EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [GERD - 이풍렬 교수님 특강]
[GERD - 이풍렬 교수님 특강]
1. Introduction
2. 위식도역류질환 역학
3. 위식도역류질환 병태생리
4. 위식도역류질환 진단
5. 위식도역류질환 치료
7. 바렛식도
8. Related condition: 트름, supragastric belching, rumination syndrome
9. FAQ
10. References
2018-1-8. 이풍렬 교수님 특강
Seoul Consensus on GERD 2020 PDF 0.6M
![]() 1. Introduction
1. Introduction
이풍렬 교수님의 GERD 특강을 요약하였습니다. 매년 강의해 주시고 계십니다. 감사합니다.
[2019-1-7. 이풍렬 교수님 comment]
"GERD 영역이 발전할 수 있었던 것은 PPI의 역할이 적지 않았습니다. PPI는 1991년 말부터 국내에서 사용되기 시작하였습니다. 그러나, 25년 정도 시간이 흐르면서 PPI 하나만으로 불편한 점이 적지 않다는 것을 이야기하고 있습니다. 최근 (2017년-2018년) 과거의 정의나 진단기준을 다시 검토하기 시작하였습니다. Lyon consensus(Gyawali CP, Gut 2018)라는 중요한 제안이 있었고, Revisiting Montreal이라는 논문(Am J Gastroenterol 2018)도 있었고, PPI 부작용 부분이 개념 정리가 되었고 (Nature Review 2017), P-CAB이라는 새로운 약도 나오면서 오랫동안 조용하던 GERD 영역이 갑자기 hot해졌습니다.
![]() 2. 위식도역류질환 역학
2. 위식도역류질환 역학
정의는 Montreal 정의를 이용합니다.
분류는 LA classification을 따릅니다. Minimal change는 역류성 식도염으로 간주하지 않습니다.
위식도역류질환, 바렛식도, 바렛식도암쪽으로 갈수록 men, western, white 비중이 높습니다. 최근에는 men, western, white가 obesity라는 보다 중요한 위험인자로 환원되고 있습니다. 서양인이 아니더라도, 남자가 아니더라도, central obesity가 있으면 GERD 발생 위험이 높습니다.
우리나라를 포함하여 아시아에서 바렛식도가 뚜렷하게 증가하고 있다는 증거는 부족합니다. 오직 일본에서만 높게 나오고 있는데, 일본의 바렛식도 진단기준이 특이하기 때문입니다. 비만 유병률도 높아지고 있습니다. 우리나라도 조만간 높아질 가능성도 있습니다.
일본 빼고는 식도 선암이 증가하였다는 증거는 부족합니다. 그러나 향후 높아질 가능성은 있습니다.
![]() 3. 위식도역류질환 병태생리
3. 위식도역류질환 병태생리
위식도역류질환의 공격인자와 방어인자의 관계
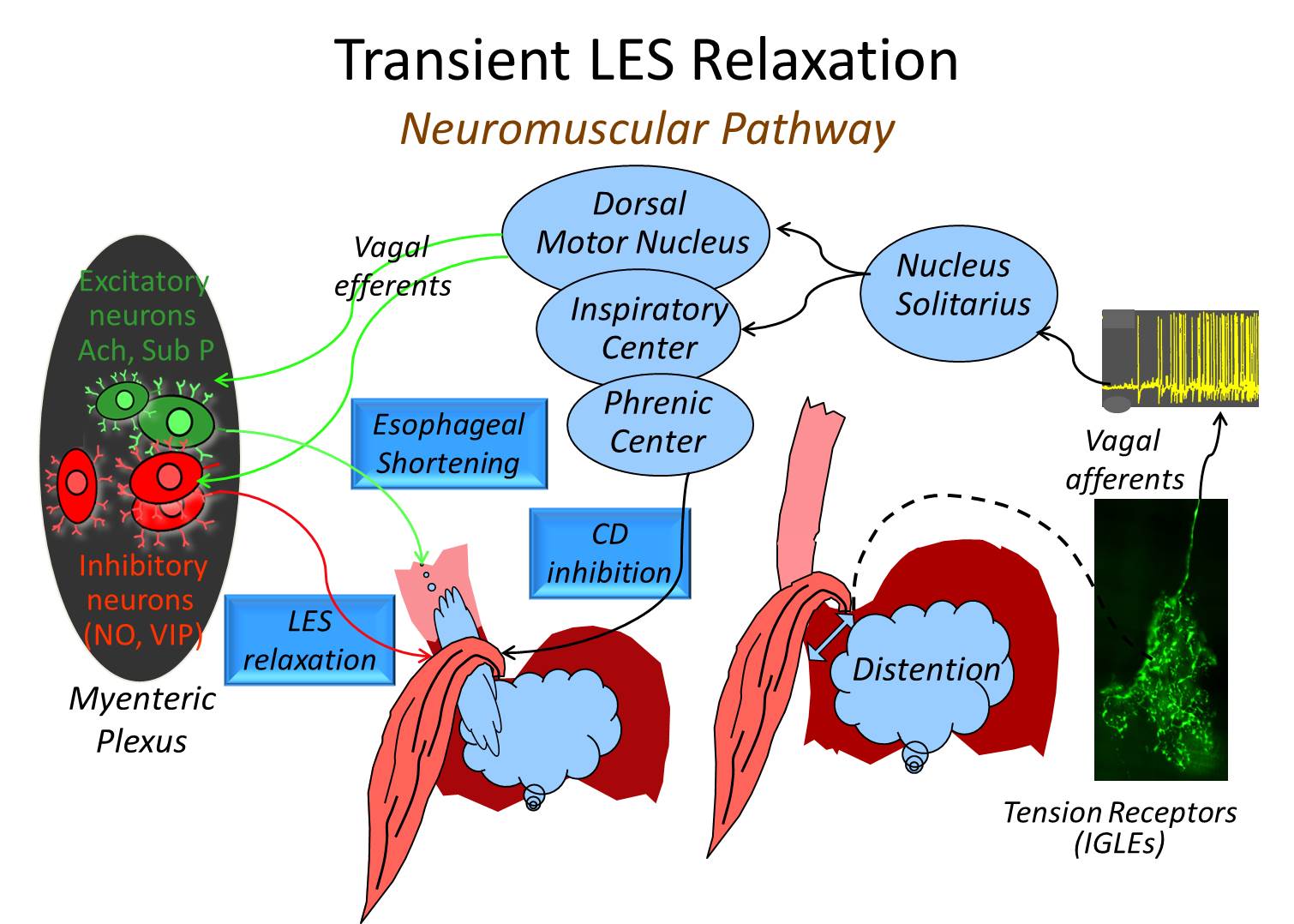
1) 병태생리 중 tLESR은 꼭 아셔야 합니다. 위 확장(gastric distention)에 따른 vagal reflex입니다. 그러나 tLESR에 대한 모든 약은 효과가 신통치 않았습니다. 최근 비만의 중요성이 강조되고 있습니다.
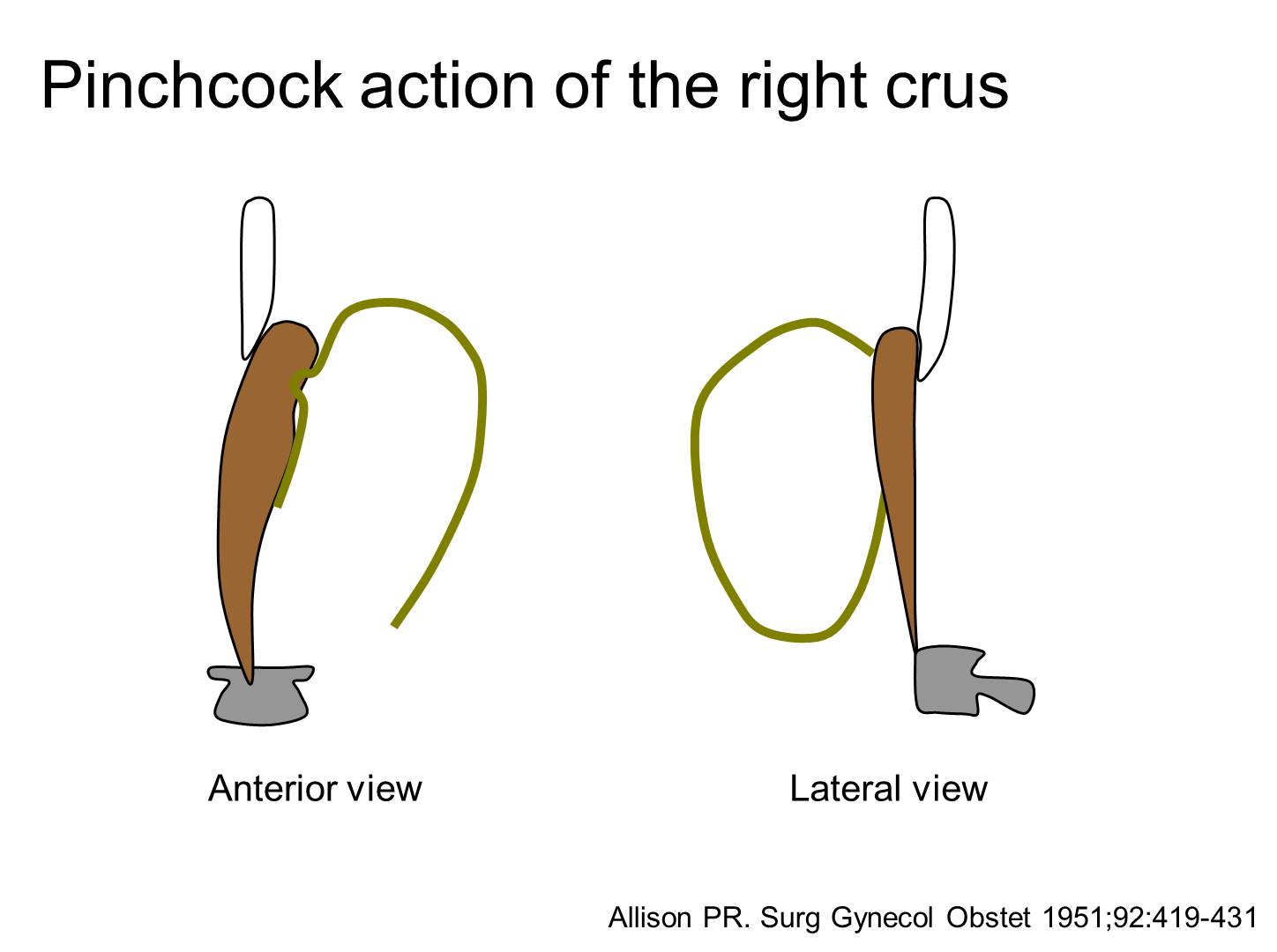
2) 횡경막
Right crus가 sling-like하게 식도를 감싸고 있습니다. 복부 비만에 의하여 복부가 팽창되면 diaphragm이 늘어나면서 hiatal opening도 늘어납니다.
3) Flap valve의 중요성이 강조되고 있습니다.
Opposing sling and clasp muscle fibers. The longitudinal muscle layer of the stomach has been cut away to show the opposing sling and clasp muscle fibers. These fibers sit in tonic opposition until a swallow triggers receptive relaxation. It is thought that progressive stretching of these fibers leads to valve incompetence and subsequent GERD. (Jobe BA. Am J Gastroenterol 2004)
Intraabdominal esophagus의 angle of His가 예각을 유지하면서 효과적인 flap valve를 형성하고 있는 모습.
Sling fiber와 clasp fiber가 협조하여 효과적인 flap valve를 형성하고 있는 모습
Angle of His가 둔각이 되면서 flap valve 기능을 잃음.
Angle of His가 둔각이 되고, hiatus가 넓어지고, intraabdominal esophagus가 상승하면 sliding hiatal hernia가 됨.
오래 전 제안된 Hill grade에 대한 관심이 최근 점차 높아지고 있습니다.
4) Acid pocket - 식후에 위산역류 증상이 흔한 paradox에 대한 좋은 설명입니다. 식후 새로 만들어진 위산이 acid pocket에 모이는 현상입니다.
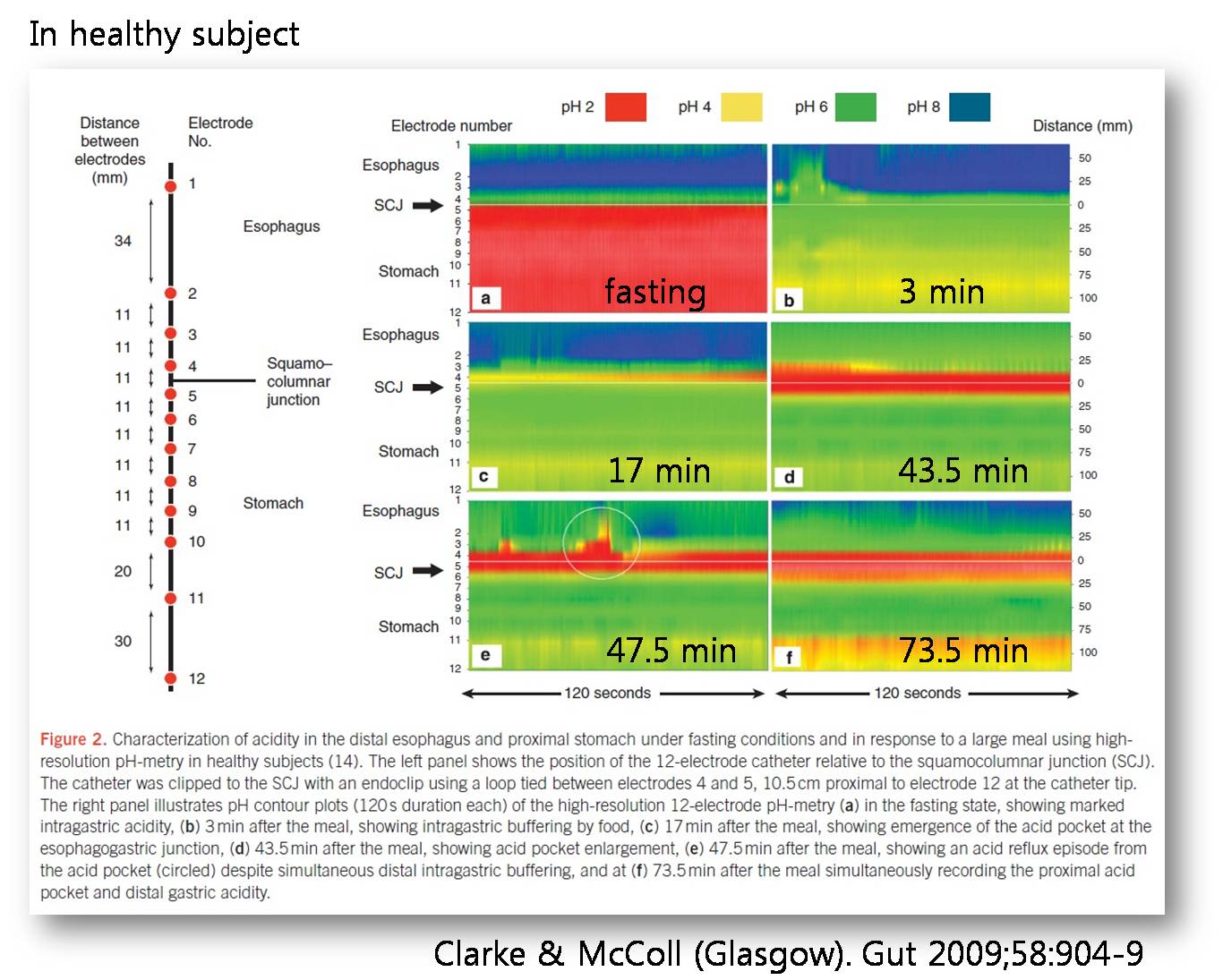
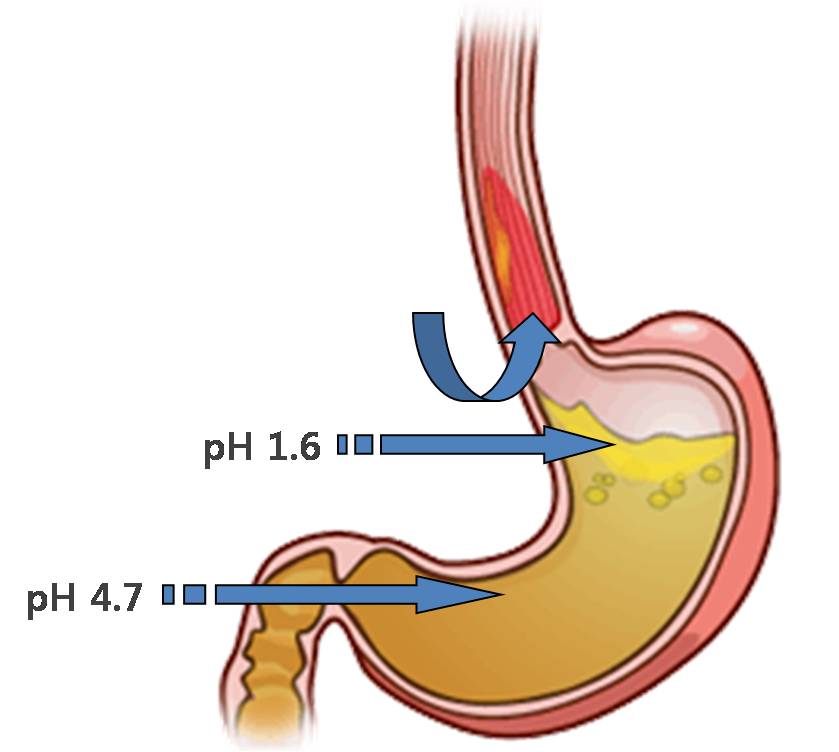
Acid pocket이 diaphragm보다 위쪽에 위치하면 (= hiatal hernia) 위산이 역류하기 쉬운 상태가 됩니다.
5) 식도 체부의 기능이상
6) 비만 - 더 이상 비만과 GERD 관련성에 대한 논문은 나오지 않습니다. 너무나 명확하게 확립되었기 때문입니다.
마른 환자, 복부 지방이 없는 환자에서 hiatal hernia가 있는 경우는 아직도 고민입니다. ('농사하는 할머니 syndrome'이라고 주장하는 일본 의사도 있습니다.)
7) 헬리코박터
과거에는 헬리코박터가 GERD에 대한 protective effect가 있다고 말한 적이 있지만, 앞으로는 절대로 이런 말을 쓰면 안되겠습니다. 사실 인체에 좋은 헬리코박터는 없습니다. 헬리코박터 감염에 의한 위축성 위염의 결과 위산분비가 줄어 GERD 증상이 다소 덜한 것은 사실이지만 "protective effect"라는 말은 부적절합니다.
최근에는 이 모든 인자를 종합하여 생리적인 방어인자의 지속적인 파괴에 따른 역류발생 및 악화를 중요하게 생각하는 '위식도역류질환의 개념적 모델'로 통합되었습니다. 악화인자 중 obesity와 diet가 조절할 수 있는 요소입니다.
![]() 4. 위식도역류질환 진단
4. 위식도역류질환 진단
Lyon consensus (Gut 2018)를 통하여 GERD의 개념이 다시 한번 정리되었습니다. LA-A 혹은 LA-B의 역류성 식도염은 pathologic reflux의 conclusive evidence에서 배제되었습니다.
Interpretation of oesophageal test results in the context of GERD. Any one conclusive finding provides strong evidence for the presence of GERD. While a normal EGD does not exclude GERD on its own, this provides strong evidence against GERD when combined with AET <4% and <40 reflux episodes on pH-impedance monitoring off proton pump inhibitor therapy. When evidence is inconclusive or borderline, adjunctive or supportive findings can add confidence to the presence or absence of GERD. Histopathology as an adjunctive measure requires a dedicated scoring system (incorporating papillary elongation, basal cell hyperplasia, DIS, intraepithelial inflammatory cells, necrosis and erosions) or evidence of DIS on electron microscopy. However, adjunctive findings, particularly histopathology and motor findings in isolation, are not enough to diagnose GERD. AET, acid exposure time; DIS, dilated intercellular spaces; MNBI, mean nocturnal baseline impedance; HRM, high-resolution manometry; PSPWI index, postreflux swallow-induced peristaltic wave index; EGJ, oesophagogastric junction. *Factors that increase confidence for presence of pathological reflux when evidence is otherwise borderline or inconclusive. (Gut 2018)
[2019-1-17. 이준행 comment]
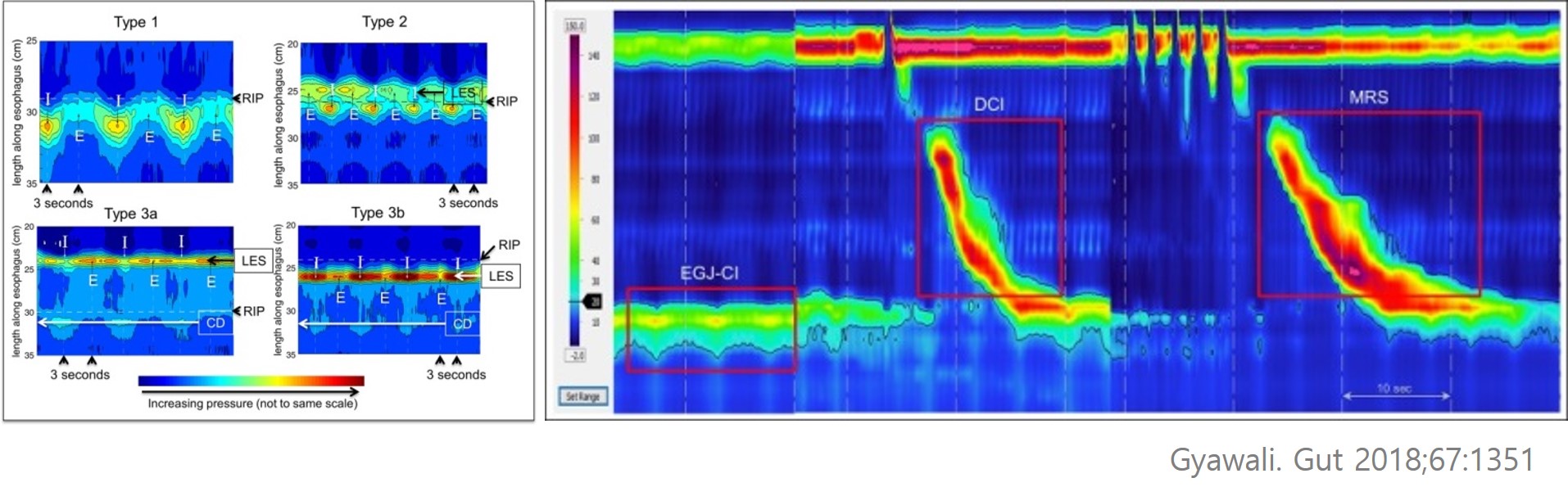
Lyon consensus(Gyawali CP, Gut 2018)에 대하여 잠시 생각해 봅니다. 이러한 consensus meeting이 있었던 것은 Montreal definition 따라 증상 기반으로 PPI를 쓰는 것은 GERD overdiagnosis와 PPI overuse를 가져왔다는 문제의식에 기인합니다. Lyon consesnsus에서는 크게 두 가지가 강조되고 있습니다. (1) Symptom-based GERD diagnosis와 physiology-based GERD diagnosis가 일치하지 않는 경우가 많고 (sensitivity와 specificity가 70% 혹은 그 이하), (2) GERD의 subtype 구분을 위하여 적절한 physiology study가 필요하다는 점입니다. High resolution manometry와 impedence 검사가 강조되었는데 EG junction anatomy와 physiology의 객관화가 핵심인 것 같습니다. EGJ contractility의 85% 를 crural diaphragm (CD)이 담당하므로 EGJ anatomy가 중요하고, EGJ contractile integral이 유망한 지표로 제시될 수 밖에 없습니다.
그러나 Lyon consensus에서는 그 흔한 algorithm을 하나도 제시하지 않았습니다. 아마도 제시하지 못했다고 하는 것이 맞겠지요. 하나의 질환으로 묶였을 때 하나의 algorithm이 나오는 것이지 여러 질환이 대강 섞인 상황이라는 것이 명백한데 어찌 하나의 algorithm으로 정리할 수 있겠습니까. Lyon consesnsus의 저자들은 이러한 사실을 명백하게 밝히지 않고 특유의 완곡어법으로 빙빙 돌려서 표현하고 있을 뿐입니다. "No single approach is perfect"라고 선언하면서 "The goal of evaluation should therefore transition toward defining GERD phenotypes to facilitate tailored treatment"라는 매우 애매한 문장으로 마무리하였더군요. 저는 GERD라는 것을 하나의 algorithm으로 정리할 수 없는 heterogenous한 질환의 모임으로 생각합니다. PPI의 약효에 놀라서 GERD를 하나의 질환으로 오해하였던 전문가들이 이제 슬슬 제정신을 찾고 중립적인 입장에서 초심으로 돌아가는 모양새입니다. 바람직하다고 생각합니다. 오래전부터 주장하고 있는 바이지만 PPI 혹은 P-CAB을 단기간 사용한 후 깜짝 놀랄만큼 증상이 좋아지는 환자는 GERD로 보고 그렇지 않으면 physiology test를 통하여 subtype을 규명하기 위하여 노력해야 할 것 같습니다. 저의 point는 "깜짝 놀랄만큼"입니다. 애매하게 좋아지는 것 말로 깜짝 놀랄만큼 좋아져야 합니다. (2019-1-17. GI ASCO에 참석하기 위하여 미국으로 날아가는 대한항공 economy 석에서 쪼그리고 앉아 썼습니다. 거의 10년 만에 장거리 비행을 하느라 미칠 지경입니다. 저는 2시간 이상의 비행을 끔찍히 싫어합니다.)
![]() 5. 위식도역류질환 치료
5. 위식도역류질환 치료
증상에 따라서 PPI에 대한 반응이 다릅니다. PPI에 반응하는 환자를 선별하여 투약하고 PPI에 반응하지 않는 사람에서는 빨리 약을 끊어주어야 합니다.
위식도역류질환하면 역류성식도염으로 생각했던 시절에는 역류성식도염의 점막병변의 치유(healing)가 치료의 목표였기 때문에 80년대 후반 위산분비억제제(PPI)가 개발되었을 때 이러한 목표는 쉽게 달성될 수 있었다.
대부분의 나라에서 이때문에 외과적 위분문부성형술(surgical fundoplication)과 같은 다른 방식의 치료요구도 급격히 감소하였다.
그러나 최근에 문제가 되는것은 PPI치료에도 불구하고 역류증상이 지속되거나 식도염 없이 증상이 발생하는 등의 문제 이다.
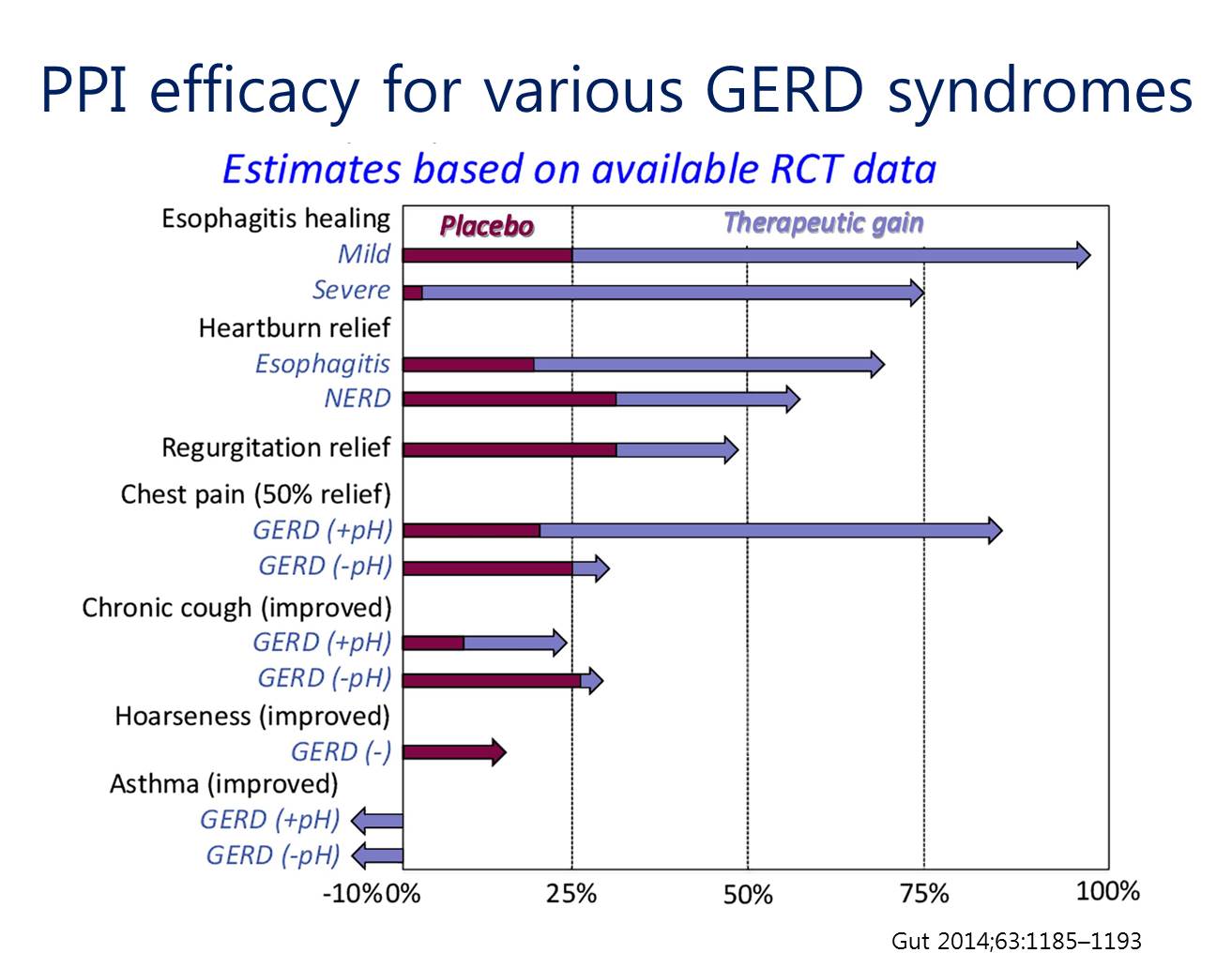
그리고 위산분비억제제(PPI)에 대한 효용성은 식도염, 가슴쓰림증상(symptomatic heartburn), 역류(regurgitation), 흉통(chest pain), 기침(cough), 인두염(laryngitis) and 천식(asthma) 순으로 급격히 떨어진다.
Revisiting Montreal이라는 흥미로운 리뷰가 있습니다. "With one third of "typical" symptoms known to be refractory" 및 "Mechanisms underlying GERD, RH, and FH are (in theory) not mutally exclusive"라고 전제하면서 아래와 같이 매우 도전적인 그림 두 개를 소개하고 있습니다. Scale에 따른 position은 아니라지만 그나마 heartburn이 PPI에 반응하고 regurgitation, chest pain, cough 순서로 반응이 떨어진다는 점을 정확히 지적하고 있습니다. Heartburn도 subtype에 따른 차이가 있음을 그 다음 그림에서 보여줍니다.
Suspected gastroesophageal reflux disease (GERD)-related symptoms, their relative likelihood of response to acid-suppressive therapy based on the literature, and the presumed importance of acid reflux for symptom generation based on these findings. Smaller arrows underneath each symptom indicate the direction of the shift in response to acid suppression when patients are selected based on the presence (RE+) or absence (RE-) of reflux esophagitis, or the presence (pH+) or absence (pH-) of pathologic esophageal acid exposure. The relative position of each symptom and the size of the arrows is not to scale. In summary, heartburn is assumed to be the quintessential acid-related symptom and as such correlates the most frequently with pathologic esophageal acid exposure and response to acid-suppressive therapy. The response of heartburn (and regurgitation) to acid suppression is higher in RE+ patients than in RE- patients, concordant with RE being a good proxy for pathologic esophageal acid exposure in lieu of pH-testing. The relative response of symptoms to acid suppression decreases as their dependence on pathologic esophageal acid exposure decreases. However, even for symptoms such as chest pain and cough, response rates to acid suppression can be enhanced by identifying patients who have pathologic esophageal acid exposure (pH+), albeit with a dwindling effect as symptom etiology becomes increasingly multifactorial
Relationship between reflux acidity, response of heartburn to acid-suppressive therapy and the role of peripheral and/or central esophageal hypersensitivity in different gastroesophageal reflux disease (GERD) and non-GERD patients with heartburn. Reflux esophagitis (RE) correlates strongly with the presence of pathologic esophageal acid exposure and, concomitantly, healing of RE and heartburn resolution are high with acid-suppressive therapy in these patients. Some patients have heartburn but not RE. Those who have pathologic esophageal acid exposure (pH+) have NERD, and heartburn symptoms respond as well to acid suppression as they do in patients with RE. Those patients with heartburn who do not have pathologic esophageal acid exposure may still have a positive symptom association probability (SAP+) for acid or non-acid reflux, and are thus categorized as having reflux hypersensitivity (acid hypersensitive esophagus (AHE) or non-acid hypersensitive esophagus (NAHE)). Patients without pathologic acid exposure who have a negative SAP are designated as having functional heartburn (FH). The role of peripheral and/or central esophageal hypersensitivity increases as dependence on acid reflux (and response to acid suppression) decreases, in line with heartburn perception occurring despite non-pathologic acid reflux (hyperalgesia) in patients with reflux hypersensitivity, or under physiological reflux conditions (allodynia) in patients with FH.
Life style modification에서 가장 중요한 것은 비만 치료입니다. 체질량지수가 3.5kg/m2 감소되면 (= 대략 10kg 감량) GERD의 위험도가 40%나 감소한다. 일반적인 음식은 크게 제한하지 않습니다. 본인이 드시고 불편하면 그 음식만 피하면 됩니다.
PPI and adverse events with proven and unproven causality에 대한 검토가 있었고 (1) structural and functional changes in the gastric mucosa, (2) acute kidney injury, (3) enteric infection 세가지는 연관성이 있다고 개념이 정리되었습니다. (Nature Review 2017)
PPI를 longterm으로 사용하려면 definite absolute indication이 있어야 합니다. Definite absolute indication이 없으면 함부로 longterm으로 사용하면 안 됩니다. 이풍렬 APDW
수술은 high dose PPI와 효과가 비슷합니다. 그러나 수술은 mortality가 있고 complication을 고려해야 합니다. 따라서 일반적으로는 내과 치료가 우선이고 hiatal hernia가 현저한 경우, 젊은 사람의 경우 physilogy를 잘 알고, 수술의 경험이 많은 외과의사에게 수술을 권해볼 수 있습니다.
[2019-1-7. 이풍렬 교수님 comment]
복부 비만을 가진 GERD 환자에서 PPI만 드리면 의사의 직무유기입니다. 비만을 평가하고 적극적인 비만 관리를 환자에게 강력히 추천해야 합니다.
과거는 Compliance는 어떻고 metabolism이 어떻다는 등 환자 탓을 많이 했습니다. 최근에는 진단을 다시 살펴볼 것을 추천합니다. pH-impedence 검사를 해 볼 필요가 있습니다.
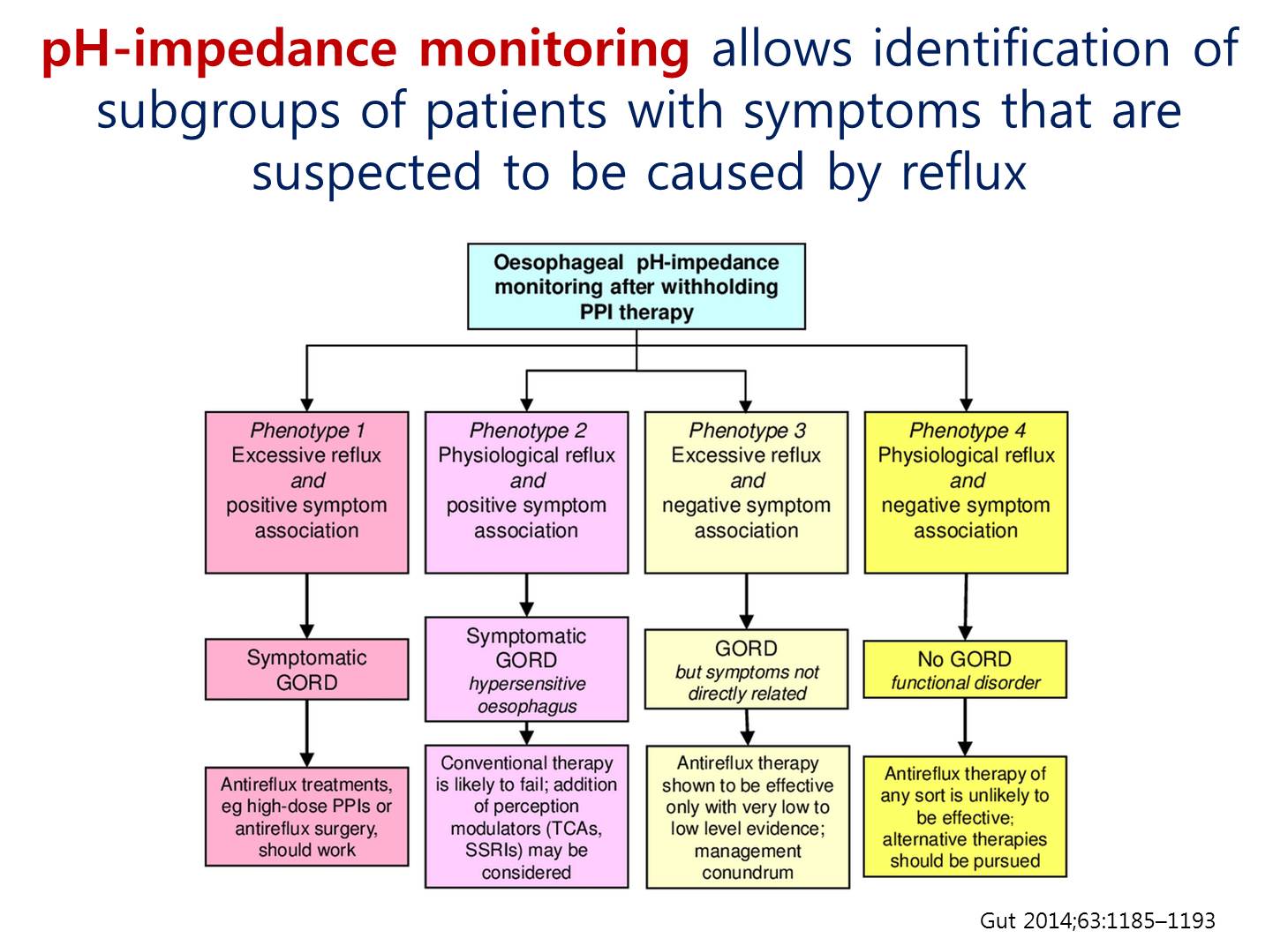
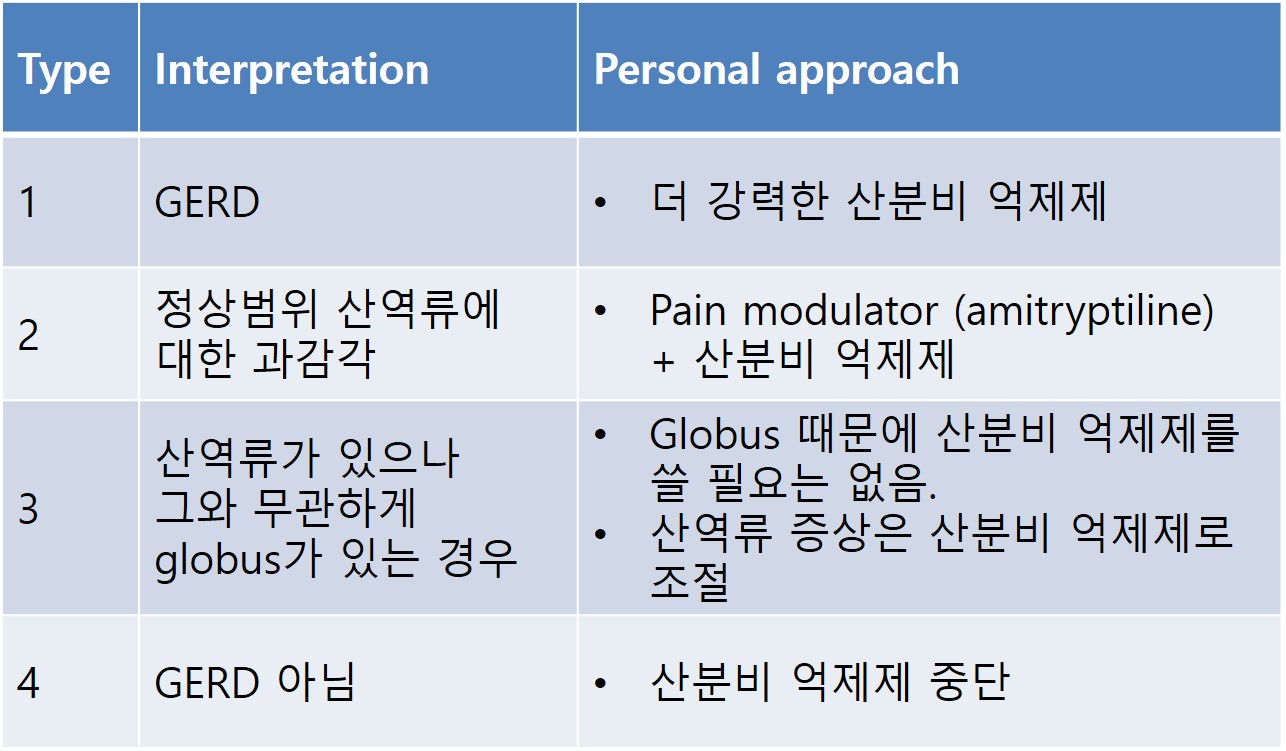
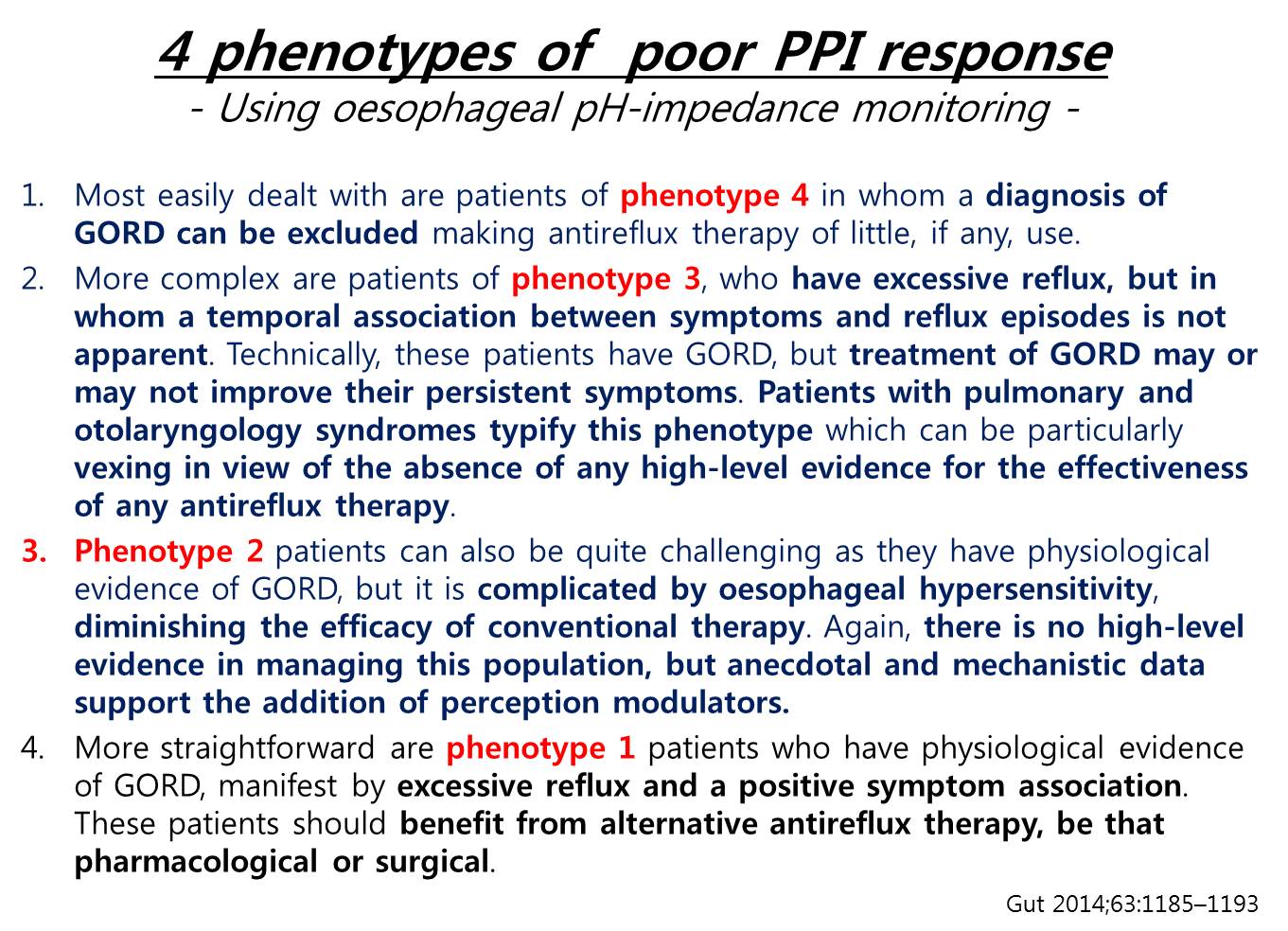
pH-impedence 검사를 통하여 4개의 phenotype으로 나눌 수 있습니다. 1형은 위산을 더욱 강력하게 억제해야 합니다. 2형은 위산에 대한 식도과민성입니다. TCA나 SSRI등을 쓸 수 있습니다. 3형은 산역류는 있으나 증상은 이와 무관한 경우입니다. 3형에서 산역류와 관련된 증상(heartburn)과 산역류와 관련되지 않는 증상(globus)을 함께 가질 수 있습니다. 이런 경우 PPI를 주면 산역류 증상은 좋아지지만 globus는 좋아지지 않습니다. Globus가 PPI 반응이 없을 것임을 미리 설명하여 이해시키면 환자가 안심을 하면서 증상이 저절로 좋아지기도 합니다. 4형은 GERD가 아니므로 모든 약을 끊어야 합니다.
Phenotype 2는 간단합니다. 산역류는 증상이나 symptom association이 있는 경우입니다. 정상 범위의 산역류에 대한 과감각이 있는 경우이므로 기본적으로 PPI를 주면서 pain modulator를 함께 써 주는 것이 좋습니다. 가장 안전한 amitryptiline을 사용하고 있습니다.
Phenotype 3는 복잡합니다. 산역류는 있으나 그와 무관하게 globus가 있는 경우입니다. Globus 증상과 관련성이 없는 것입니다. 일단 약을 끊고 산역류 증상만 관리하시면 됩니다.
Phenotype 3, 4에서는 PPI를 끊어주는 것이 정답입니다. 대부분의 extraesophageal symptom이 여기에 해당합니다.
[2017-10-25. 이풍렬 교수님 comment]
[2019-1-7. 이풍렬 교수님 comment]
PPI 약을 수년간 복용하고 있으나 약물반응이 뚜렷하지 않은 분들이 많습니다. 과거에 한번은 반응이 있었으나 그 이후 반응이 없다면 사실 그 환자는 PPI response가 없는 것입니다. GERD라는 진단은 오진입니다.
이준행 comment: 이풍렬 교수님의 강의를 들으면서 제 나름대로 다시 정리해 보았습니다.
* 참고: EndoTODAY Refractory GERD
![]() 7. 바렛 식도
7. 바렛 식도
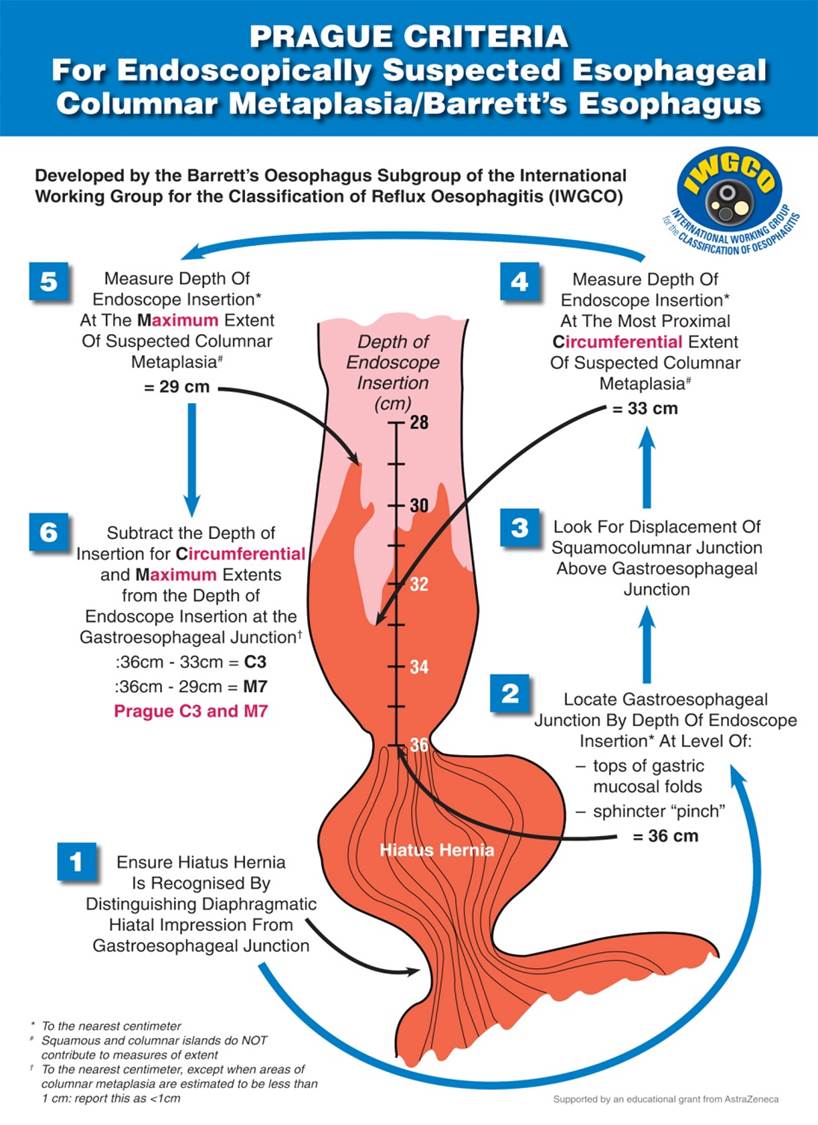
바렛 식도의 진단에는 반드시 specialized intestinal metaplasia(SIM)가 확인되어야 합니다. 즉 goblet cell이 관찰되어야 합니다. SIM이 없는 경우는 columnar lined esophagus (CLE)로 불러야 합니다.
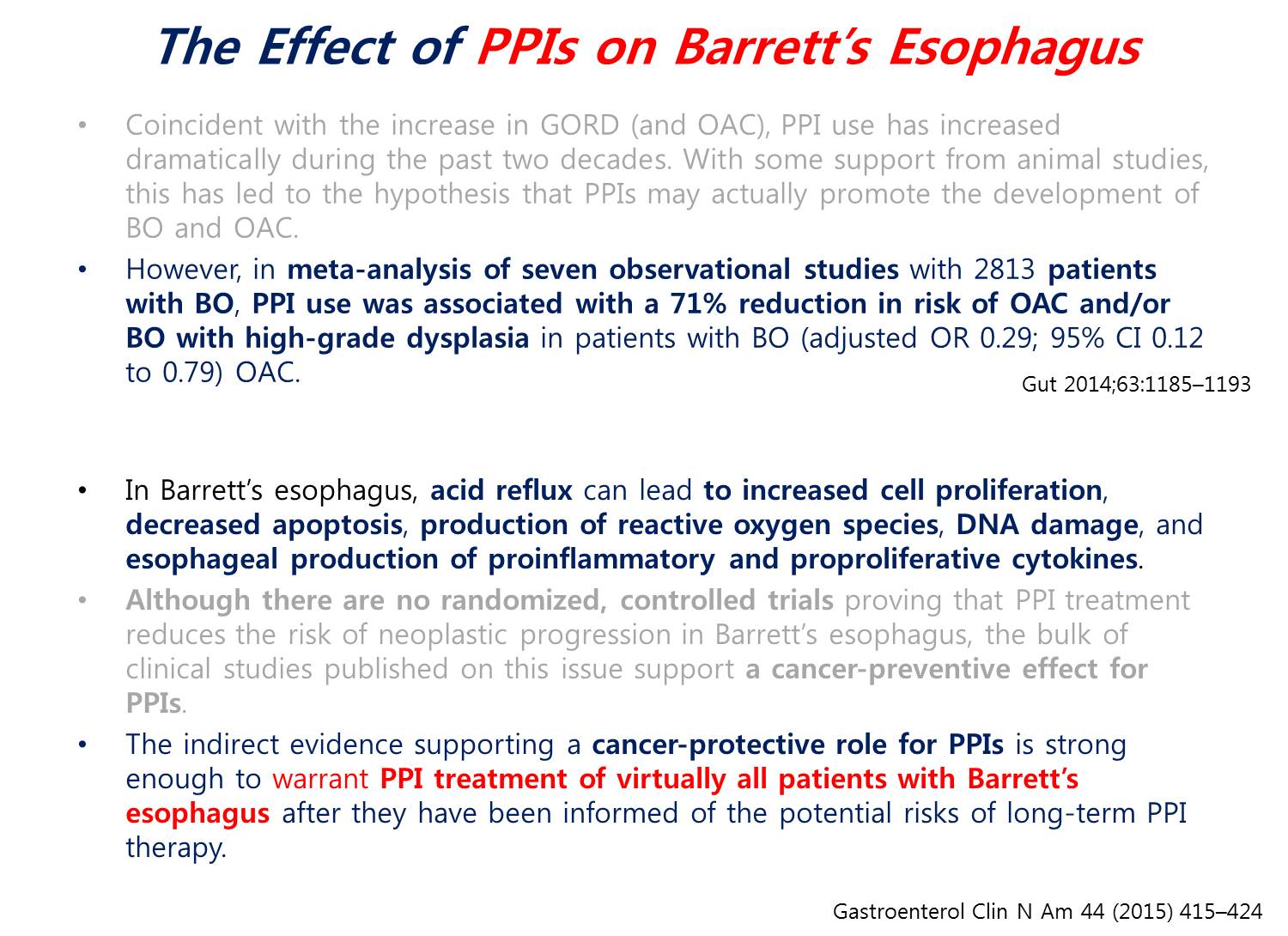
과거에는 바렛이 있어도 산역류가 있는 경우만 PPI를 투여했습니다. 최근에는 개념이 바뀌었습니다. 바렛과 산역류의 관련성이 관심을 끌고 있습니다. 아직 대규모 연구는 부족하지만 이제는 바렛이 있으면 증상이 없더라도 PPI를 투여하는 쪽으로 이야기가 모이고 있습니다. 식도선암이나 고도이형성증의 위험도를 71% 감소한다는 메타분석이 있습니다 (Gut 2014;63:1185).
비록 randomized study는 없으나 바렛 식도에서 PPI 사용의 긍정적 효과는 충분히 입증되어 있습니다.
![]() 8. Related condition: 트름, supragastric belching, rumination syndrome
8. Related condition: 트름, supragastric belching, rumination syndrome
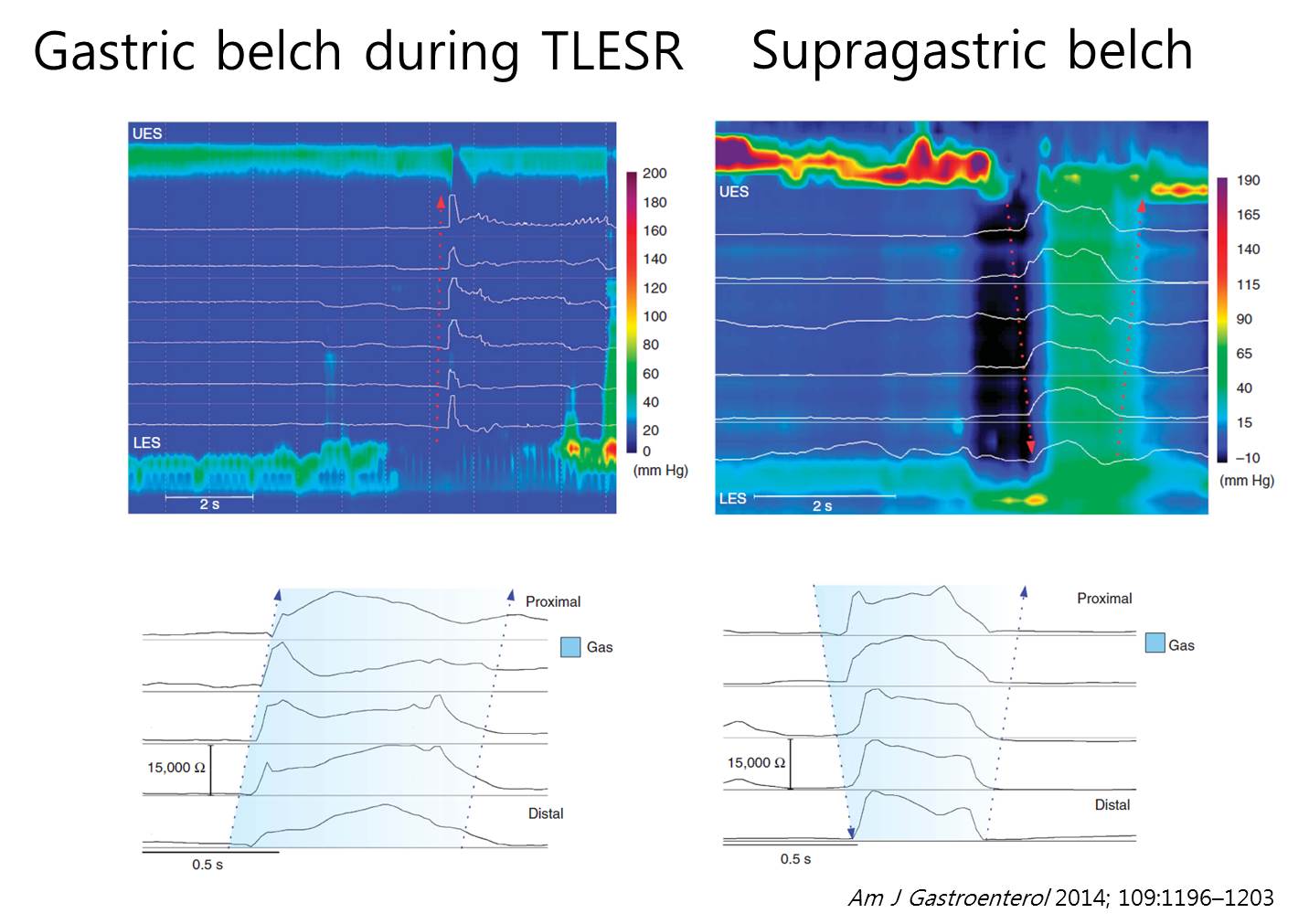
LES relaxation을 동반하는 것이 트름입니다.
Supragastric belching은 트름 같으나 트름이 아닙니다. 식도 압력을 낮춰 공기를 흡입한 후 공기를 뱉는 것입니다. 물론 rumination에 산역류가 동반될 수 있습니다. Behavioral disorder 입니다. 복식 호흡, biofeedback이 도움이 됩니다.
Rumination syndrome. 식후 30분 - 1시간에 되새김을 합니다. 자다가 되새김하는 경우가 없습니다. 정확한 진단과 설명이 중요합니다. 참아야하고 복식호흡을 권합니다. 특히 식후 1시간 동안 눕지 말고 복식호흡을 해야 합니다.
![]() [FAQ]
[FAQ]
[2018-1-8. 질문]
Rome IV에서 reflux hypersensitivity가 어느 정도의 의미를 가지는 category인가에 대한 의문입니다. 검사 도중 환자가 버튼을 누르면 reflux hypersensitivity (= positive symptom association)로, 버튼을 누르지 않으면 functional heartburn (= negative symptom association)으로 구분됩니다.
[2018-1-8. 이풍렬 교수님 답변]
검사 전에 정확한 버튼을 누르는 것이 얼마나 중요한지 잘 설명해 주는 수 밖에 없을 것 같습니다.
[2018-1-8. 질문]
P-CAB의 전망은 어떠합니까.
[2018-1-8. 이풍렬 교수님 답변]
P-CAB은 onset이 빠르고 위산분비 억제가 강력하므로 효과는 좋은데, 부작용이 걱정입니다. LFT 이상이 자주 발견됩니다. 현재의 유용성은 두 가지입니다. (1) Refractory GERD type 1에서 도움이 되고, (2) 헬리코박터 제균치료에 도움이 될 것 같습니다.
[2019-1-7. 질문]
P-CAB 계열의 신약이 국내에서 개발되어 곧 launching 되는 것으로 알고 있습니다 (K-CAB). GERD의 치료에 어떠한 역할을 담당할 수 있을 것으로 생각하시는지요?
[2019-1-7. 이풍렬 교수님 답변]
Promising 한 면도 있고 우려스러운 면도 있습니다. PPI를 써서 약이 안 들어쓸 때 고민할 것이 10가지 정도 있습니다만, P-CAB에서는 이런 고민이 없습니다. Effect가 바로 definite하게 나타나는 장점이 있습니다. (1) Compliance만 확실하면 위산 억제가 보장됩니다. (2) fast onset은 틀림없습니다. (3) 음식과 무관하게 복용할 수 있습니다. 그리고 Helicobacter 제균치료에 도움이 됩니다. (1) Side effect에 대하여 조금 더 살펴볼 필요가 있습니다. Hepatotoxicity에 대한 우려가 없어지려면 조금 더 경험이 필요합니다. (2) Acid-related complication도 장기적으로 살펴보아야 합니다.
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.