EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Dr. Sinn's LiverTODAY 028 - LLV (low level viremia)]
[Dr. Sinn's LiverTODAY 028 - LLV (low level viremia)]
이번 주에는 Hepatology에 실린 Low-level viremia in hepatitis b patients on antiviral treatment: Can we ignore it?을 소개합니다. 삼성서울병원의 자료(Kim JH, Sinn DH, et al. Hepatology 2017)에 대한 editorial인데, 요점을 소개한 후 저자 직강(?)으로 몇 가지를 추가하겠습니다.
With the goal of antiviral treatment being to decrease the morbidity and mortality associated with chronic hepatitis B (CHB), the first-line antiviral agents recommended for treating CHB patients by the American Association for the Study of Liver Diseases (AASLD) include pegylated interferon, entecavir, and tenofovir.[2] With their easy tolerability and efficacy in suppressing viral replication associated with high genetic barrier to resistance, many patients with HBV worldwide were treated with either oral agent, often achieving reversal of cirrhosis and reduced incidence of HCC.[3, 4]
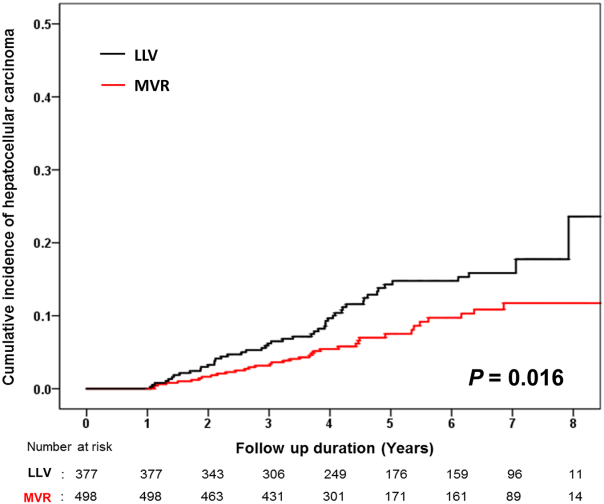
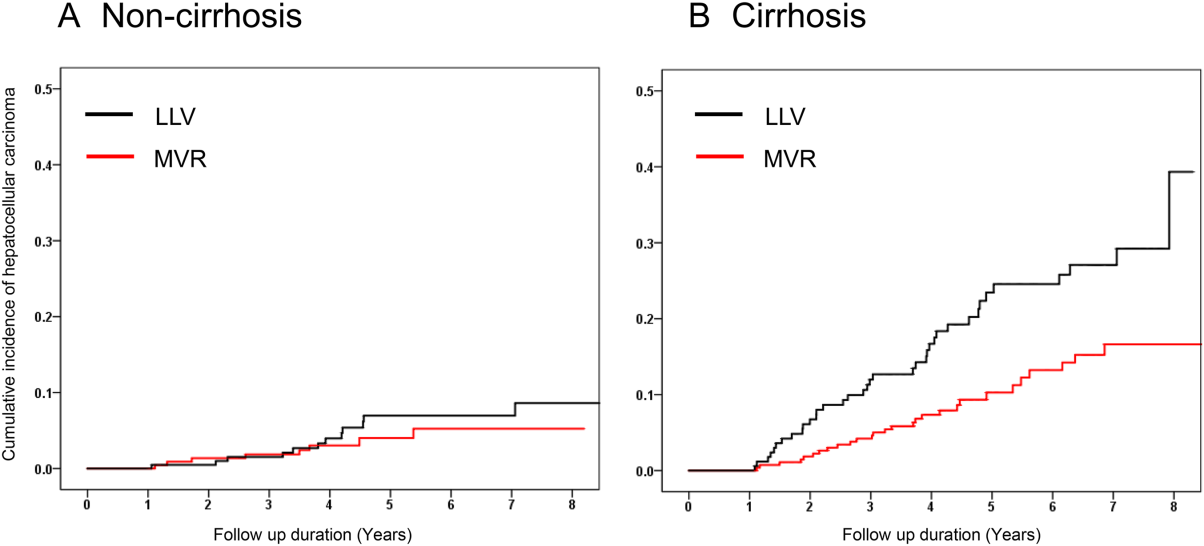
One question posed in the recently updated AASLD guidelines for management of CHB was whether there would be a role for adding a second antiviral agent with persistent low-level viremia (LLV; <2000 IU/mL) while on entecavir or tenofovir. The guidelines suggest that such CHB patients with LLV continue monotherapy.[2] This approach was demonstrated in a European cohort study in which long-term entecavir monotherapy led to a virologic response in the vast majority of treatment-naive patients, including those with a partial virologic response after 48 weeks of treatment.[5] In this issue of Hepatology, a large retrospective study by Kim and Sinn et al. indicates that among patients on antiviral therapy, LLV, defined as persistent or intermittent episodes of HBV DNA greater than the lower detection limit of 12 IU/mL but <2000 IU/mL, was associated with a higher risk of developing HCC when compared with those who maintained virologic response (MVR) with persistently undetectable HBV DNA levels.[6] Previously treatment-naive 875 patients were treated with entecavir for at least 1 year. During a median follow-up of 4.5 years, 85 patients (9.7%) developed HCC. Overall, the development of HCC was more frequent in patients with LLV than MVR (14.3% versus 7.5% at 5 years, P = 0.016). On multivariate analysis, LLV was an independent risk factor associated with HCC development (HR = 1.98, P = 0.002). However, although patients who have cirrhosis with LLV had a higher risk of developing HCC than those with cirrhosis and MVR, among patients without cirrhosis there was no statistically significant difference in the risk of HCC occurrence between patients with LLV and those with MVR, possibly due to a lower risk of HCC in that population than in patients with cirrhosis. Achieving MVR even in noncirrhotic patients may still be important, but we would need a study with a much larger sample size and/or a longer follow-up to show such impact, including stratified analysis by age and sex that may be helpful in accounting for the effect of those strong covariates. Thus, at least for CHB patients with cirrhosis, presence of LLV while on entecavir or tenofovir may not be ignored with a higher risk of developing HCC than those with MVR.
Whether or when a compliant CHB patient with LLV on treatment with entecavir or tenofovir should add another agent is not clear.[2, 7] Entecavir or tenofovir fails to achieve HBV DNA undetectability after 48 weeks in 10% and 30% in HBeAg-negative and HBeAg-positive patients, respectively.[2] In light of the Kim and Sinn et al. study, we should consider a potential alternative strategy, at least in patients with cirrhosis. There is no prospective, well-designed study in answering what is the best strategy among the three options in compliant patients with LLV on entecavir or tenofovir - whether to continue the initial agent, switch to the other agent or add the second agent.
With cirrhosis as the major risk factor of HCC development, and in light of the Kim and Sinn et al. study's findings, we may no longer be able to ignore the significance of LLV in patients with compensated cirrhosis who are already on antiviral therapy. However, in considering how to convert those being treated from LLV to MVR camp, without well-designed comparative studies available we would have to make a decision based on indirect evidence, incorporating data from observational studies, individual patient preference, and available resources.[7]
한글 요약입니다.
1. B형간염 약 복용 후 바이러스가 음전된 후 미검출 상태로 지속 유지되는 사람(maintained virological response, MVR)는 바이러스가 간헐적으로 낮은 농도로 검출되거나, 음전되지 않고 낮은 농도로 지속적으로 검출되는 사람들(intermittent or persistent low level viremia)에 비해 간암 발생 위험이 높았고, 특히 간경변이 있는 경우에는 간암의 발생 위험의 차이가 매우 높았습니다.
2. 핵심은 B형간염 환자들에서는 바이러스가 미검출 상태로 지속 유지되는 것이 매우 중요하다는 점입니다. 간헐적으로라도 바이러스가 검출되는 것은 간경변 환자에서는 간암 발생의 위험을 높였습니다. 연구의 가장 중요한 한계는, 후향적 연구여서, low-level viremia (LLV)가 intermittent하게 나타나는 것이 약을 잘 먹고 있지 않아서였는지가 제대로 평가되지 않았다는 점입니다.약을 복용 중인 환자, 특히 간경변 환자들에게는 정기적 약 복용의 중요성을 꼭 강조하고, 바이러스가 미검출로 잘 유지되는지 확인이 필요합니다.
→ 무증상일 때 약을 잘 먹는다는 것은 매우 어려운 일 같습니다. 저는 요즘에는 복약 도우미 앱을 (삼성서울병원에서도 자체 개발 app이 있습니다) 적극 활용할 것을 권하고 있습니다.
3. 만약 약을 잘 먹고 있는데도 low-level viremia가 지속되는 경우라면, 간경변이 동반된 경우라면, 뭔가 다른 대책을 고민해야 하지 않나 생각이 들었습니다. Compliance issue가 없이, entecavir 치료 중 low-level viremia (partial virological response)를 보이는 환자들의 치료 전략에 대해서는 고대안산병원 임형준 교수님께서 전향적 연구를 진행하고 있는데, 결과가 나오면 추가로 소개하겠습니다.
4. 근거가 없는 상황에서 심평원 보험급여 정책하에서 진료하고 있는 저의 현재 practice는 아래와 같습니다. (evidence 없이 말씀드리는 것이라 매우 조심스럽습니다만, 개인 견해라고 이해해 주시면 감사하겠습니다)
- Low level viremia 때 약제 전환은 entecavir, tenofovir 복용 시에는 1년 이후 보험 급여 하에서 약제 변경이 가능합니다. 자세히 소개하지 않았는데, 이번 자료를 분석하면서 살펴보니 2년 정도는 complete virologic response가 오는 것을 기다려 보는 게 좋은 것으로 나왔습니다 (본문 Table 표에 CVR 인자 분석에 내용을 담았습니다). 이후 high potent drug 사용 중인 경우에는 complete virologic response 오는 것을 2년 정도 기다려 보고 있습니다.
- 2년간 사용중인 환자에서 바이러스가 검출되면, 또는 미검출 환자에서 바이러스가 검출되고 compliance issue가 없다면, 약제간 교체 투약을 하고(entecavir → tenofovir; tenofovir → entecavir) 경과를 살펴보고 있습니다. 심평원 급여 기준하 급여변경이 가능합니다.
- 단일약제 교체 투여 후에도 바이러스 미검출이 유지되지 않으면, non-cirrhosis는 변경된 약제를 유지하고 있습니다. Cirrhotic 환자에서는 다른 한가지 약을 추가하고 있습니다 (이때 다른 한가지 약제를 추가하는 것은 급여인정이 되지 않아, 추가하는 약제는 100/100, 엄밀하게는 비급여 처방을 하고 있습니다).
![]() [References]
[References]
1) EsoTODAY - Esophageal diseases
2) SmallTODAY - Small bowel diseases
3) ColonTODAY - Colorectal diseases
4) Dr. Sinn's LiverTODAY - Liver diseases
© 성균관대학교 의과대학 삼성서울병원 소화기내과 신동현 (2017-7-21)