EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Thursday Endoscopy Conference 20180510. 송병근 선생님]
[Thursday Endoscopy Conference 20180510. 송병근 선생님]
![]() 1. Rectal carcinoid with lymph node metastasis
1. Rectal carcinoid with lymph node metastasis
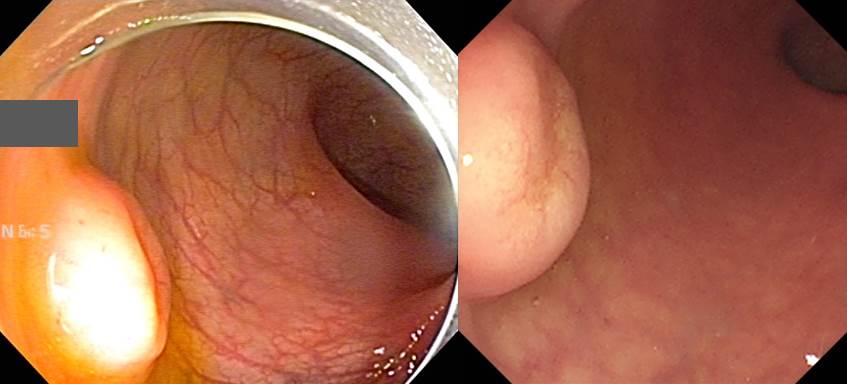
Rectal carcinoid로 의뢰된 환자입니다.
ESD가 시행되었고 병리소견에서 lymphatic invasion이 의심되었습니다.

Well differentiated neuroendocrine tumor (CARCINOID) (G1)
1) size: 1.2x1.0 cm
2) confined to mucosa and submucosa
3) mitosis: 1/10 HPF
4) lymphovascular invasion: suspicious (in one focus)
5) perineural invasion: absent
6) focal involvement of deep cauterized resection margin
수술을 시행하였고 아래의 결과였습니다.
Rectum, low anterior resection : Status post endoscopic submucosal dissection for well-differentiated neuroendocrine tumor
. No residual tumor
. Histologic type and grade: not identified (no residual tumor):
1. Location: rectum
2. Gross type: scar
3. Size: cannot be determined (no residual tumor)
4. Depth of invasion: cannot be determined (no residual tumor)
5. Resection margin: free from carcinoma (no residual tumor) safety margin: proximal, 9.2 cm; distal, 0.5 cm; circumferential (radial), >10 mm
6. Lymphovascular invasion: cannot be determined (no residual tumor)
7. Perineural invasion: cannot be determined (no residual tumor)
8. Regional lymph node metastasis: metastasis to 1 out of 12 regional lymph nodes (1/12: perirectal, 1/12)
직장 유암종 내시경 치료에서는 병리과 선생님이 매우 매우 매우 매우 중요합니다.
![]() [References]
[References]
1) SMC Endoscopy Unit 삼성서울병원 내시경실
2) SMC Monday GI conference 삼성서울병원 일원내시경교실 월요점심소화기집담회
3) SMC Thursday endoscopy conference 삼성서울병원 일원내시경교실 목요점심내시경집담회
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.