EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [StomachTODAY 041. Immune checkpoint inhibitor-induced hemorrhagic gastritis / colitis] - 終
[StomachTODAY 041. Immune checkpoint inhibitor-induced hemorrhagic gastritis / colitis] - 終
1. Immune checkpoint inhibitor란?
2. Immune checkpoint inhibitor의 부작용
4. 출혈성 대장염
5. 간세포암 atezolizumab + bevacizumab 치료에서 위장관 천공
6. 췌담도파트의 처방례
7. References
![]() 1. Immune checkpoint inhibitor란 무엇입니까?
1. Immune checkpoint inhibitor란 무엇입니까?
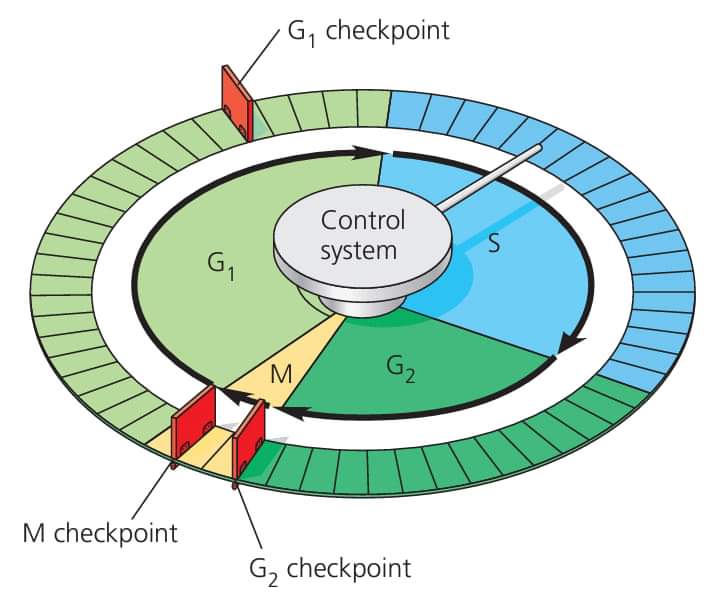
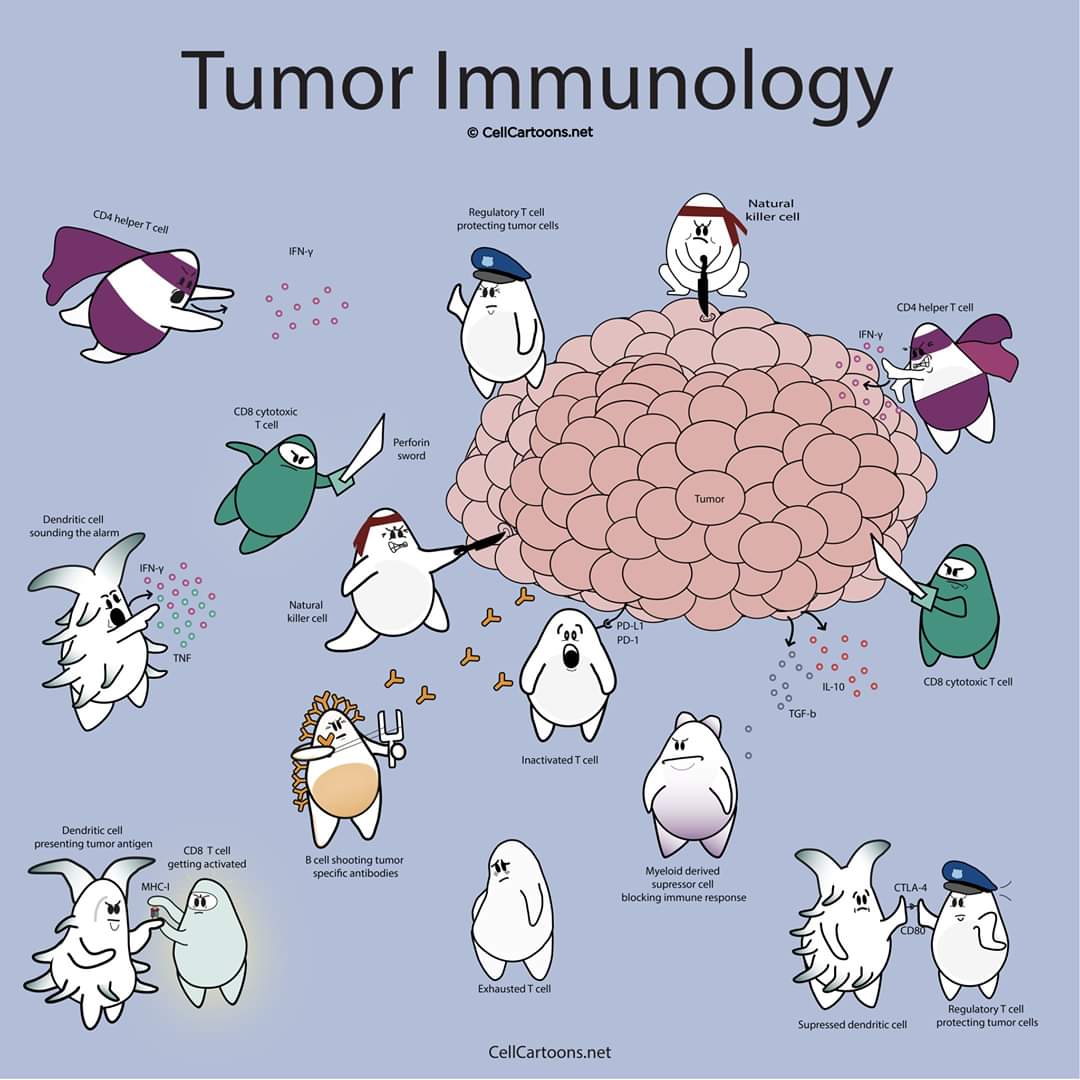
학생 때 이런 그림을 보신 적이 있을 것입니다.
Immune checkpoint inhibitors는 폐암, 악성 흑색종 등 다양한 악성질환에서 사용됩니다. 아래 그림에서 보이는 바와 같이 크게 세개의 target molecule이 있습니다.
source: The Pharmaceutical Journal 2018
The T-cell receptor binds to an antigen found on the major histocompatibility complex on the surface of the cancer cell.
1) This is a stimulatory response and activates T cells to remove pathogens or cancer cells (shown as the positive circles). A co-stimulatory receptor also exists (CD28), which binds to a ligand (CD80). This results in an increased immune response toward the cancer cell
2) CTLA-4 has a stronger affinity to CD80 and so competes with the co-stimulatory pathway to inhibit the response and ‘switch it off’
3) When a strong TCR stimulus exists, the inhibitor molecule CTLA-4 is upregulated and transported to the surface of the cell; a similar process occurs with PD-1
4) The checkpoint inhibitors act by blocking the inhibitory response by targeting CTLA-4, PD-1 or the ligand PD-L1.
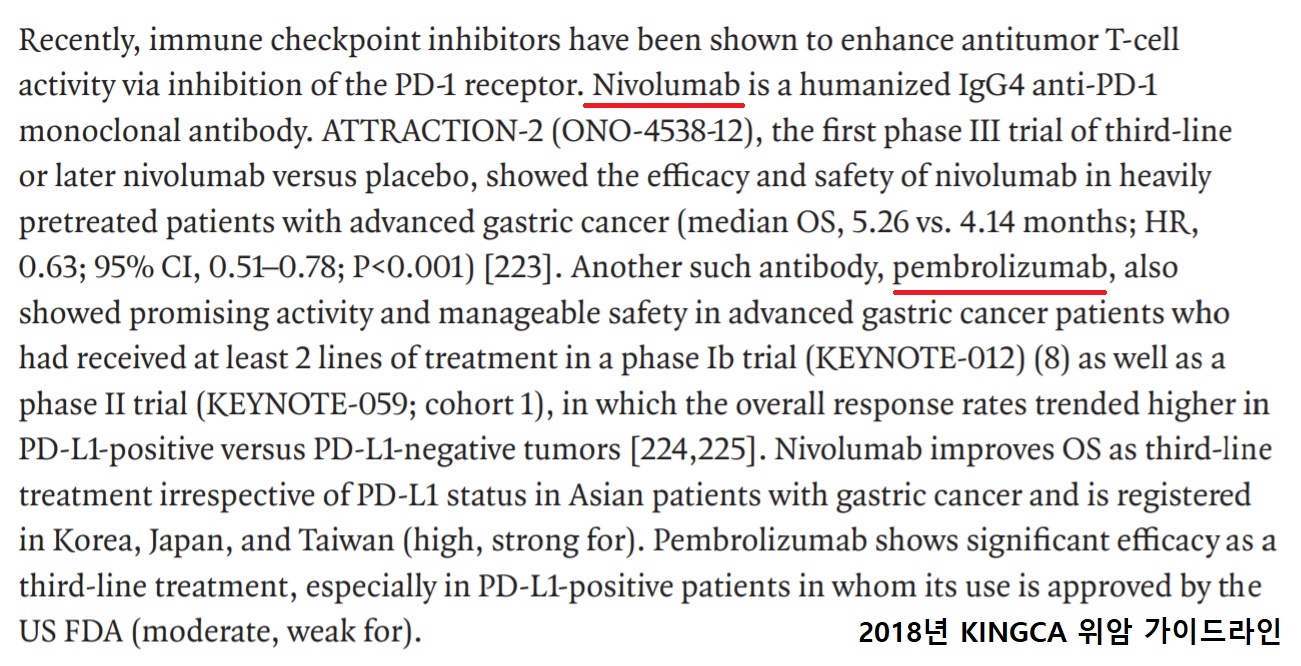
위암 영역에서도 immune-checkpoint inhibitor의 역할에 대한 연구가 활발합니다. 2018년 KINGCA 위암 가이드라인에서도 아래와 같이 언급되고 있습니다.
![]() 2. 부작용
2. 부작용
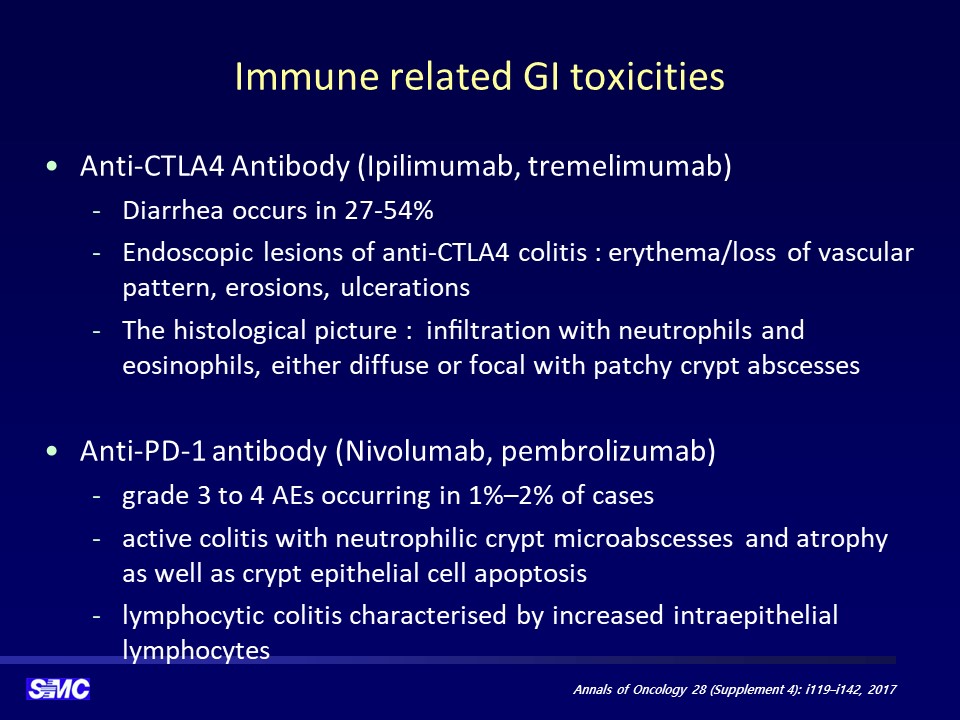
Checkpoint inhibitor는 면역기능에 작용하는 약이므로 면역과 관련된 부작용이 여러 장기에서 발생할 수 있습니다. 한 가지 약을 쓸 때에도 발생할 수 있지만 기전이 다른 두 개의 checkpoint inhibitor를 쓰면 심한 부작용이 발생하기 쉽습니다. 대장염, 피부 발진, 갑상선 기능저하증 등이 흔하지만 출혈성 위염도 가능합니다. 조직검사에서는 lymphocytic 혹은 eosinophilic gastritis의 양상을 보입니다. 크론병 비슷한 양상을 보일 수 있습니다.
약물역학위해관리학회지 2019 (한림대 장승훈)의 일부를 옮깁니다.
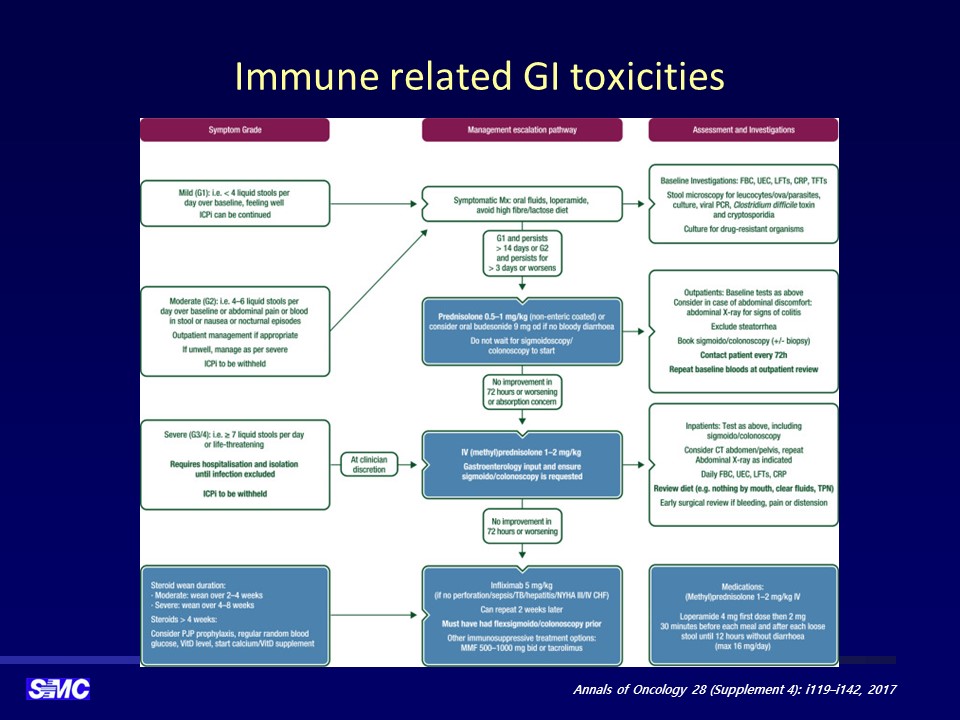
PD-1/PD-L1 억제제 투여 후 경증 설사가 발생하는 경우는 6-8%로 빈번하지만 중증 대장염을 유발하는 경우는 0.6%로 매우 드물다. CTLA-4 억제제에 의한 장염의 발생률은 12.2%로 PD-1/PD-L1 억제제보다 많이 발생하고 CTCAE 3-4등급의 장염도 10.4%나 되는데, 양상이 크론병과는 상당히 이질적이고 궤양성 대장염과 더 유사하지만 약물에 의하여 발생한 대장염 환자의 약 25%가 소장 전반에도 염증이 발생한다는 것은 궤양성 대장염과 다른 점이다. PD-1/PD-L1 억제제에 의한 대장염은 언제든 발생할 수 있으나 치료 시작 후 수 개월 이후에 나타나는 경우가 많으나, CTLA-4 억제제인 경우는 두 번째나 세 번째 투여할 때 나타나는 경우가 많다. 항암제에 의한 대장염은 감염성 대장염과 감별이 필요하다. 경증 설사인 경우 항암제 치료를 지속하면서 적절한 대증요법을 시행하는데 2주 이상 증상이 지속되는 경우에는 항암치료를 중단하고 저용량의 스테로이드를 투여할 수 있으며, 3일간 증상 호전이 없거나 악화되면 고용량 스테로이드를 투여하며 이것에도 불응하는 경우에는 TNF-alpha 억제제인 infliximab 투여를 고려한다. 하루 4-6회 설사를 하는 중등증 대장염 증상을 보이는 경우에는 면역관문 억제제 투여를 중단하고 대증요법과 환자의 반응 을 관찰하며 저용량 스테로이드, 고용량 스테로이드, infliximab 투여로 순차적으로 치료 단계를 상향한다. 증상이 회복 되면 PD-1/PD-L1 억제제는 재투여 가능하나 CTLA-4 억제제는 영구 중단을 고려해야 한다. 하루 7회 이상의 설사, 심한 복통을 호소하는 중증 대장염이 발생한 경우에는 즉각 항암제 투여를 중지하고 대증요법과 고용량 스테로이드를 투여해야 한다. 이에 불응하면 infliximab을 추가하고 회복 후에도 항암치료의 재개는 불가능하다.
Intestinal Research 2021에 실린 종설에서 옮깁니다.
ICI ASSOCIATED IMMUNE-RELATED ADVERSE EVENTS
irAEs (immune-related adverse events) associated with ICIs are commonly known to affect the colon, liver, lungs, pituitary, thyroid and skin, and less commonly the heart, nervous system and other organs. The reported incidence of irAEs from different clinical trials has been variable, largely due to an inconsistent definition of an irAE. An irAE incidence of 15% to 90% (of any grade) has been reported and severe toxicities requiring immunosuppression after discontinuation of the offending drug occurred 0.5% to 13% of the time. Most of these clinical trials state that gastrointestinal tract toxicities tend to be the most commonly occurring serious irAEs. A systematic review conducted by Wang et al. focused on fatal toxicities of all ICI therapies using the database of the World Health Organization, reported a total of 613 fatal events from 2009 to 2018. Out of these, 198 deaths were due to anti-CTLA-4 therapy, and colitis was the cause in 135 cases (70%). Numerous mechanisms have been proposed for irAEs that occur with ICI usage. One belief is that since CTLA-4 is responsible for the regulation of self-antigen tolerance, blockage of CTLA-4 can lead to downstream autoimmunity leading to CD4 T-helper cell and CD8 T-cell tissue infiltration and cytokine release. Mouse modes of regulatory T-cells (Treg) deficiency subsequently developed autoimmune diseases. Since CTLA-4 is abundantly expressed on the surface of Treg cells, CTLA-4 blockade could lead to diminished numbers of Treg and lead to autoimmunity. Recent data advocate the involvement of human gastrointestinal microbiota in the development of ICI induced colitis.
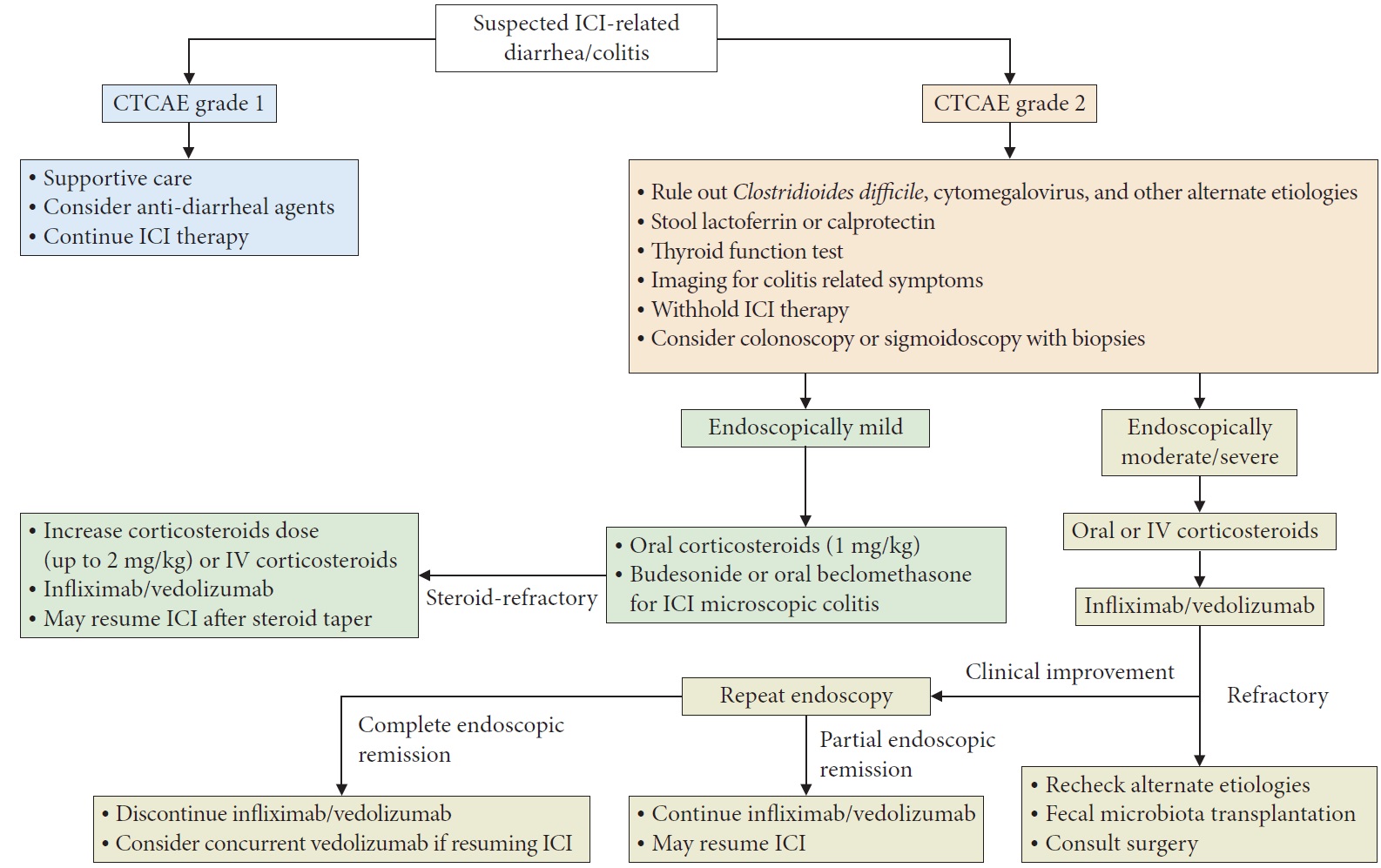
진단과 치료를 요약한 표입니다.
Common terminology criteria for adverse events (CTCAE) grades ver. 5.0 CE 2024
![]() 3. 출혈성 위염
3. 출혈성 위염
아래 환자는 전형적인 checkpoint inhibitor-induced hemorrhagic gastritis의 내시경 소견입니다. 폐암으로 programmed cell death-1 inhibitor pembrolizumab을 사용하던 분입니다. 구역과 속쓰림의 증상이었고 내시경에서는 diffuse한 부종, 발적, friability 등이 보입니다. 저는 가급적 출혈성 위염이라는 용어를 쓰지 말자고 주장하고 있습니다만, checkpoint inhibitor와 관련된 이러한 상황에서는 출혈성 위염이라는 용어가 적합하다고 생각합니다.
출혈성 위염 양상이므로 조직검사가 무서울 수 있습니다. 그러나 이런 경우의 출혈은 peptic ulcer with exposed vessel이나 Dieulafoy ulcer와는 다른 상황입니다. 염증이 있는 점막에서 oozing 되는 양상입니다. 따라서 조직검사를 한다고 대량 출혈이 발생할 확률은 높지 않습니다. 조직학적 증거를 가지고 진단하기 위해서 가급적 2개 정도의 조직검사를 하실 것을 권합니다. Checkpoint inhibitor를 사용하는 환자의 출혈성 위염은 조직검사 합병증 위험보다 정확한 확진이 중요한 상황이니까요.
치료는 steroid이며 호전이 없으면 infliximab을 투여합니다.
[CMV gastritis]
Immune checkpoint inhibitor (Pembrolizumab)를 쓰면 CMV가 activation되어 CMV gastritis가 심하게 올 수 있습니다.
CMV gastritis due to immune checkpoint inhibitor.
흥미로운 그림입니다.
CMV에 대한 치료를 시작하며 immune checkpoint inhibitor (Pembrolizumab)도 끊었습니다. 점차 호전되었습니다. 상세한 설명은 아래 동영상을 참고하시기 바랍니다.
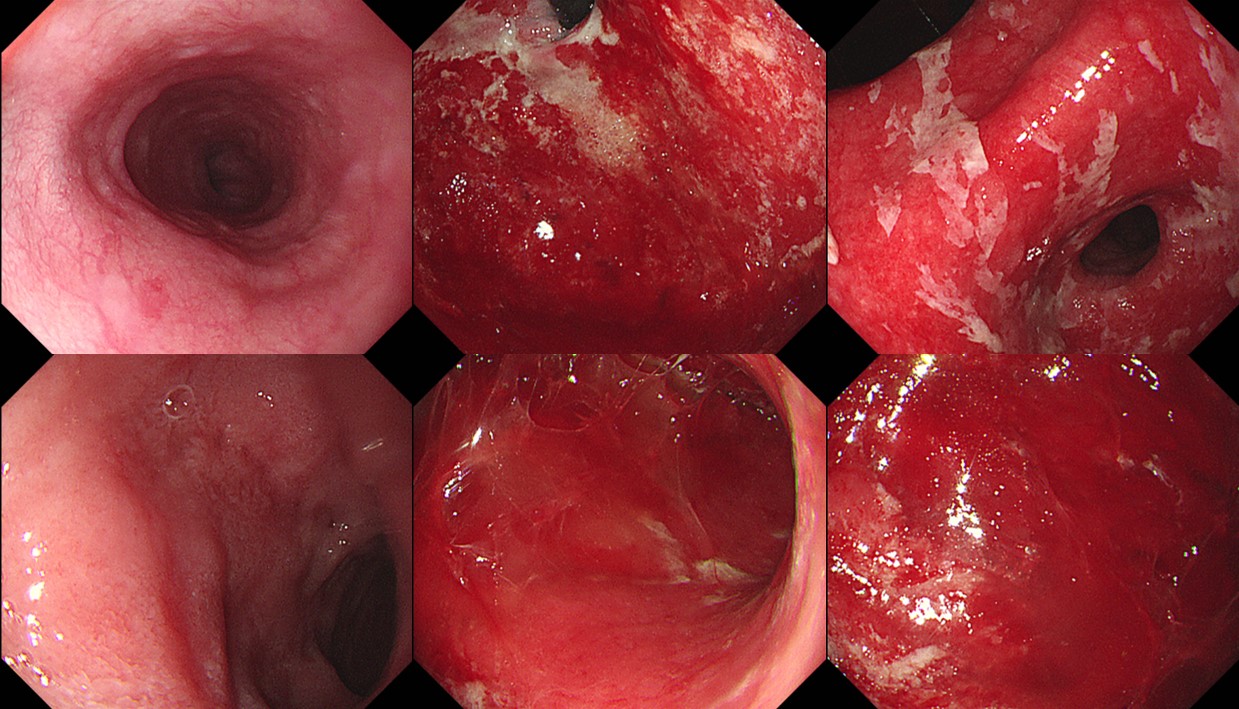
![]() 4. 출혈성 대장염. Immune checkpoint inhibitor-associated colitis 증례
4. 출혈성 대장염. Immune checkpoint inhibitor-associated colitis 증례
HCC
Esophageal cancer
2021년 건국대 이선영 교수님 quiz 중
2020년 7월 2일 내시경 집담회에서 임상강사 권태진 선생님께서 정리한 내용입니다.
ACG Virtual Grand Round 슬라이드에도 해당 내용이 있어서 소개합니다. 좌측 상단 사진과 설명입니다.
![]() 5. 간세포암 atezolizumab + bevacizumab 치료에서 위장관 천공과 출혈
5. 간세포암 atezolizumab + bevacizumab 치료에서 위장관 천공과 출혈
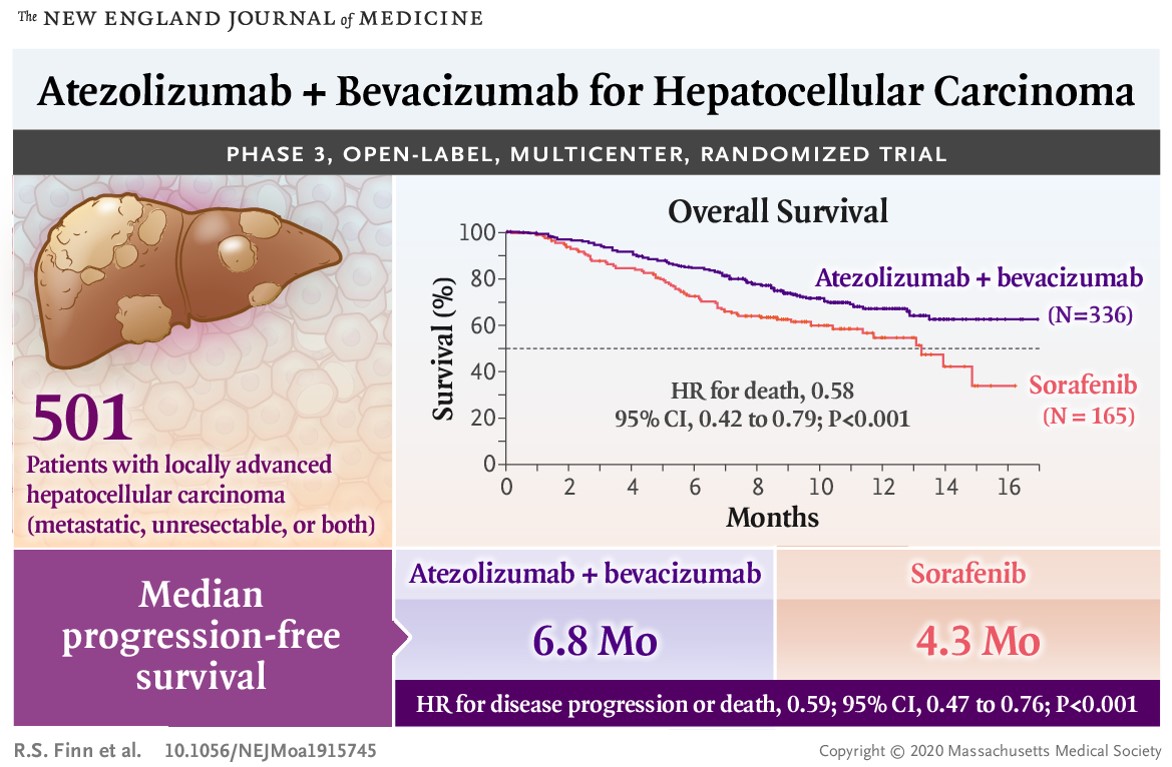
간세포암 항암치료로 sorafenib가 널리 사용되었습니다. 최근 atezolizumab + bevacizumab 치료가 더 효과적이라고 알려졌습니다 (Finn et al. NEJM 2020).
Atezolizumab은 PD-L1에 대한 IgG1 antagonist antibody입니다. Tumor cell의 PD-L1이 activated T cell의 PD-1과 B7.1등과 binding하여 T cell을 inactivation 시키고 tumor를 자라게 하는데 이것을 막으면서 tumor cell의 죽음을 유도하는 약물입니다. Bevacizumab은 VEGFA에 binding하여 VEGF mediated immunosuppression을 줄여주면서 anti PD-1 and anti PD-L1등 immune checkpoint inhibitor의 efficacy를 potentiation시켜서 시너지틱한 effect를 낸다고 합니다. PD-1 inhibitor는 single agent로서는 phase 3 study에서 overall survival을 증가시키지 못하였었습니다.
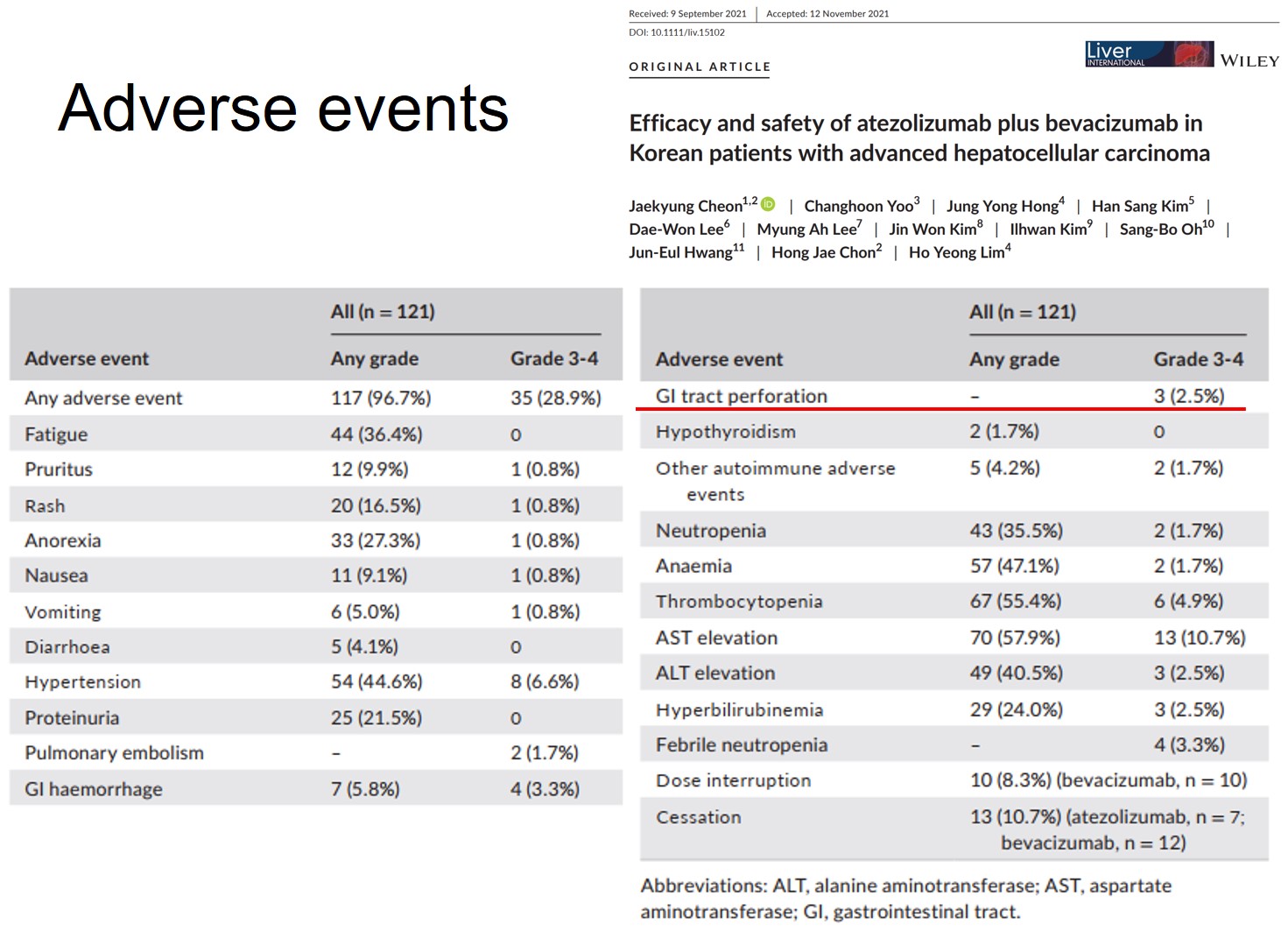
그런데 최근 연구에서 Ate/Beva 치료의 합병증으로 위장관 천공이 제시되었습니다. 간 상태가 좋지 않은 분이므로 일단 위장관 천공이 발생하면 효과적으로 대처하기 어렵습니다. 조금이라고 의심되거나 고위험군으로 생각되면 미리 PPI를 쓰는 것은 어떤가 혼자 생각해 보았습니다.
Bleeding도 문제입니다. Esophageal varix나 gastric varix가 현저할 때 atezolizumab + bevacizumab 치료가 출혈을 일으킬 수 있다는 우려가 제기되고 있습니다.
Targeted Oncology 토론 동영상
최근에는 atezolizumab + bevacizumab 치료 전 varix를 평가하여 어느 정도 이상이면 atezolizumab + bevacizumab 치료 전 band ligation을 할 것을 권하기도 합니다. 따라서 내시경으로 varix를 평가하면서 적절한 grading을 하는 것이 매우 중요한 일이 되고 있습니다.
F2 RC (+)로 평가되었으나 F1 RC (-)로 변경하였던 증례
[2022-4-14] Single topic symposium on esophageal varix grading
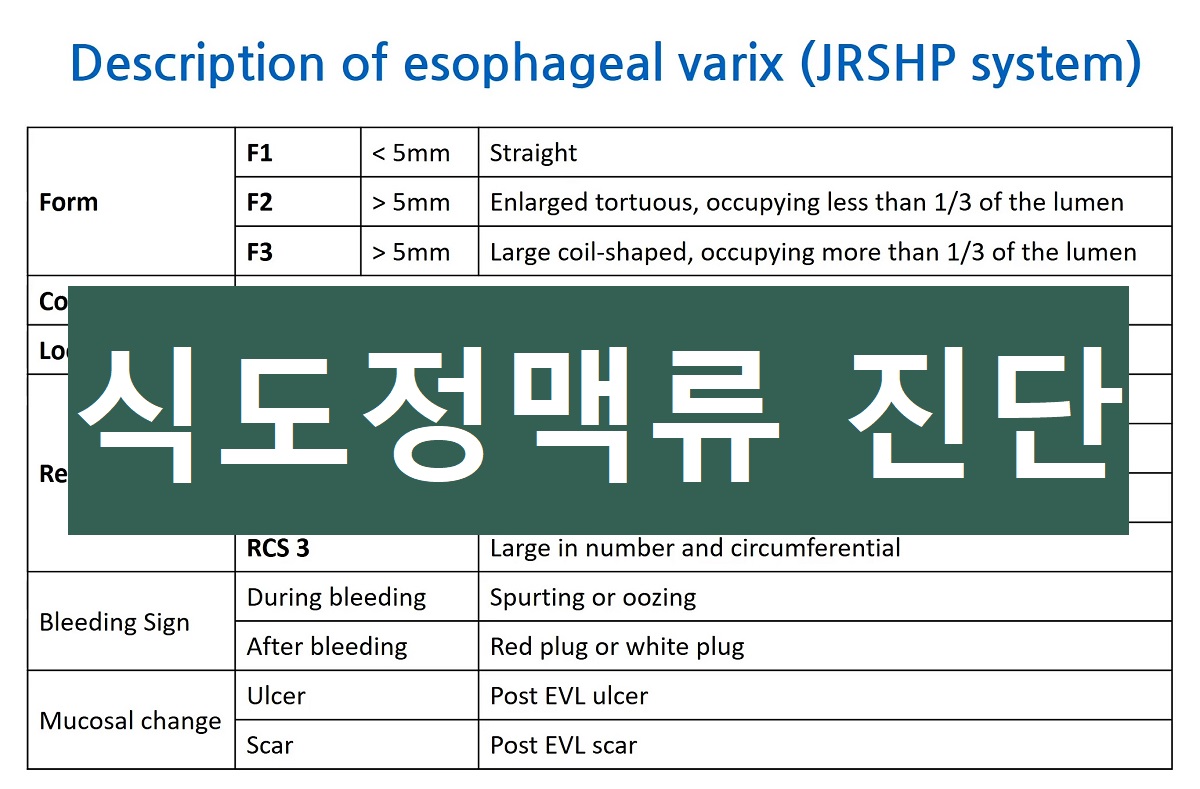
F1 (linear, < 5mm)과 F2 (beaded or tortuous, >5mm)의 구분이 애매하면 F1으로 준다. 약간 beaded 한 모양이더라도 5mm 미만이면 F1으로 준다.
F2와 F3의 구분은 임상적으로 별 차이가 없다.
애매하면 세게 주기보다는 약하게 준다.
EVL을 여러번 시행받은 환자에서는 F1,2,3 구분이 어렵다. 치료가 필요하다고 판단되면 F2, 치료가 필요하지 않다고 판단되면 F1을 주기도 한다. 사진을 잘 찍어두는 것이 중요하다.
![]() 6. 췌담도파트 처방례
6. 췌담도파트 처방례
[2021-1] 췌담도파트에서 시행하고 있는 치료를 소개합니다. 가격 등 보험 조건은 수시로 바뀝니다.
약제: Pembrolizumab
표준 치료에 실패했거나 표준 치료가 적합하지 않은 PD-L1 positive 진행성 담도암, 담낭암 (바터팽대부암)
D1: pembrolizumab 200mg + NaCl 0.9% 100ml (over 30 min)
3주 간격, 2주마다 CBC, chemistry, electrolyte, CA 19-9, chest PA
TSA: baseline, 6주차, 12주차, 18주차
1 cycle: 570만원
Low protein binding 0.2-5 micron in-line filter 사용
![]() [References]
[References]
1) EndoTODAY chimeric antigen receptor-T 세포를 이용한 암 면역치료 CAR-T
2) NK cell 기능 검사와 NK cell 항암 치료제
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng (2020-5-21, update: 2024-11-29)