between OS and DSS in the two groups. Since follow-up with no additional treatment after ESD may be an acceptable option for patients at low risk, further risk stratification is needed for appropriate individualized treatment strategies.

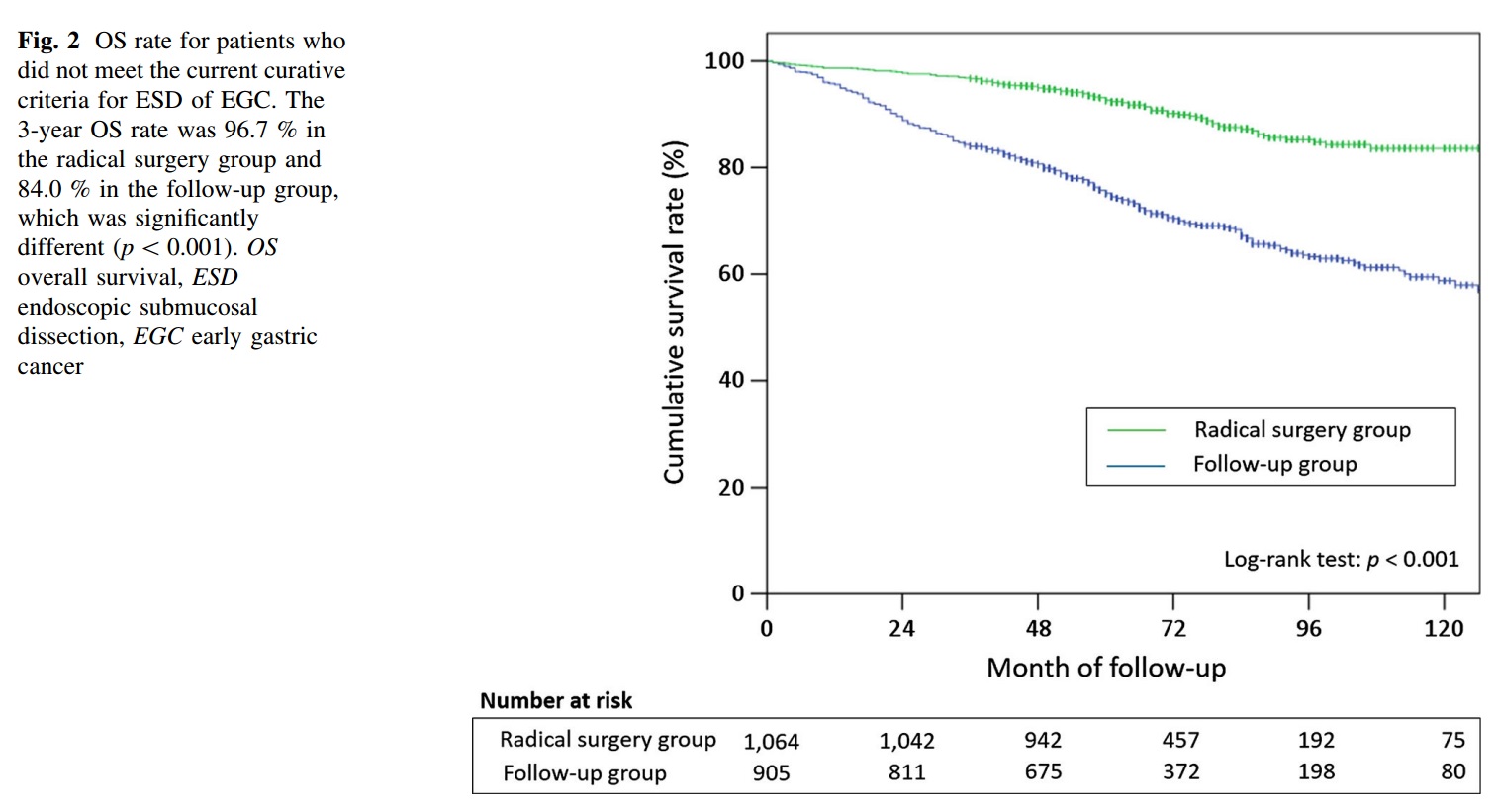

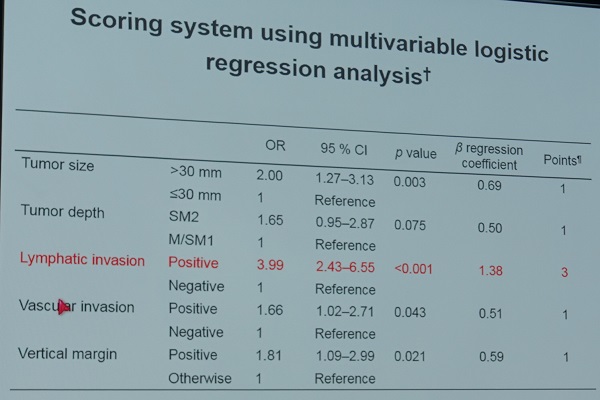
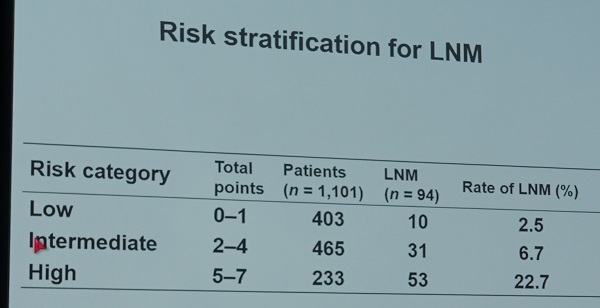
Hatta W. J Gastroenterol 2016 논문의 마지막은 다음과 같았습니다. "Although radical surgical resection is currently indicated for these patients, we suggest that follow-up with no additional treatment after ESD may be an acceptable option for patients at low risk. Consequently, further risk stratification is needed for appropriate individualized treatment strategies." 이미 이에 대한 분석을 마친 것 같고 강의 중에 일부 자료를 소개하셨습니다. eCura system이라 불리는 scoring system입니다. 다른 위험인자보다 lymphatic invasion에 3배의 가중치가 주어졌습니다.
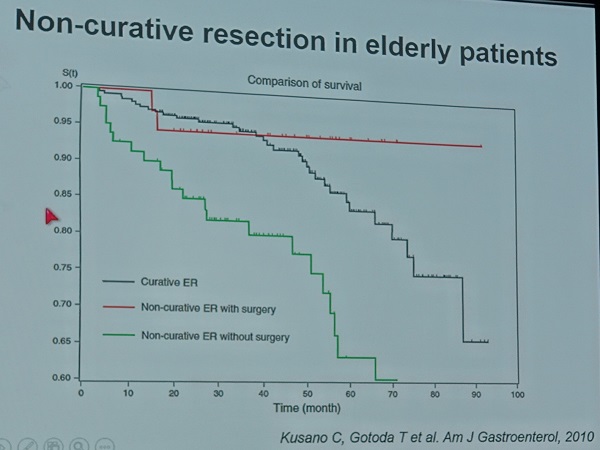
Gotoda 선생님은 Kusano의 유명한 논문도 함께 소개하였습니다. 수술을 받지 않은 군에서 survival이 훨씬 못하다는 유명한 data입니다. Elderly를 대상으로 한 연구였기 때문인지 수술군과 비수술군의 차이가 더욱 현저합니다.
Gotoda 선생님은 "Further innovation is still demanded"라는 말로 강의를 마무리하였습니다. 멋진 강의였습니다.

![]() 6. Meet the professor - Surgical treatment for AGC based on oncologic principles (연세대 노성훈)
6. Meet the professor - Surgical treatment for AGC based on oncologic principles (연세대 노성훈)
Unnecessary manipulation을 피하는 것이 좋습니다. Wound healing과 metastasis의 process가 비슷하기 때문입니다.
Additional paraaortic lymph node dissection이 표준 D2 LN dissection보다 우월성은 없었습니다.
D2 dissection이 표준이 되었지만 아직 서구에서는 limited dissection이 더 많이 행해지고 있습니다.
일반적으로 LN 14v는 distant metastasis로 간주되지만 right epiploic node (#6) 양성자에서는 도움이 될 것으로 생각됩니다. (2010(?) 가이드라인부터 LN 14v는 위암의 위치와 무관하게 metastasis로 간주되고 있다고 합니다.)
Is splenic hilar lymph node dissection without splenectomy possible? 두 가지 술기가 있습니다. 과거에는 mobilizatin 법을 사용했지만 최근에는 in situ 법을 사용합니다. Spleneen preserving total gastrectomy (Ann Surg Oncol 2001, J Surg Oncol 2009).
Spleen preservation has benefit in terms of survival if LN #10 is adequately dissected. What is the reason? Is it due to less morbidity and mortality in the shortterm or due to longterm oncologic advantages?
Big incision, NG tube, drain이 꼭 필요한가? 노교수님은 routine NG tube와 routine drain은 사용하지 않는다고 합니다. Prophylatic drain은 선택적으로 합니다 .
연세대에서 2014년 수술한 1,180 환자의 54%가 복강경이나 로봇으로 수술을 받았습니다.
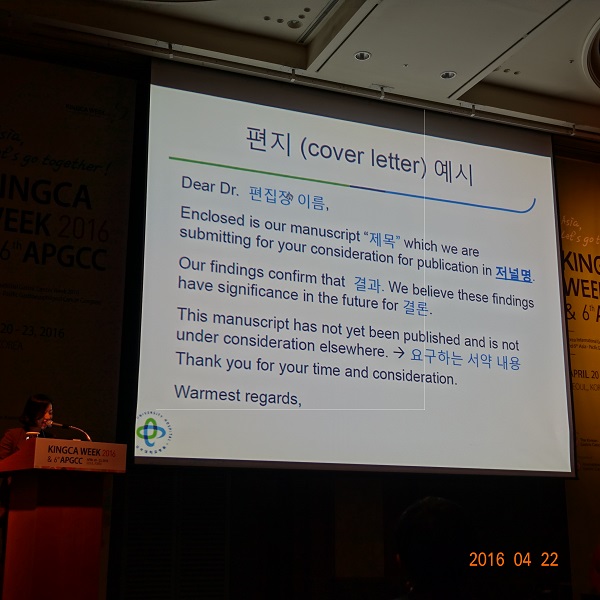
![]() 7. How to write good manuscripts
7. How to write good manuscripts
1) How to write a good manuscript. (건국대학교 이선영)
결과까지는 과거형. 결론은 미국은 현재형을 유럽은 과거형을 선호합니다.
후향적 연구는 다음 4가지 경우에 허용됩니다.
- 희귀한 질병이라서 전향적으로 모을 수 없는 연구
- 전향적으로 허락되지 않는 비윤리적인 연구
- 전향적 연구비를 감당할 수 없는 비싼 연구
- 샘플 수가 아주 많이 모여있는 상태에서 시작한 연구
고찰
- 가능한 6 문단 이내로 요약
- 각 문단마다 본인 연구결과를 언급
- 결과에서 자세한 수치는 빼고 주요 내용만 설명
- 본 연구결과와 관련된 참고문헌만 인용
- 연구 가설에 대한 해석을 포함
- 한계점을 적었다면 그대로 결론이 도출된 이유를 명시
- 최종 결론을 마지막 문단에 요약
2) Writing English medical papers. (아주대학교 장기홍)
Collins English Dictionary를 추천합니다.
P = 0.05 (띄어쓰기)
0.55 +/- 0.21 (띄어쓰기)
Semicolon은 가급적 쓰지 맙시다.
Cases 보다는 patients, subjects 표현이 좋습니다.
Syntatic ambiguity. ... time flies like arrows
can be는 가급적 쓰지 마세요. can be는 능력을 의미할 뿐입니다.
possible 은 < 50%를, probable은 > 50%를 의미합니다.
3) Authorship and conflict of interest (한림대학교 김수영)
Contributor도 서명을 받도록 권합니다. 최근 Medline에서도 non-author contributor를 언급하기 시작했습니다.
이해상충이 없으면 비판적인 결론의 논문이 많습니다. 일반적인 공개의 역치는 미국에서는 3년 이내 1만불 정도라고 합니다.
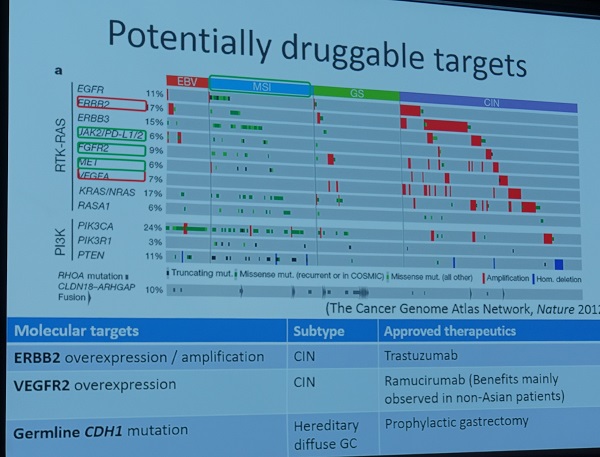
![]() 8. Targeted and immune therapy in gastric cancer
8. Targeted and immune therapy in gastric cancer
1) Druggable targets for the treatment of gastric cancer (울산대학교 김지현)
2) Targeted therapy in HER2-positive gastric cancer (Japanese NCC, Boku)
ToGA trial subgroup 중 아시아 사람은 효과가 적었다.
T-mab을 초기 6 싸이클 후 계속 사용하면 더 좋았다.
일본의 표준 항암치료에 Tmab을 더하면 median survival이 15개월까지 나온 연구가 있었습니다.
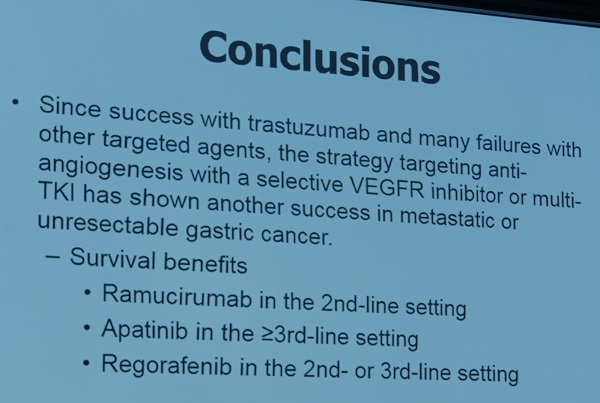
3) Anti-VEGFR (울산대학교 박숙련)
Tmab 이후 많은 연구가 실패하였으나 최근 Rmab이 유망하다는 결과를 보였습니다
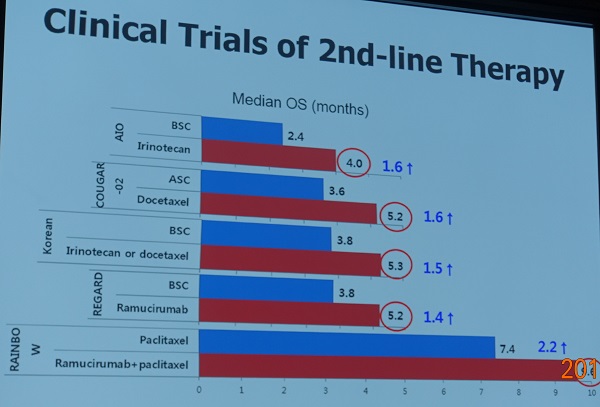
 아직 Rmab은 보험급여가 되지 않고 있으며 60 kg의 경우 월 650만원 정도 필요합니다.
아직 Rmab은 보험급여가 되지 않고 있으며 60 kg의 경우 월 650만원 정도 필요합니다.
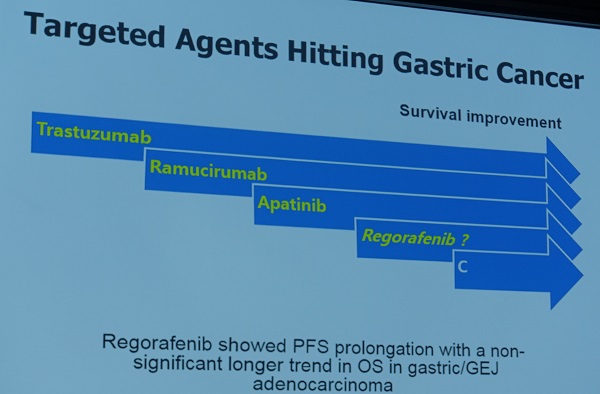
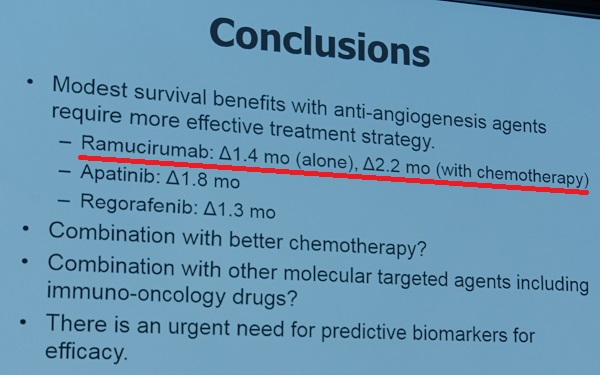
이준행 comment: 티끌 모아 태산이라는 말이 있습니다만, 매달 650만원이라는 고가의 항암제로 고작 한 달 반 더 산다니 약간 허무하군요.
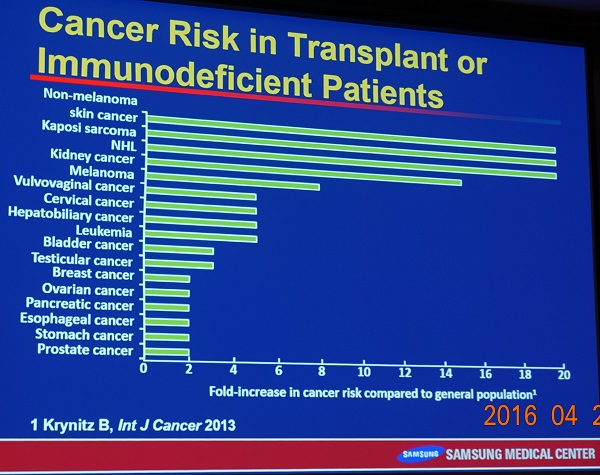
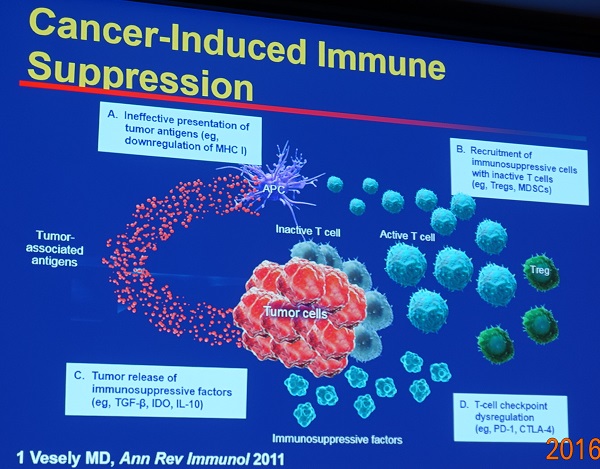
4) Immunotherapy (성균관대학교 삼성서울병원 박세훈)
Immunodefient patient에서 암이 잘 발생하고 tumor 조직에 T cell이 많으면 예후가 좋습니다. 그러나 지금까지의 면역치료는 몇몇 예외를 제외하고는 크게 효과를 보이지 못했습니다.
면역은 암 발생에도 관여합니다. Immune editing이라는 개념이 있습니다. 면역계와 암의 상호작용도 있습니다. 한편 암 자체가 면역을 억제하기도 합니다.
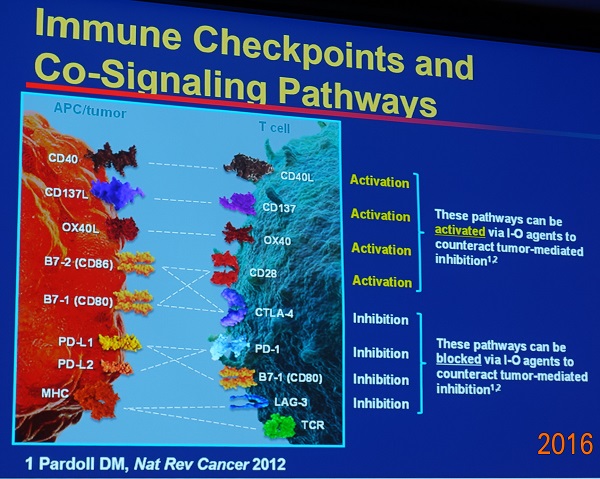
Immune checkpoint inhibitors 두개의 중요한 checkpoint가 있습니다.
![]() 9. Management of gastric subepithelial tumor
9. Management of gastric subepithelial tumor
1) Endoscopic diagnosis and treatment for gastric submucosal tumor (울산대학교 서울아산병원 안지용)
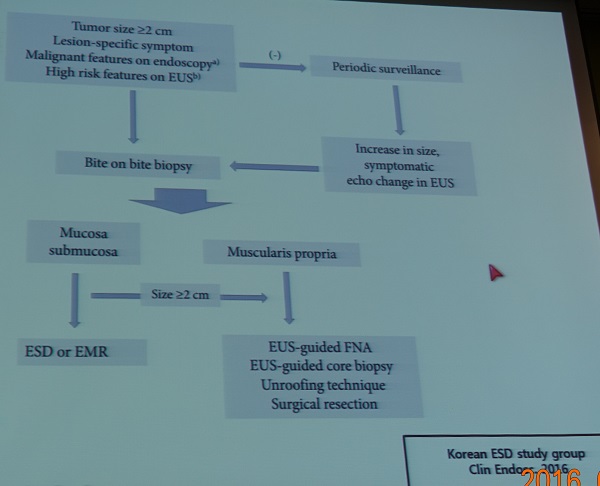
이준행 comment: 2016년 발표된 상기 가이드라인은 EUS 등 검사의 lower size limit를 제시하지 않았다는 점에서 진정한 의미의 가이드라인이라고 말하기 어렵습니다. 과잉 검사를 유도하는 가이드라인은 어떤 이유로도 정당화되기 어렵다고 생각합니다.
홍콩 선생님 한분은 unroofing, FNA, Trucut biopsy로 얻은 샘플로는 mitotic count를 정확히 알기 어렵다는 점을 지적하였습니다.
2) Laparoscopic resection for SET near pyloric ring or GEJ (Nishida, Japan NCC)
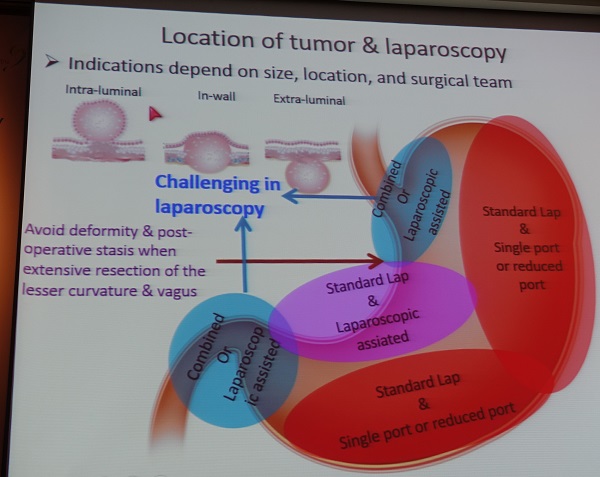
Ng 좌장님이 pyloric ring tumor에 대하여 질문하였습니다. Nishida 선생님은 병이 크면 partial gastrectomy가 좋으나 작으면 (pylorus의 1/3 이하) wedge resection 후 pyloroplasty를 하고 있다고 답하였습니다.
3) Chemotherapy for gastric GIST (서울대학교 김태용)
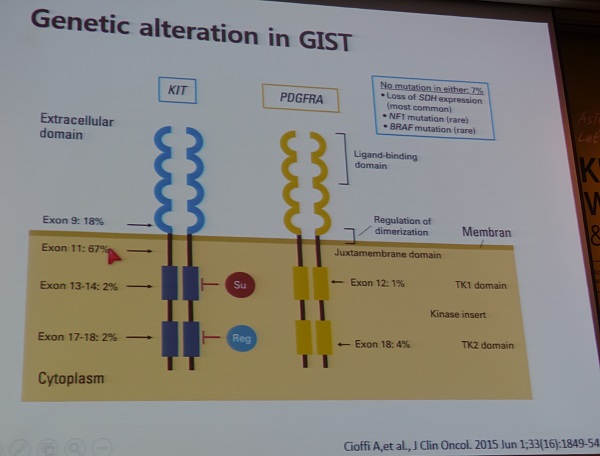
Tumor genotype is of major prognostic importance. Imatinib의 경우 exon 9 mutation이 가장 반응이 좋지 않습니다.
Su 와 Reg는 특정 부위 mutation이 있는 사람에서 반응이 더 좋습니다.
Sunitinib: multikinase inhibitor. Imatinib과 반대로 secondline sunitinib을 사용하는환자에서는 exon 9 mutation 환자가 더 잘 반응한다.
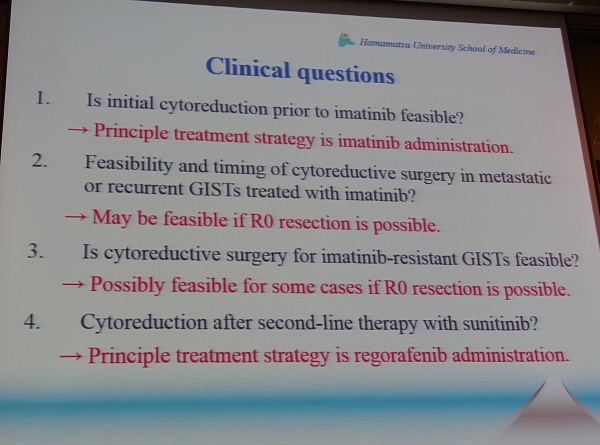
4) Cytoreductive surgery (Kikuchi. Hamamatsu U. Japan)
Imatinib 치료에서 initial tumor volume이 중요합니다.
Cytoreduction before imatinib therpay appears not to improve the prognosis
![]() 10. Meet the professor. Lee Swanstrom (The Oregon Clinic)
10. Meet the professor. Lee Swanstrom (The Oregon Clinic)
미국은 매우 넚어서 내시경 의사가 없는 곳도 많습니다. 그래서인지 미국 외과 의사 training course에 내시경 교육이 포함되어 있습니다. 그러나 교육 기간이 끝나면 50%는 내시경을 그만 둔다고 합니다. 도시에서 일하는 외과의사는 내시경을 계속하지 않는 경우가 많다고 하네요.
Barrett esophagus with high grade dysplasia를 대부분 내시경 절제술이나 RF ablation으로 치료하고 있으므로 이 적응증으로 수술하는 경우는 아주 드물다고 합니다. 과거에는 내시경 절제술이 많았으나 최근에는 RF ablation이 주류입니다.
![]() 11. Antireflux and bariatric surgery
11. Antireflux and bariatric surgery
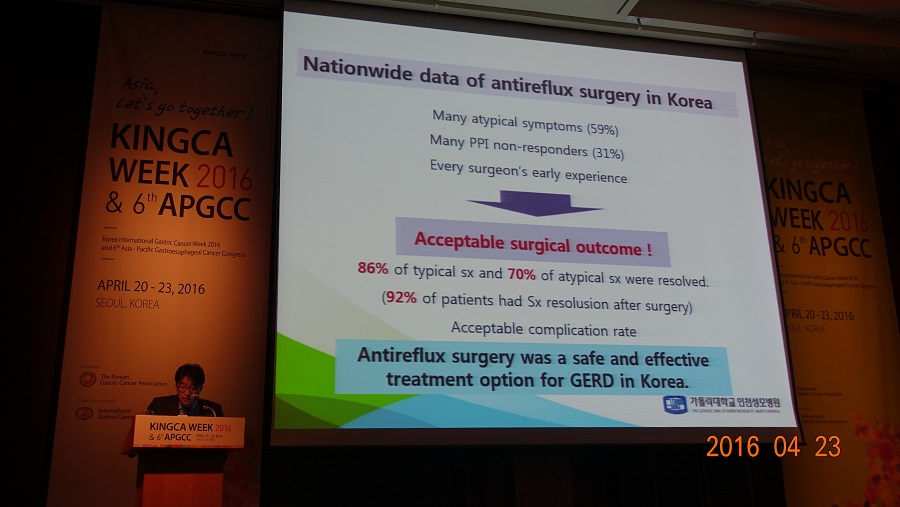
1) Anti-reflux surgery in Korea. 인천성모병원 김진조
2) Anti-reflux surgery: total or partial. University of Queensland, Mark Smithers
강의 결론은 Nissen과 Toupet가 비슷하다는 것입니다. Wrap이 작으면 산 증상은 더 많으나 dysphagia는 덜합니다. 충분히 예상할 수 있는 것이지만...
Patients expectation before surgery is highly important.
수술 전부터 nonspecific motility symptom이 많다는 것이 강조되었습니다. 그리고 수술 후 새로운 증상이 발생할 수 있다는 것을 잘 설명해야 합니다. 증상이 있는지 구체적으로 물어보아야 합니다.
Functional sequalae가 가능합니다. Functional or psychologic quality of life 자료는 아래와 같습니다.
대부분의 환자는 결정을 잘 했다고 답합니다.

저는 누가 수술을 결정하는가, 환자가 스스로 찾아오는 경우가 있는가 질문을 했는데, Smithers 박사는 호주에서 60% 환자는 GI specialist로부터 의뢰되고 40%는 family doctor로부터 의뢰된다고 합니다. 처은 경험이 중요하다고 합니다. 첫 200명의 성적이 매우 좋았기 때문에 많은 환자가 의뢰된다고 합니다 (제가 정확히 이해했는지 모르겠으나... Smithers 박사의 호주식 영어 발음을 알아듣기 어려워서).
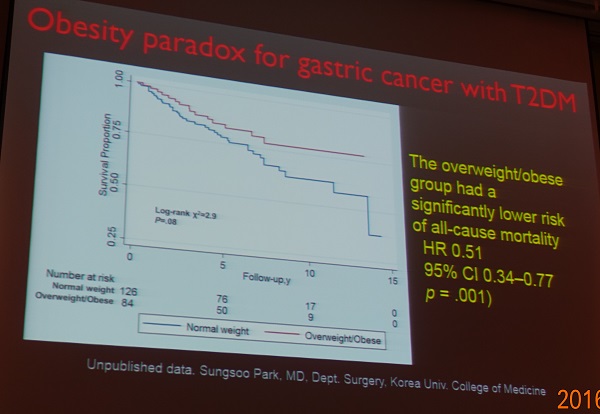
3) Onco-metabolic surgery for type 2 DM with gastric cancer. 고려대학교 박성수
외과의사들이 수술 전후 metabolic change에 관심을 갖게 된 것 같습니다.
박성수 선생님은 강의 거의 마지막에 Obesity paradox 슬라이드르 보여주면서 아직도 할 일이 많다고 결론을 지었습니다.
당뇨가 있으면 B-II를, 당뇨가 없으면 B-I, Roux en Y를 한다고 합니다.
좌장이신 최성호 선생님께서는 당뇨 환자 중 비만도 있고 비만이 아닌 분도 있습니다. 우리나라에는 non-obese DM이 많으므로 beta cell function을 좀 더 고려해햐 할 것 같다, randomized study가 필요하다고 comment를 주셨습니다.
4) Bariatric and metabolic surgery. Singapore National University. Asim Shabbir
동양에는 early onset DM이 많습니다. 신기술로 learning curve가 짧아졌다는 것은 흥미로웠습니다. 그러나 수술의 종류가 너무 많아서 강의 내용을 잘 이해하기 어려웠습니다.
엄마에 대한 bariatric surgery로 인한 benefit이 epigastric change를 통하여 아이에게도 전달된다고 합니다. 자료는 제시되지 않았지만.
저는 비만을 수술로 치료해야 한다는 아이디어에 찬성하는 쪽은 아닙니다만... 외과 선생님들과 국민들의 관심은 높습니다. 오늘 이 주제로 강의한 싱가폴 선생님의 마지막 그림입니다. 입이 다물어지지 않았습니다. 맙소사...
![]() 10. Selected presentations and others
10. Selected presentations and others
Germany. Amicaes Parisi. IMIGASTRIC project.
- Minimal invasive gastric cancer surgery 에 대한 유럽의 다기관 등록 연구.
- http://www.imigastric.com
- 수술의 종류: 복강경 22%, 로봇 22%, 개복 56%. 유럽 쪽에서는 이탈리아에서 로봇 수술이 많다고 합니다.
2) 울산대학교 서울아산병원 김도훈. ESD for adenocarcinoma of EG junction
Siewart type II, 88명. Stricture가 한명도 없었다는 점이 다소 놀라와서 질문을 했습니다. 김도훈 선생님은 Circumferential resection이 적었기 때문이라고 답변을 주셨습니다. 최근에circumferential resection 3예가 있었는데, 그 경우는 oral steroid를 쓰셨다고 합니다. 3/4 이상 절제된 경우 cardia나 pylorus의 경우는 식도보다 stricture가 잘 생기지 않는다고 합니다. ESD 후 2년 동안 내시경과 abdominal CT를 이후는 매년 검사하고 있다고 합니다. 저는 abdominal CT로 충분할지 질문했습니다. 혹시 mediastinal node에서 문제가 생길까봐. 바렛식도암은 3예였다고 합니다.
3) 기타
 Reduction surgery는 추천되지 않음. 리가타 연구
Reduction surgery는 추천되지 않음. 리가타 연구
연자는 Conversion surgery에 대해서는 'slight chance for the cure'라고 주장하였습니다.
 일본의 표준치료입니다.
일본의 표준치료입니다.
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.