 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [ESD for EGC with undifferentiated-type histology]
[ESD for EGC with undifferentiated-type histology]
![]() 1. Current status (2018-4)
1. Current status (2018-4)
[임시 프로토콜 (2018-4)]
내시경적으로 1 cm 이하의 Signet/poorly-differentiated EGC에 대해서는 ESD를 시도할 수 있다고 외과 교수님들과 협의하였습니다. 내과나 외과 외래로 내원한 'Small Signet/poorly-differentiated EGC'에 대해서는 아래와 같은 절차를 밟고자 합니다.
1) ESD 또는 수술 전 시행한 EGD에서 크기가 1 cm 이하로 판단되는 경우 육안적으로 보이는 병변 경계의 5 mm 밖에서 four-quadrant biopsy 시행 --> Bx (+)면 수술, Bx (-)면 ESD
2) ESD 시행했을 경우는 ESD specimen에서 LV invasion을 보기 위한 immunohistochemical stain (D2-40 등)을 반드시 시행
![]() 2. [2016년 6월 24일 IDEN lecture] ESD for EGC with undifferentiated-type histology (이준행)
2. [2016년 6월 24일 IDEN lecture] ESD for EGC with undifferentiated-type histology (이준행)
I’d like to start with a few cases. Fifty five years old gentlemen was transferred for endoscopic treatment of EGC. The histology was moderately differentiated adenocarcinoma. ESD was done, but the pathology was mostly signet ring cell carcinoma. It was a 1.8 cm sized mucosal cancer with no lymphovascular invasion. Would you recommend surgery? The procedure was done in 2007 but there was no recurrence until now without surgery.

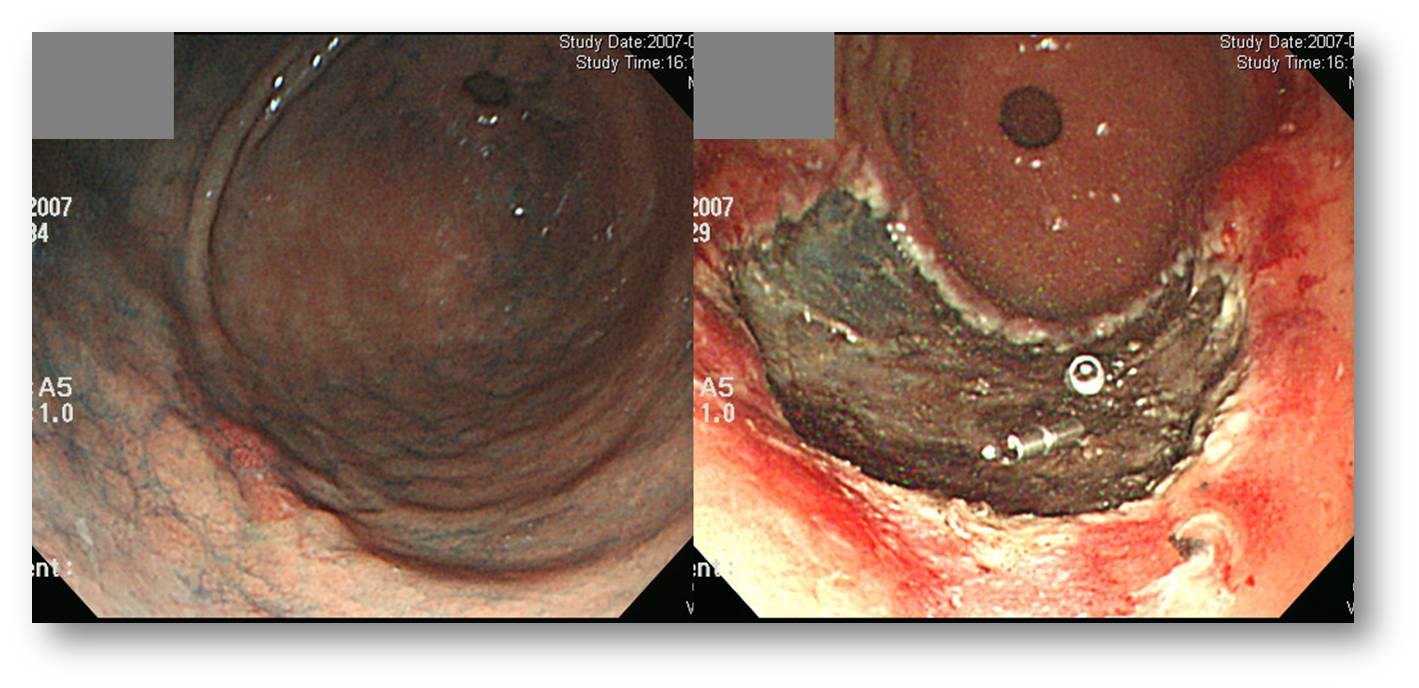
Second case. A small poorly differentiated adenocarcinoma was found during the screening endoscopy of 60 years old female. Would you perform ESD or not? I will show you one more picture, a indigocarmine chromoendoscopy. /// Would you change your opinion? Because it is a depressed lesion, larger than 1 cm, and poorly differentiated histology, I recommended surgery.
It was a mucosal cancer. However, to my surprise, there were three metastatic lymph nodes.
Before talking about the undifferentiated type EGC, I’d like to briefly review the differentiated type EGCs. Outcome of endoscopic treatment of EGC with differentiated histology is well established. We have ITT analysis such as comparison with surgery using propensitiy score matching. We also have PP analysis such as long-term follow-up data after curative resection or non-curative resection.
At my institution, we performed a propensity score-matching analysis between the two groups, endoscopic resection or surgery for differentiated type EGCs.
In the propensity score matched cases, about 60 percent were absolute indication cases. Others are expanded or beyond.
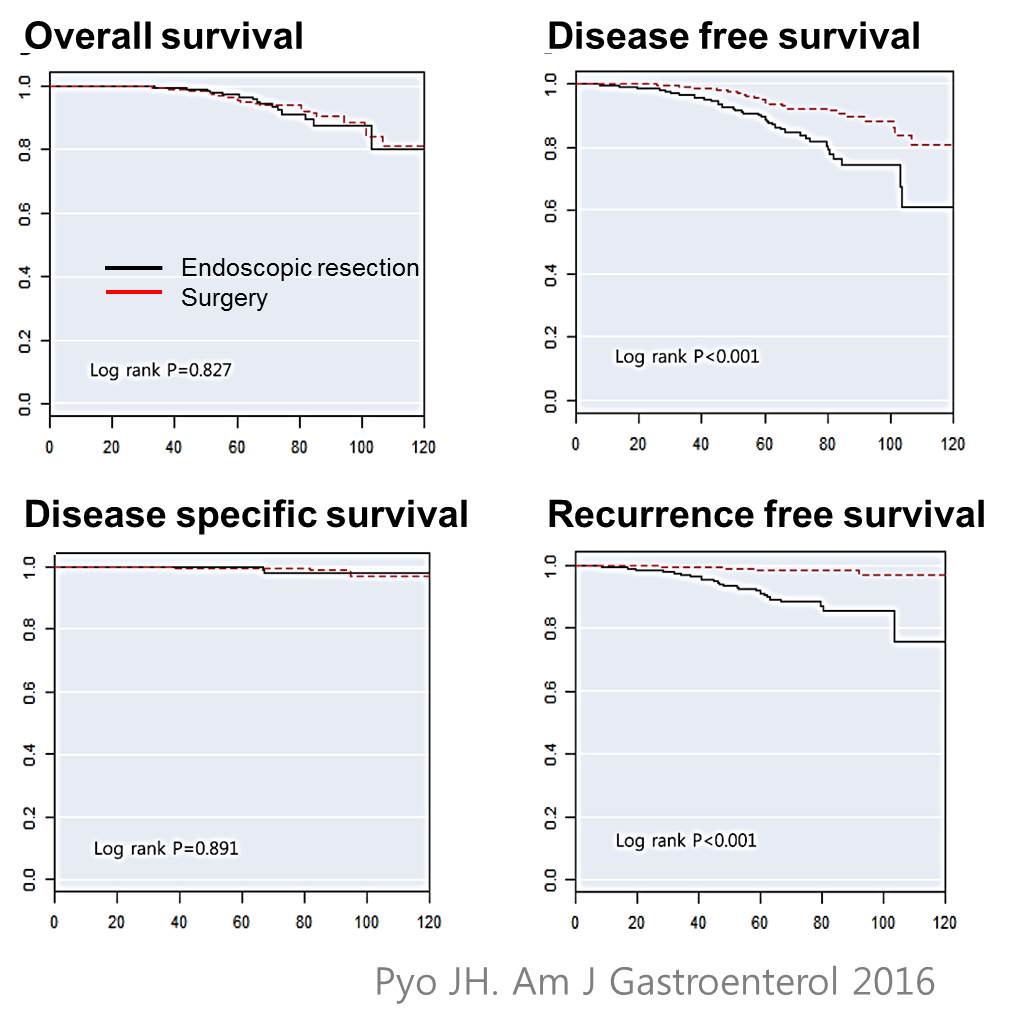
The rate of R0 resection was 82% in the endoscopic resection group The overall survival was almost the same in the two groups. Because of the metachronous recurrences, disease free survival and recurrence free survival is better in the surgery group. However, there was no difference in the disease specific survival.
Next evidence is the PP analysis. It’s a single-arm long-term follow-up data for curatively resected differentiated-type EGCs.
Excluding metachronous recurrences, we experienced only one case of local recurrence, and 2 cases of extragastric recurrences.
There are the pictures of the two extragastric recurrences. The top case belonged to the absolute indication group, and the lower case belonged to the expanded indication group.
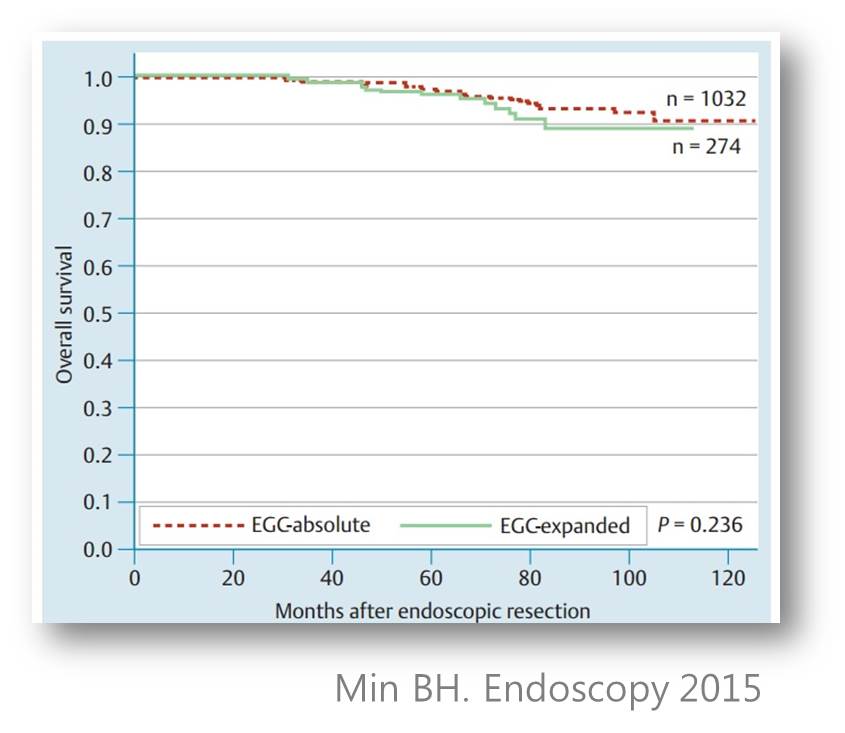
This is the overall survival. There was no statistical difference between absolute indication and expanded indication.
This is another PP analysis of non-curatively resected differentiated type EGCs. In cases with risk of lymph node metastasis, 70% were operated, and 30% were observed without surgery.
In the surgery group, 11 have lymph node metastasis, which means 5.7%. Patients with lymph node metastasis were older. To our surprise, the rate of lymph node metastasis was not different by the tumor size, depth of invasion, histological differentiation, and lymphovascular invasion in the endoscopically resected specimen. So, basically we found no predictor of lymph node metastasis in this analysis.
Rate of progression into the advanced cancers were different between 2 groups. Five advanced cancers were found in the observation group, and only one metastatic disease was found in the surgery group.
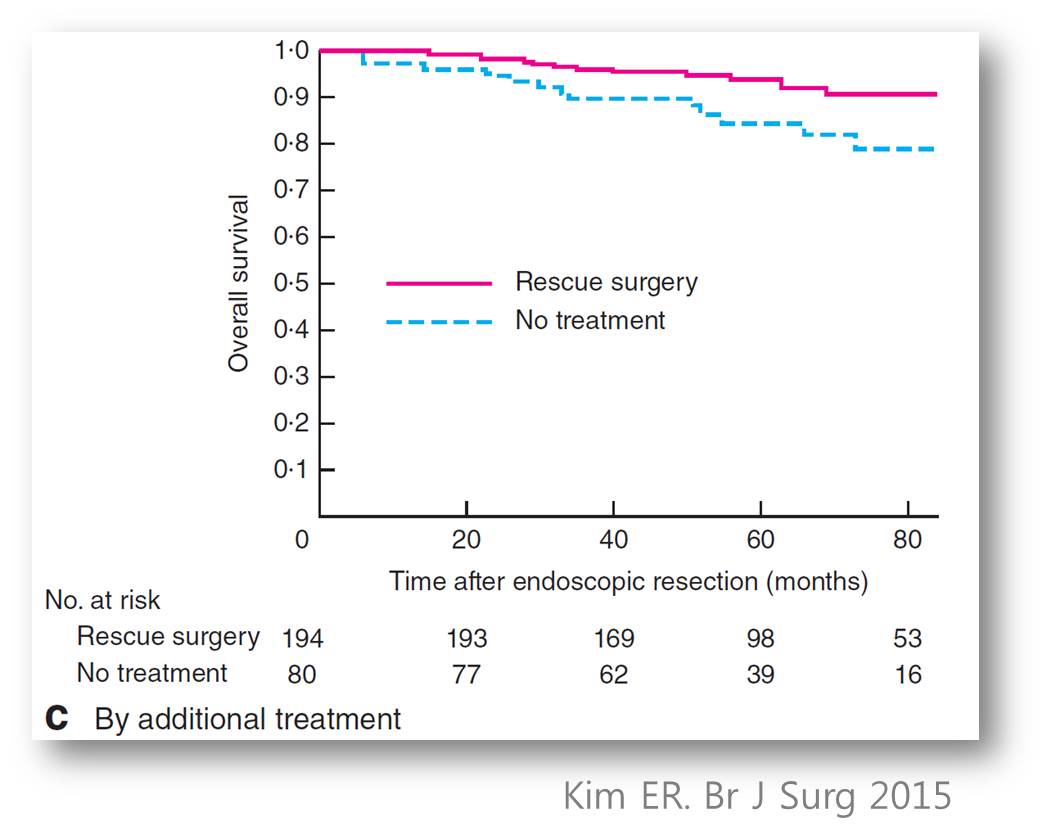
In terms of the overall survival, additional surgery was related with better outcome.
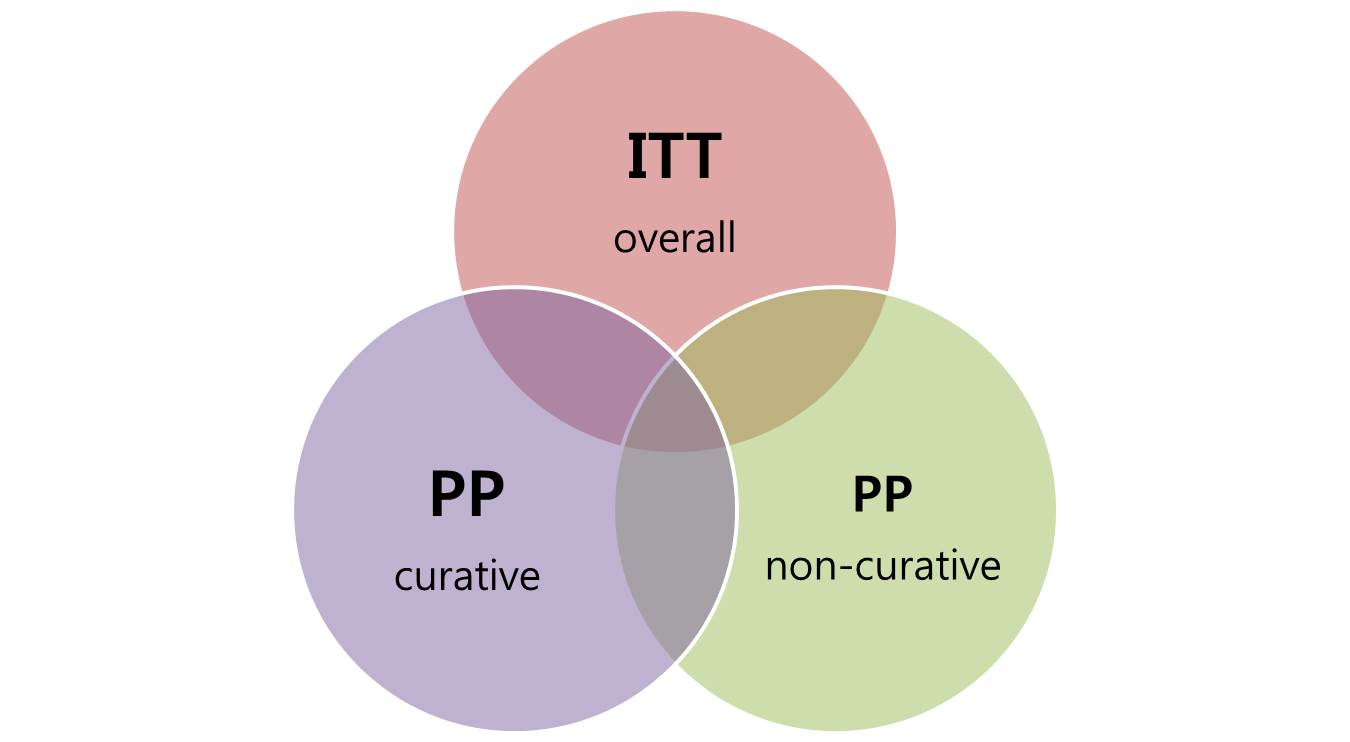
Based on the discussions until now, I can say that the outcome of ESD for differentiated-type EGC is well established. ITT analysis was done as a comparison study with surgery. PP analysis was done as long-term follow-up studies for curative resection and noncurative resection cases.
From now on, I’d like to talk about my main subject. ESD for undifferentiated-type early gastric cancers.
There are many unsolved questions regarding this topic. The first question is “are UD-type EGCs included among the expanded indications?”
This is a famous Gotoda table. In the original JCO article, UD-type cancers are not considered as expanded indications. But these days, most researchers include UD- type cancers among expanded indications.
Small UD-type mucosal cancers are included among the expanded indications /// in the Korean guideline, /// in the Japanese guideline, and /// in the European guideline. But, please be careful when reading the literature, because the term ‘expanded indication’ is differently used in the guidelines and in the literatures.
Many literatures about expanded indications do not include UD-type EGCs. Examples are /// studies from Tokyo University, /// Samsung Medical Center, /// Asan Medical Center, and /// Japanese National Cancer Center.
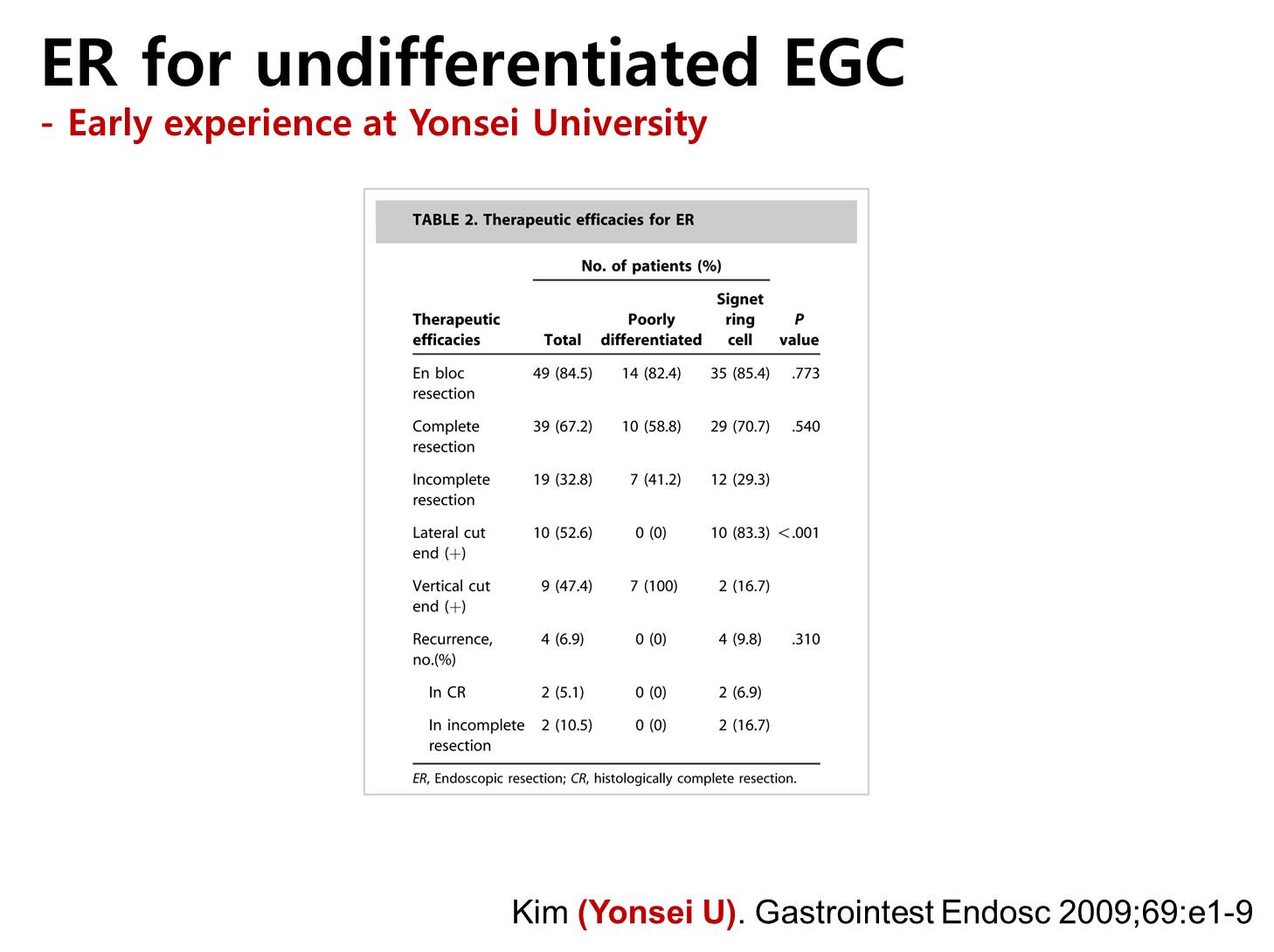
Instead, outcome for UD-type EGC is usually reported as a separate entity. This is a good example from Yonsei University Hospital. The complete resection rate of PD- type is lower than the signet ring cell type. In PD-type cancers, vertical margin was frequently involved. In signet ring cell-type cancers, lateral margin was frequently involved.

This is a follow-up from Yonsei University. There are some fatal cases in metachronous recurrence group or non-curative resection group. However, outcome was quite good in curatively-resected UD-type cancers.
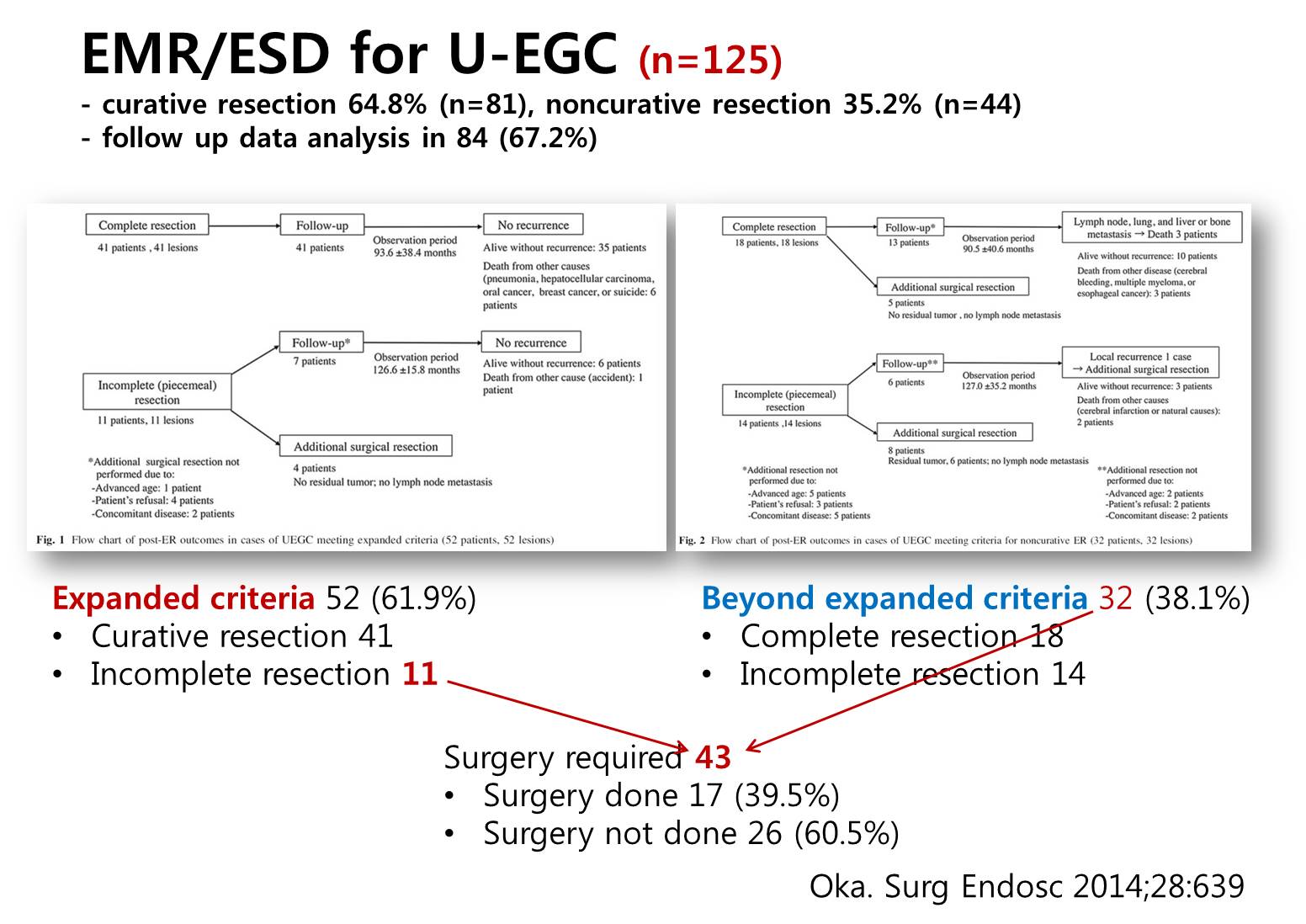
This is a report from Hiroshima University. The curative resection rate was 65%. Surgery was required in 43 cases. However, only 40% underwent surgery. For me, this number is somewhat worrisome.
This is our experience. 42 cases were PD-type and 17 cases were SRC type. Surgery was done in 44 cases and follow up was done in 15 cases.
UD type lesions are more common in younger patients, location of gastric body, bigger size, more lymphovascular invasion, more lateral margin positive, higher chance of incomplete resection.
In many cases with UD-type histology in the ESD specimen, the initial biopsy was differentiated-type histology. In this figure, only 9 out of 59 cases showed UD-type histology in the initial endoscopic biopsy. This kind of pretreatment and posttreatment histological discrepancy is a big clinical problem.
Indications are different from criteria. Indication is something that we consider before the treatment. Criteria is something we consider after the treatment. In this regard, it is likely that many UD-type cancers were initially considered as differentiated type cancers in many literatures. For further discussions, we need to focus on cases with UD-type histology in the forceps biopsy.
For this purpose, we recently performed a clinical simulation using cases with UD- type histology in the forceps biopsy.
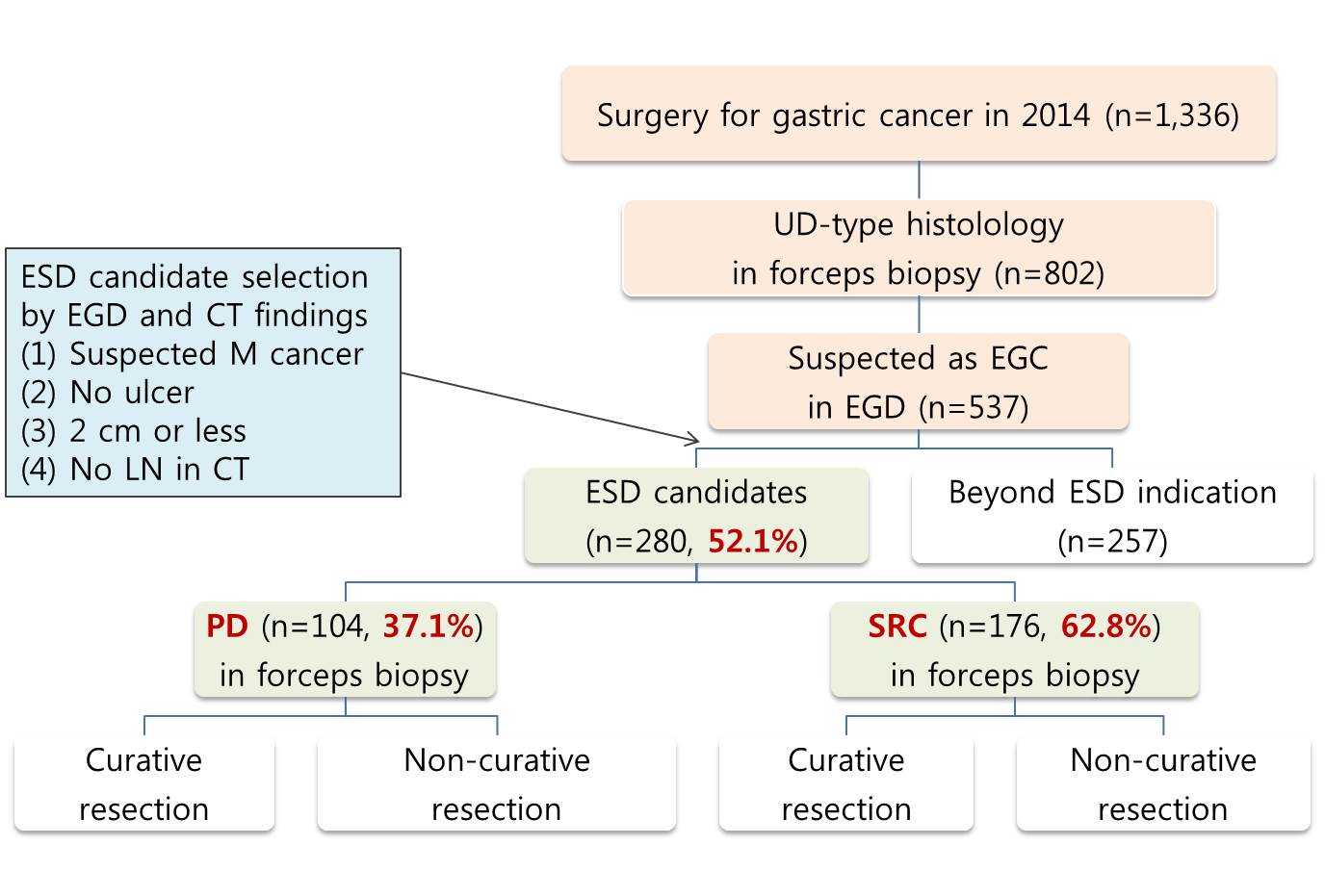
Among 537 endoscopically suspected EGCs with UD-type histology in forceps biopsy, 52 percent were selected as ESD candidates. Among them, 37 percent were PD-type and 63 percent were signet ring cell type. Based on the pathology of the surgically resected specimen, outcomes of ESD simulation were evaluated as either curative resection or non-curative resection.
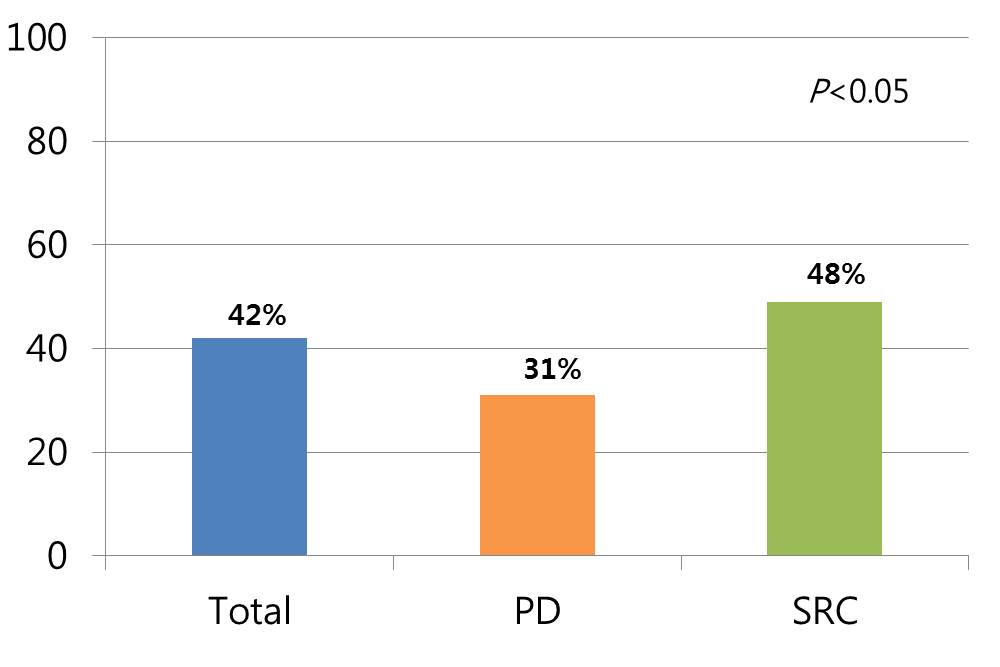
The overall rate of curative resection for expanded indication undifferentiated type EGCs was only 42%. Especially, the curative resection rate in PD type EGCs was less than one third.
This graph shows the reasons of non-curative resection in out ESD simulation. The most common reason was the size larger than 2 cm, followed by SM invasion and LV invasion.
There were three cases with lymph node metastasis in the curative resection group. Two were PD-type and one was SRC-type in the forceps biopsy. In the final surgical pathology, they was PD type mucosal cancers with SRC components larger than 1.0 cm.
Because the size was the most common reason of non-curative resection, we modified the expanded indication criteria into 1.5 cm, 1 cm and 0.6 cm. When a size criterion of 1 cm was applied, the number of ESD candidates was decreased by 51.4% and the curative resection rate was increased into 54%. However, this increase in the curative resection rate was mostly seen in the SRC type EGCS. The curative resection rate in PD type was almost the same in the smaller lesions. SRC- type less than 1 cm in diameter is the best candidate for ESD.
In this review article, proposed indications by different groups were summarized. The size limitations were usually 20 mm. However, some authors proposed 15 mm or even 10 mm.
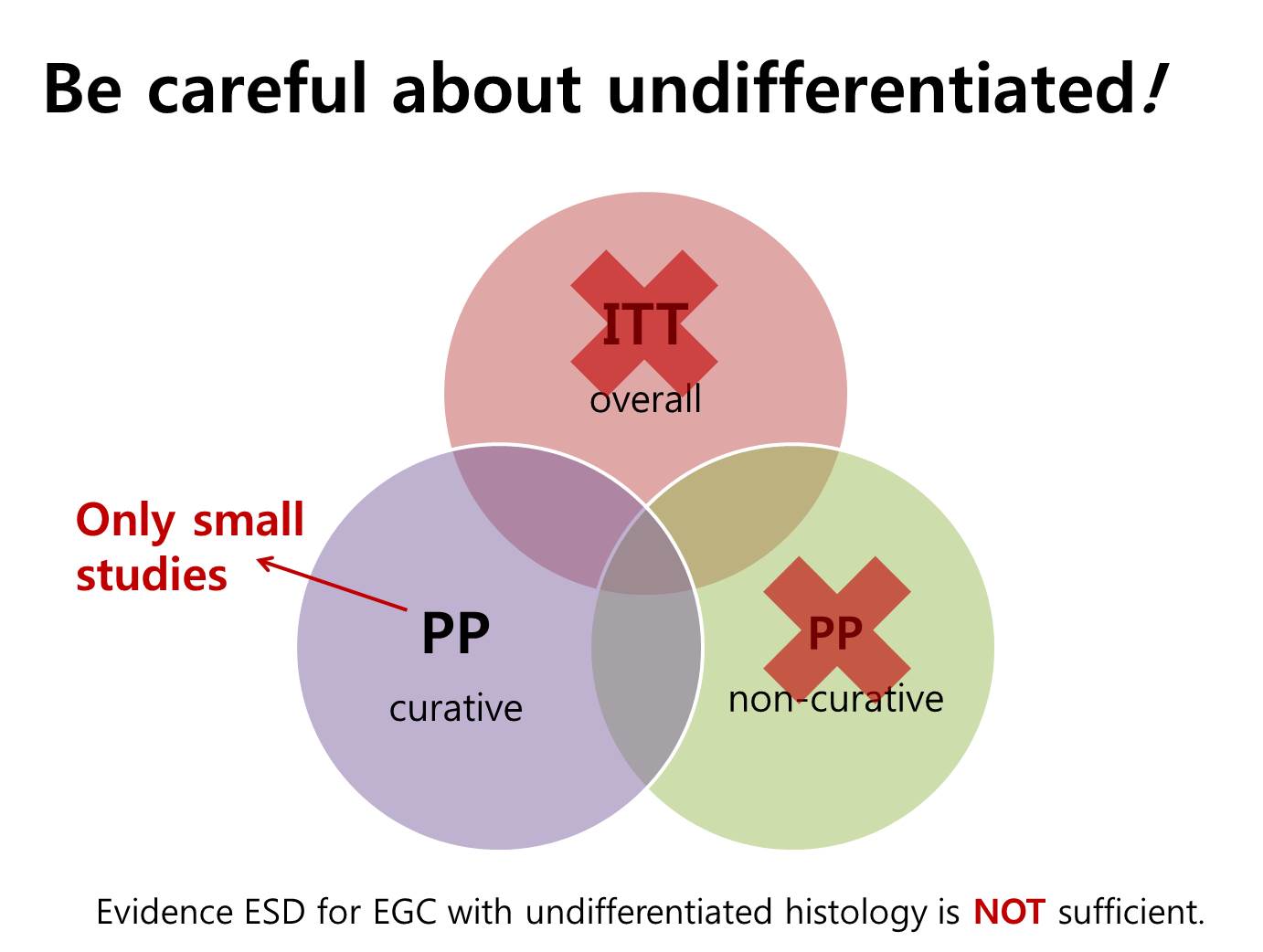
This is a summary. For UD-type cancers, we have no ITT analysis. There are insufficient data from highly selected small retrospective studies. We need to be more conservative with this topic.
Ladies and gentlemen. I’d like to conclude my presentation by saying that evidence supporting ESD for UD-type EGC is not enough. Data from surgical pathology is inconsistent. Long-term outcome data is not enough. Most importantly, selection bias makes the interpretation difficult. I propose to start with safer indications such as tumor size < 1 cm with histology of SRC to achieve better outcomes.
![]() [References]
[References]
1) EndoTODAY Undifferentiated라는 용어에 대하여 (미분화)
2) EndoTODAY Undifferentiated-type 조기위암의 림프절 전이 위험
3) EndoTODAY 확대적응증에 undifferentited-type이 포함되는가?
4) EndoTODAY 삼성서울병원 위 ESD 논문 모음
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.