EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Endoscopic treatment - Stretta, TIF, MUSE and others] - 終
[Endoscopic treatment - Stretta, TIF, MUSE and others] - 終
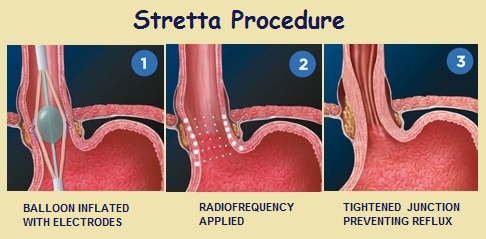
![]() 1. Hands on course on Stretta procedure for GERD (아산병원 정훈용) 2015-12-5. 상부위장관헬리코박터학회 심포지엄
1. Hands on course on Stretta procedure for GERD (아산병원 정훈용) 2015-12-5. 상부위장관헬리코박터학회 심포지엄
1) 최근 우리나라 식약청에서 신의료로 승인되었습니다. 인정비급여로 시행할 수 있다는 의미입니다. 그런데 문제는 너무 비싸다는 것 같습니다.
2) 적응증: PPI를 유지할 수 없는 GERD 환자
a) Non-responder to PPIs: non-acid reflux, poor responder despite high dose PPIs, GERD with LPR, extraesophagal symptoms
b) Intolerant to PPIs: severe adverse reaction to PPIs
c) Refractory GERD: recurrent disease after quitting PPIs
d) Candidate to surgery
3) 금기증
a) age < 18 years
b) pregnant women
c) patients without diagnosis og GERD
d) large hiatal hernia more than 3 cm
e) achalasia or incomplete LES relaxation
f) poor surgical candidate
4) 안전성: 2004년까지 많은 시술예가 있으나 식도천공 합병증으로 중단되었음 (1명 사망). 이후 회사가 바뀌고 electronic delivery를 조금 약하게 하는 등 변화를 줌으로써 현재는 훨씬 안전해짐.
5) 효과: 절반 정도는 약 없이 지낼 수 있음.
6) 기전: 6 level에 radiofrequency를 가하여 coagulation이나 necrosis가 아닌 hypertrophy가 유도됨.
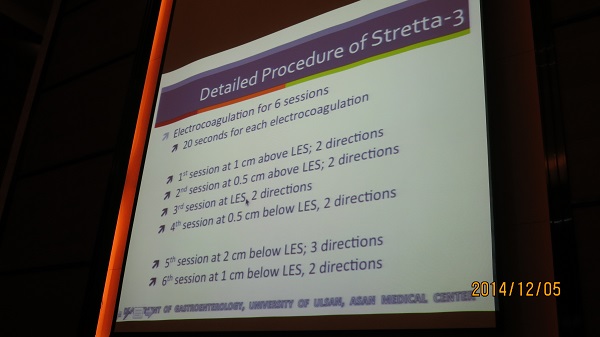
7) 시술 tip
a) 침을 줄이기 위하여 atropine 투여
b) propofol을 이용한 진정
c) 내시경으로 위치를 확인하고 기계에 몇 cm인지를 입력.
문제점: 가장 큰 문제는 고비용입니다. 시술비는 적어도 400만원은 되어야 할 듯 합니다. 너무 비싸다고 할 수 있습니다. 효과가 100%도 아닌데...
![]() 2. Meta-analysis (2014) and other literatures
2. Meta-analysis (2014) and other literatures
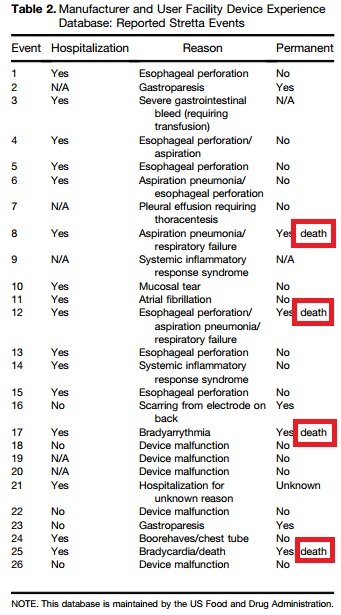
2014년 2월까지 발표된 4개의 무작위 전향적 연구(165명)의 메타분석이 발표되었습니다 (Lipka S. CGH 2015). 제목부터 negative result였음을 강력히 보여주고 있습니다. No evidence for efficacy of radiofrequency ablation for treatment of GERD. 메타분석에서 언급된 미국 FDA 자료에 의하면 4명이 사망하였습니다.
We collected data from 4 trials and a total of 165 patients (153 patients were analyzed). Three trials compared Stretta vs sham, and 1 trial compared Stretta with PPI therapy. The overall quality of evidence was very low. The pooled results showed no difference between Stretta and sham or management with PPI in patients with GERD for the outcomes of mean (%) time the pH was less than 4 over a 24-hour time course, LESP, ability to stop PPIs, or HRQOL.
메타분석의 discussion을 일부 옮깁니다. 18개 연구 1,441명 pooled data를 보여준 Perry의 연구를 가차없이 비판하고 있습니다.
The beneficial effects of Stretta reported by Perry et al were based on single-arm, pre-post design studies, which are prone to regression to the mean, making the efficacy of Stretta susceptible to a high risk of bias. Regression to the mean is a statistical phenomenon that affects all pre-experimental designs that include, or analyze data from, participants selected on the basis of an extreme, usually low or high, pre-intervention condition. Although there is well-recognized value to using single-group studies to identify and quantify the occurrence of adverse events, the role of these studies in evaluating efficacy and safety is not well developed.29 Therefore, the nearly unanimous efficacy of Stretta for the management of GERD observed in single-arm studies is not appropriate for informed decision making.
Recently, SAGES made a "strong recommendation" about the use of Stretta for GERD. However, the panel members of SAGES did not provide details on the process of how they arrived at this recommendation.
Although Stretta’s mechanism of action for the treatment of GERD is not understood fully, it appears to increase the resting tone and reduce the incidence of transient relaxations of the LES. Although data from human beings are lacking, this appears to result from induction of hypertrophy and fibrosis of the LES, and possible tissue neurolysis.
Until more good-quality evidence is available, we agree with the new American College of Gastroenterology guidelines (2013) on GERD that the "current endoscopic therapy... cannot be recommended as an alternative to medical or traditional surgical therapy."

2014년 Pandolfino의 리뷰(CGH 2014)에 실린 Stretta에 대한 부정적 견해
The Stretta device showed promising results with early open-label trials. However, the randomized sham-controlled trials did not support the findings of the open-label trials. Thus, high-quality evidence suggests that the Stretta procedure only provides a mild subjective improvement in symptoms but no objective improvement in reflux burden, EGJ function, or reduction in PPI use. The mechanism of the symptom improvement has been postulated to be related to alteration in esophageal visceral afferent fibers resulting from thermal injury. The lack of improvement in objective parameters, along with complications noted that are not much less frequent or severe compared with fundoplication, make this approach less attractive. Further studies are unlikely to change this recommendation and thus, we would not recommend use of Stretta for the treatment of GERD.
중국에서 laparoscopic fundoplication과 Stretta를 비교한 전향적 연구의 중간결과를 발표하였습니다 (Liang WT. 2015). PPI 중단율은 Stretta 72.3%, fundoplication 68.3%로 비슷하였으나 전형적 증상의 호전은 fundoplication 군이 우월했습니다.
![]() 3. Stretta symposium (2016년 1월 29일 18:00-21:05, Grand Hyatt Hotel)
3. Stretta symposium (2016년 1월 29일 18:00-21:05, Grand Hyatt Hotel)

노출 오류. 쏘리~~~
연자인 Mark Noar 박사(mnoar@gastro-doc.com, Endoscopic Microsurgery Associates, Towson, Maryland)의 최근 letter를 소개합니다 (Noar. CGH 2015). 2014년 Pandolfino의 리뷰(CGH 2014)에 실린 Stretta에 대한 부정적 견해에 대한 반박의 글입니다.
The device design and function specifically allow for treatment of the muscularis propria only and not the mucosal or submucosa.
... results in muscle fiber bundle proliferation and increased muscle cell volume within each bundle, cuasing sphincter lengthening and thickening and increased physiolical barrier function.
1) Up-to-date diagnosis and treatment of GERD (연세대학교 이상길)
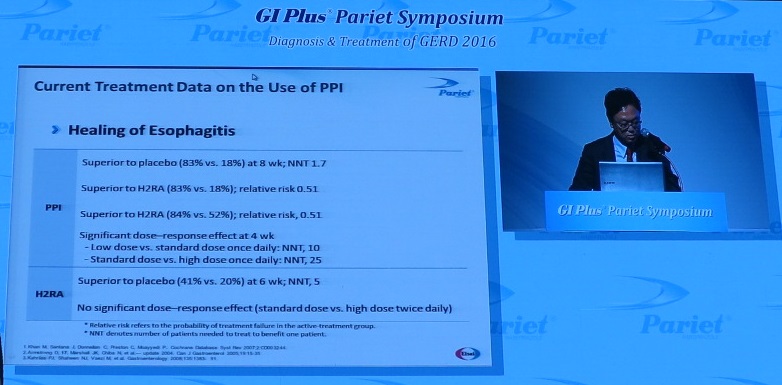
GERD relapse rates on maintenance Placebo - 78%
H2RA - 64%
Half dose PPI - 40-50%
Standard dose - 15-20%
이상길 선생님은 continuous therapy와 on demand therapy를 비교한 일본 연구를 소개하셨습니다 (Nahagara SJG 2014:49;409-417). 전체적으로 continuous therapy 군이 on demand therapy군에 비하여 증상조절이 잘 되었습니다. 그러나 24주 연구기간 중 마지막 7주 동안에는 양군 사이에 차이가 없었습니다 (아래 그림). 즉 continuous therapy나 on demand therapy나 오래되면 비슷해진다는 것입니다. 이상길 선생님은 심한 식도염이 적은 우리나라에서는 on demand가 우용할 것으로 말씀하셨습니다. (이준행 주: 흥미로운 자료라고 생각합니다. Continuous therapy는 매일 약을 먹는 방법이고 on demand therapy (gradually increase the interval between medications as long as the symptoms do not recur)는 보통 일주일에 2-3회 먹는 방법인데 별 차이가 없다는 것입니다. 저는 threshold therapy를 선호하는데 개념상 on demnad에 가깝습니다.)
Percentage of patients who were symptom free for 6 or more days a week as recorded on a daily chart. **p < 0.01, *p < 0.05 versus on-demand group.
NERD에서 유지요법의 효과가 낮습니다 (Kusano JG 2015:50;298-304). Maintenance therapy에 대하여 만족한 환자는 ERD 군에서 70%, NERD 군에서 50%였습니다.
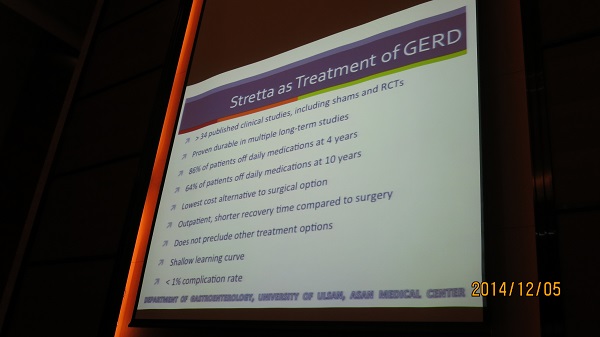
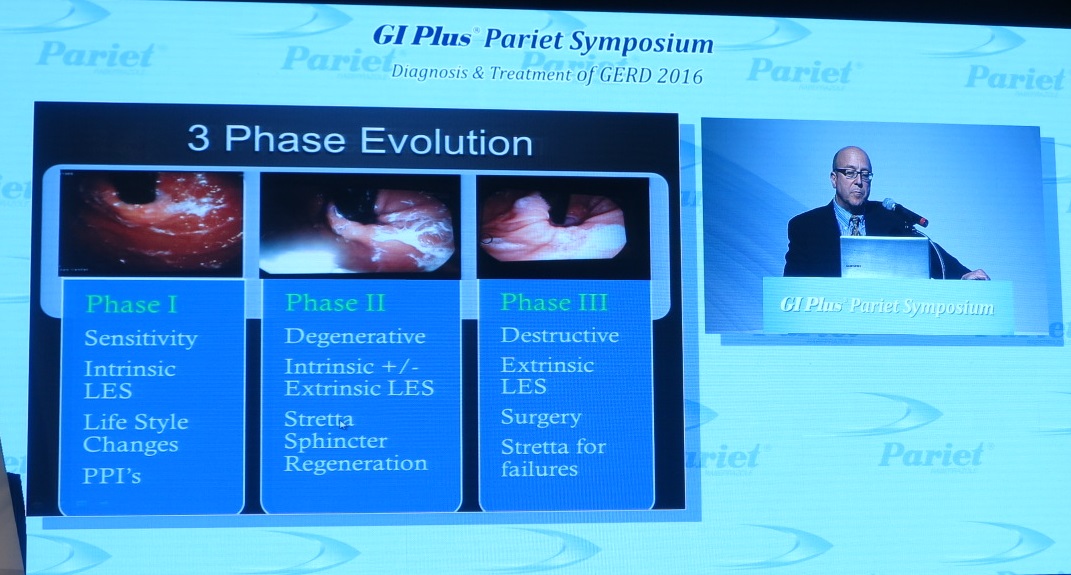
2) Stretta treatment of GERD (Mark Noar)
Noar 박사는 자신을 "Interventional sphincterologist"로 소개하였습니다.
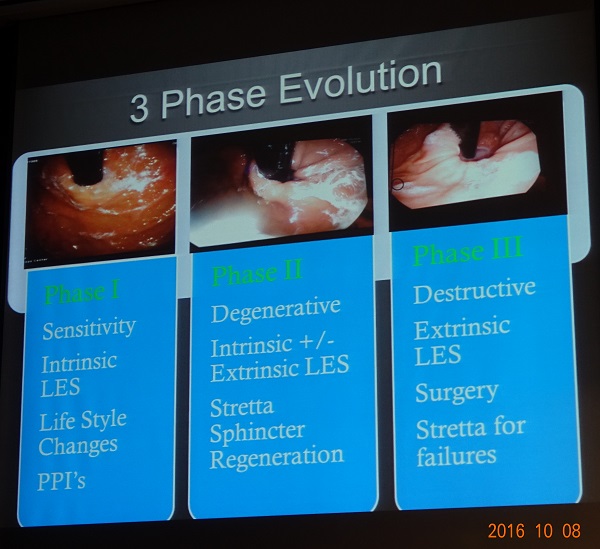
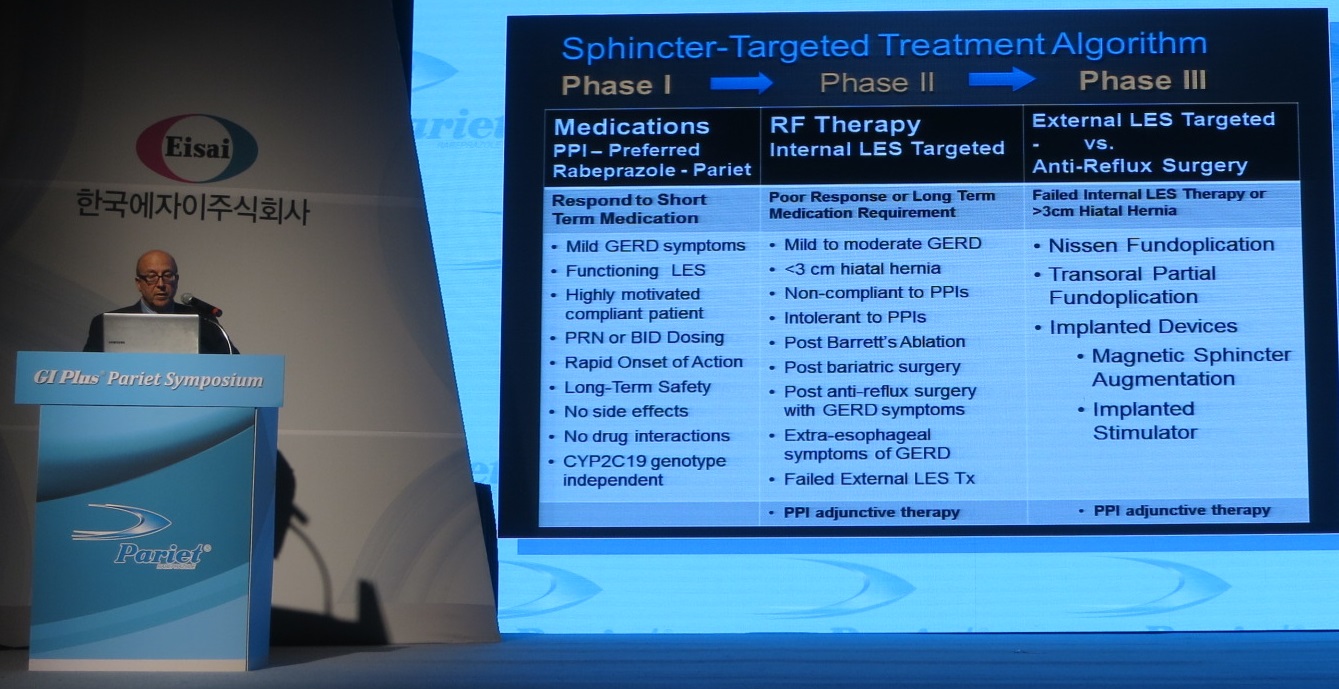
GERD는 일종의 chronic degenerative disease입니다. 3 phase evolution을 생각할 수 있습니다. (1) sensitive, (2) degenerative, (3) destructive로 나눌 수 있고 이 중 두번째가 Stretta 치료 대상입니다.
Pathological disease concepts Acid-pepsin interaction
TRPV1/TRPV4 receptor mediated
LES dual sphincter degradation
Sling-clasp muscles
Muscularis mucosa sphincters
Multi-factorial pathogenesis

The practice of sphincter directed therapy Correct the degenerative effects of chronic reflux
Restore natural sphincter function
Restore barrier function
Increase gastric yield pressure
Control TLESRs
Reverse premalignant conditions
Prevent development of cancer

Stretta RF delivery catheter Flexible
Sofe bougie tip (20 Fr)
6 mm shaft (20 Fr)
65 cm operating shaft
Balloon/basket (max 3 cm)
5.5 mm Niti electrode needles
Continous irrigation and suction channel

Contraindications Subjects under the age of 18?
Pregnant women
Patients without a diagnosis of GERD
Hiatal hernia > 3 cm
Achalasia
Severe scleroderma
Esophageal or gastic varix
Poor surgical candidates
3) Discussion
- 최근 미국에서 Stretta가 보험급여가 시작되었다. 보험회사들은 Stretta 시술을 통하여 증상이 개선되어 환자가 병원 방문을 덜하고, 검사를 덜하고, 약을 덜 먹어서 경제적으로 도움이 된다고 판단한다.
- Stretta 시술 수년 후 증상이 재발하는 예가 있다는데...? Noar 박사 답변: GERD는 chronic regenerative disease이다. 한번 증상이 다소 좋아졌다더라도 체중관리, 야식/과식 피하기, 알콜 피하기 등을 게을리하면 reflux가 발생하고 이로 인한 degenerative change가 심해질 수 있다.
- 내시경에서 GE junction이 patulous하게 열려있으면 motility 검사를 하지 않는다. 그러나 GE junction이 tight한 모양인데 GERD 증상이 있다면 motility disease 가능성 고려하여 manometry를 시행한다.
- Stretta 시술 후 바렛식도가 regression 된다.
- 협착을 경험한 적이 있는가? Noar 박사 답변: 아직까지는 없었다. LES pressure가 올라가는데 보통 정상 정도까지만 오른다. 그 이상 오르는 경우는 거의 없다.
- LPR (laryngopharyngeal reflux) 환자에서 크게 도움이 된다.
- 3 cm 이상 hiatal hernia에서는 불가능한가? Noar 박사 답변: 변형된 technique을 사용하여 시술할 수 있다. 심한 경우에는 hiatal hernia는 surgery로 교정하고 이어서 Stretta procedure를 할 수 있다.
![]() 4. Stretta에 대한 보건복지부 고시 (2014)
4. Stretta에 대한 보건복지부 고시 (2014)
2014년 마지막 '계간 의료정책포럼'에 'Stretta를 이용한 위식도역류질환의 치료 (보건복지부 고시 제2014-178호)'에 대한 내용이 실렸습니다 (링크). 향후 중요해질 수 있을 것 같아서 전문을 옮깁니다.
"STRETTA를 이용한 위식도역류질환 치료술은 위식도역류질환 환자를 대상으로 고주파에 의한 식도점막의 손상을 유발하여 하부식도괄약근을 두껍게 함으로써 역류질환 증상을 개선시키는 의료기술이다. 이 시술의 안전성은 시술관련 합병증을 통해, 유효성은 약물복용 중단 및 감소, 증상개선, 기능검사지표로 평가하였다. 문헌검색은 코리아메드를 포함한 8개 국내 데이터베이스와 Ovid-MEDLINE, Ovid-EMBASE 및 Cochrane Library 등의 국외 데이터베이스를 이용하였다.관련문헌은 [[gastroesophageal reflux.mp. OR exp Gastroesophageal Reflux/] OR 'GERD.mp.' OR 'GORD.mp.']] AND 'stretta.mp.']등의 검색 전략 및 수기검색을 통해 총 277편의 문헌을 검색하였고, 중복 검색된 문헌(86개)를 포함하여 총164개가 제외되어 총 27개의 연구가 최종 평가에 포함되었다.
체계적 문헌고찰에 의하면, 본 시술 후의 천공, 수혈이 요구되는 출혈, 사망과 같은 중증 합병증 발생은 보고되지 않았다. 시술관련 합병증 발생률은 sham 치료 및 대조군과 비교된 연구에서 중재군이 비교적 흉골후방동통, 복통 및 상복부 불편감이 높게 보고되었으며, 전후 연구(19편)에서는 위마비 1.1%∼4%(7편), 위근위부 경미한 출혈2%(2/99명)(1편),점막출혈 3.3%(3/90명)(1편), 표재성점막손상 2.2%∼5.5%(3편),흉골후방동통1.7(2/118명)∼100%(9/9명)(9편), 연하곤란 0.8(1/118명)∼77.7%(14/18명)(5편),소화불량 12.1%(1편), 오심/구토 1.7%∼12.5%(7편)등이 보고되었다. 시술로 인한 중증 합병증은 발생되지 않았고, 일부 연구들에서 비교적 높게 보고된 흉골후방동통및 상복부 불편감은 상부위장관 내시경 시술의 특성상 발생되는 증상으로 이는 일시적이거나 대부분 진통제 투여 없이 회복되었으며, 그 외의 사례들에서도 대부분 일시적인 경미한 수준으로 후유증이나 처치가 필요 없이 회복되었다는 점에서 안 전성은 수용 가능한 수준으로 판단하였다.
본 시술의 유효성은 약물복용 감소 및 중단, 증상개선, 기능검사지표로 평가하였다. 약물복용 중단 및 감소 지표와 관련하여, sham 치료군 및 대조군과 비교된 중재군의 약물복용 중단 및 감소율에 대한 통합교차비(pooled OR)는 시술 후 6개월시점 3.29(95% CI 1.66-6.49, I2=0%,p=.0006),12개월 시점에서는 2.67(95% CI 1.29-5.52, I2=12%, p=.008)이었다. 전후연구(21편, 추적관찰 3개월∼10년)에서의 약물복용 중단율은 20.2%∼80.7%로 보고되었다. 증상개선 지표에 있어,가슴쓰림 증상점수는 sham군과 비교된 무작위 임상연구(2편)에서 6개월 시점시 유의하게 감소되었으며, 대조군과 비교된 무작위 임상연구(1편)에서는 두 군간 유의한 차이는 없는 것으로 보고되었다. 역류증상 점수는 sham군과 비교된 무작위 임상연구(1편)에서 6개월 시점시 중재군이 유의하게 감소되었으며, 대조군과 비교된 무작위 임상연구(1편)에서는 6개월 시점시 중재군이 유의하게 개선된 것으로 나타났으나, 12개월 시점시에는 유의한 차이가 없는 것으로 보고되었다. GERDHRQL 증상점수는 sham군 및 약물치료군과 비교된 연구(3편) 모두에서 중재군에서 유의한 증상개선이 보고되었다. 전후 연구(16편)에서는 가슴쓰림, 역류증상점수를 포함하여 GERD-HRQL, SF-12/36, QOLRAD, 만족점수의 모든 지표에서 유의하게 개선이 있는 것으로 보고되었다(p <.05).
기능검사지표에 있어, 24시간 식도산도검사(%total time pH < 4.0 (4편), Johnson-DeMeester점수(1편))결과는 sham 및 대조군과 비교된 무작위 임상연구 5편 중 2편에서 중재군이 유의한 개선이 있는 것으로 보고되었으며, 3편에서는 두 군 간 유의한 차이는 없었다. 전후연구에서는 10편중 7편의 연구에서 시술 전과 비교시 유의하게 개선된 것으로 보고되었으며, 8년 장기추적 관찰된 1편의 연구에서는 4년 시점까지 유의한 개선을 보였으나 8년 시점에서는 다시 기저상태의 값으로 돌아간 것으로 보고되었다. 2편에서는 유의한 개선이 확인되지 않았다. 하부식도내압은 sham 치 료군과 비교된 무작위 임상연구 4편 중 1편에서 중재군이 유의한 개선됨이 보고되었으며, 3편에서는 유의한 차이가 없었다. 전후연구에서는 9편중 3편에서 시술전후 유의한 증가를 보고하였으며, 그 외의 연구에서는 시술 전후 유의한 차이는 없는 것으로 보고되었다. 이에 소위원회에서는 기능검사지표와 증상과의 상관성이 떨어져, 연구들 마다 일관된 결과를 보이지 않는 것으로 판단하였다. 또한, 식도내압의 경우 근육이 좌우하는데 동기술의 원리는 식도점막에 열을 가해 변형을 시키는 것이므로 시술후의 내압을 증가시키는 데 제한이 있다는 의견이었다.
종합하면, 동 기술은 sham 및 대조군과 비교해 약물치료 중단 및 감소에 있어 의미 있는 결과를 보였으며, 증상개선의 효과가 있었다. 다만, 일부에서 무작위 임상연구의 추적관찰기간이 6∼12개월에 불과하고, 서양인에 비해 아시아인의 상기병명으로 인한 중증도가 낮고, 아시아인을 대상으로 한 연구들이 부족하다는 점에서는 향후 장기적 추적관찰 연구는 필요하다는 의견과 함께 적응증을 제한할 필요성이 제안되었다.

이러한 문헌적 근거를 토대로 본 기술은 약물요법을 유지할 수 없거나 약물요법 시행이 적절치 않은 위식도역류질환 환자를 대상으로 열에 의한 식도점막 손상을 유발하여 하부식도 괄약근을 두껍게 함으로써 환자에게 위식도 역류증상의 호전 및 약물치료 감소를 기대할 수 있는 시술로써 안전성 및 유효성이 있는 의료기술로 평가되었다. (권고등급 B)"
본 결과는 보건복지부 고시 제2014-178호(2014년 10월 17일)로 공표되었다.
![]() 6. 2016년 10월 8일 SGI meeting - Noar 박사 강의
6. 2016년 10월 8일 SGI meeting - Noar 박사 강의
Disease progression mechanisms
Sphincter-target therapy인 Stretta는 destructive procedure가 아니고 stimulating procedure입니다.
10 year durability study: Noar M. Surg Endosc 2014
RESULTS: The primary outcome was achieved in 72% of patients (95% confidence interval 65-79). For secondary outcomes, a 50% or greater reduction in PPI use occurred in 64% of patients, (41% eliminating PPIs entirely), and a 60% or greater increase in satisfaction occurred in 54% of patients. Both secondary endpoints were achieved. The most common side effect was short-term chest pain (50%). Pre-existing Barrett's metaplasia regressed in 85% of biopsied patients. No cases of esophageal cancer occurred.
Extrinsic sphincter therapy와 intrinsic sphincter therapy가 있고 이를 함께 쓰면 더 좋습니다. Extrinsic sphincter therapy인 Nissen fundoplication이 실패한 경우 intrinsic sphincter therapy인 Stretta therapy가 좋은 option입니다.
![]() 7. 2016년 11월 26일 내시경학회 breakfast session 정훈용 교수님 강의
7. 2016년 11월 26일 내시경학회 breakfast session 정훈용 교수님 강의
"Stretta 치료는 gap 치료입니다."
1) 내과적 치료와 외과적 치료의 gap에 해당하는 치료입니다. 대부분의 환자에게 해당한다면 gap이라고 할 수 없을 것입니다. 10-15% 정도의 환자에게 적용할 수 있는 gap 치료입니다.
2) Gap 치료로도 효과가 없으면 수술로 넘어가야 합니다. 수술로 넘어가기에 유리한 치료가 Stretta입니다.
Stretta procedure for bariatric patient: Sleeve gastrectomy를 받은 환자에서는 위용적이 적어서 GERD가 발생하기 쉬운데 이 환자에서는 fundoplication을 할 수 없고 Stretta를 적용할 수 있습니다.
Poor outcome이 예측되는 환자 Subjects under the age of 18 (아마도 동의서 문제)
Pregnant women
Patients without a diagnosis of GERD
Hiatal hernia > 2 cm
Achalasia
Poor surgical candidates
아산병원 Stretta 시술 10예 중 6명은 PPI를 끊었다고 합니다. Stretta 시술 후 LES pressure가 10 이상으로 올라갑니다. 10 미만인 사람은 10 이상으로 올라가는데 20 정도인 사람이 더 이상 올라가지는 않습니다.
Anxiety, overlap syndrome이 있는 사람은 역류 증상은 좋아지지만 anxiety나 다른 증상 때문에 overall quality of life는 개선되지 않습니다.
[Floor 질문]
사전 평가는 어떻게 하십니까?
[정훈용 교수님 답변]
내시경과 manometry 정도를 하고 있습니다. 내시경에서 hiatal hernia가 보이면 시술하지 않는 것이 좋습니다. LES pressure가 10이하로 낮은 사람이 많지는 않지만 이들에서는 효과가 더 좋을 것 같습니다.
[Floor 질문]
비용은 어떻습니까?
[정훈용 교수님 답변]
신의료기술 신청을 하면 NECA에서 systemic review를 한 후 사용 가능으로 판정이 되면 1년 후 심평원 프로세스를 진행하게 되어 있습니다. 그런데 아직도 1년 후 시술 성적을 평가하는 작업이 잘 되지 않고 있습니다. 따라서 현재는 실손보험을 받을 수도 없습니다. Catheter 가격은 5000 달러 정도입니다. 환자는 600만원 정도를 내게 됩니다.
[Floor 질문]
최근의 meta-analysis에서 증상이나 parameter 등에서 효과가 없다는 결론이었는데요... 어떻게 생각하시는지요?
[정훈용 교수님 답변]
모든 parameter가 다 좋아지는 것은 아닙니다. 그러나 일부 parameter와 상당수 증상이 개선됩니다. 수술로 PPI를 끊을 수 있는 경우는 60-70% 정도입니다. Gap 치료인 Stretta가 이보다 높을 것으로 기대하기는 어렵습니다. 환자의 증상은 좋아지지만 일반적이고 객관적인 parameter가 뚜렷하게 좋아지는 것은 아닙니다.
![]() [FAQ]
[FAQ]
[2018-7-3. 이준행 질문]
Laparoscopic antireflux surgery 경험이 쌓이고 있습니다. 우리나라에서 항역류 수술의 전망을 어떻게 보고 계십니까?
[2018-7-3. 이풍렬 교수님 답변]
우리나라에서도 anti-reflux surgery의 경험이 쌓이면서 이제는 꼭 도움되는 환자에서 시행할 수 있게 되었다는 점에서 의미가 있습니다. 지금까지는 적응증 선정이 loose 했는데, 이제부터는 적응증을 잘 잡아야 할 것 같습니다.
![]() [Reference]
[Reference]
1) 불응성 역류성 식도염의 새로운 치료법 케이캡 아산병원 김도훈 교수 PDF
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.