 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [일원내시경교실 목요점심집담회 2016-4-28]
[일원내시경교실 목요점심집담회 2016-4-28]
![]() 1. EGC (signet ring cell carcinoma, 1 cm)
1. EGC (signet ring cell carcinoma, 1 cm)

수술을 하였고 1 cm signet ring cell carcinoma였습니다. Undifferentiated type histology를 가진 조기위암을 내시경으로 치료해도 좋을지 논란이 계속되고 있습니다. 아직까지는 수술이 표준입니다. 그러나 작은 undifferentiated type EGC, 특히 1 cm 미만, 혹은 1.5 cm 미만 signet ring cell carcinoma는 내시경으로 치료해보다는 의견이 있습니다.
저는 2016년 위암학회에서 관련 자료를 발표한 바 있습니다 (KINGCA 2016 이준행 구연 발표). 실제 ESD 성적이 아니라 수술받은 환자의 데이타를 바탕으로 한 simulation이었습니다.
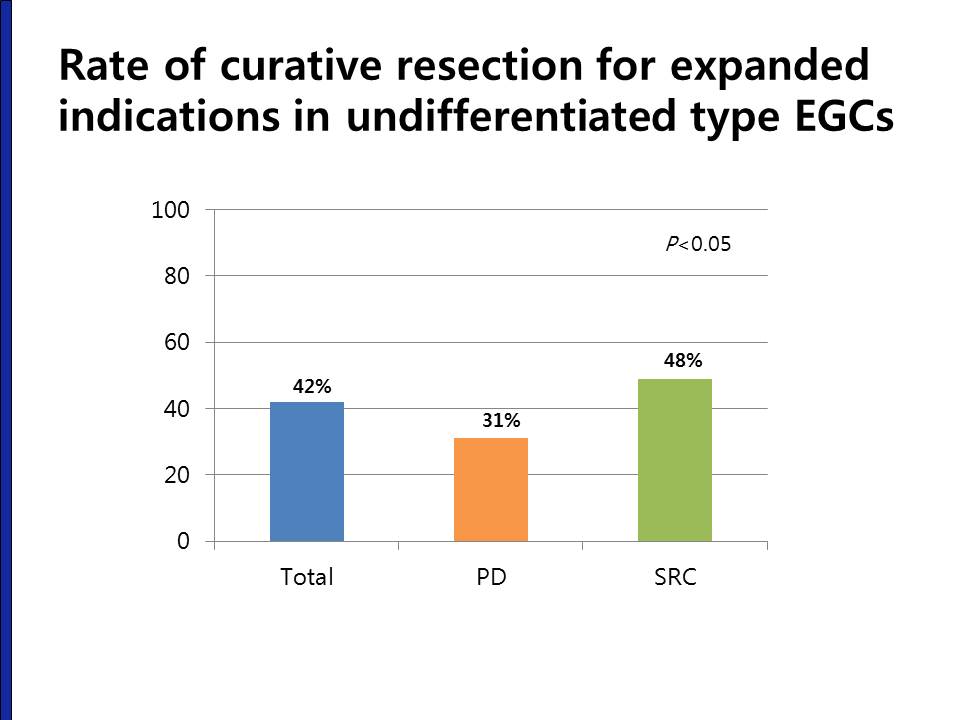
The overall rate of curative resection for expanded indication undifferentiated type EGCs was only 42%. Especially, the curative resection rate in PD type EGCs was less than one third.
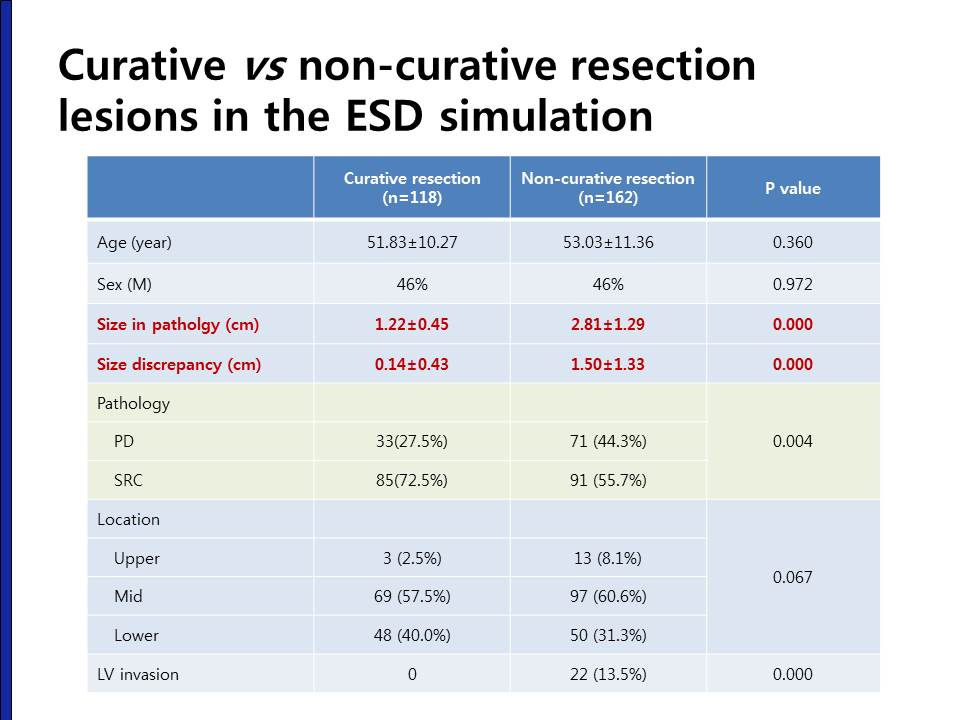
When we compare the characteristics between the curative resection lesions and non-curative resection lesions, there were no differences in terms of age, sex, location and gross type. However, the size in the curative resection group was smaller than the non-curative resection group. The size discrepancy between endoscopy size and pathology size was only 0.14 cm in curative resection group, but the size discrepancy was 1.5 cm in the non-curative resection group. This size discrepancy was one of the major reasons of non-curative resection.
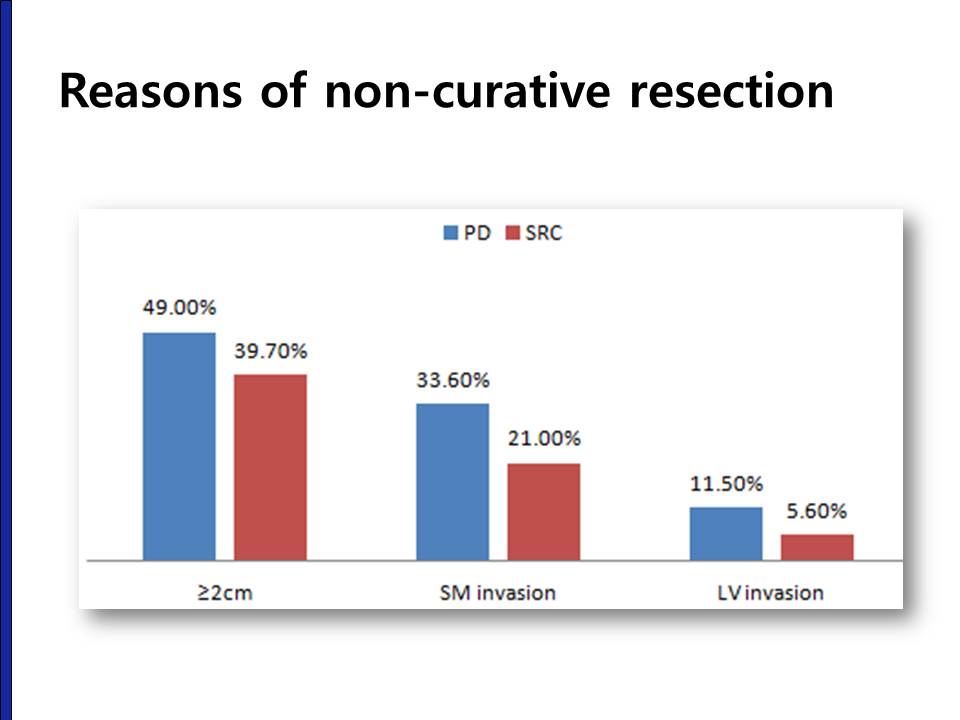
This graph shows the reasons of non-curative resection in out ESD simulation. The most common reason was the size larger than 2 cm, followed by SM invasion and LV invasion.

There were three cases with lymph node metastasis in the curative resection group. Two were PD-type and one was SRC-type in the forceps biopsy. In the final surgical pathology, they was PD type mucosal cancers with SRC components larger than 1.0 cm.

Because the size was the most common reason of non-curative resection, we modified the expanded indication criteria into 1.5 cm, 1 cm and 0.6 cm. When a size criterion of 1 cm was applied, the number of ESD candidates were decreased by 51.4% and the curative resection rate was increased into 54%. However, this increase in the curative resection rate was mostly seen in the SRC type EGCS. The curative resection rate in PD type was almost the same in the smaller lesions.
Undifferentiated type EGC의 내시경치료에 대한 2016년 5월 제 입장은 다음과 같습니다.
(1) Poorly differentiated adenocarcinoma와 signet ring cell carcinoma는 상당히 다르다.
(2) 1 cm 이하 flat한 signet ring cell carcinoma에서 시술을 고려할 수 있다.
(3) Undifferentiated type EGC에 대한 내시경치료는 아직 표준치료라고 부를 수 없다. 환자에게 먼저 내시경치료를 권할 단계는 아니다. 만약 환자가 내시경 치료를 요청하는 경우에는 아직 investigational approach라는 점을 환자에게 명백히 설명한 후 치료방침을 결정한다.
![]() 2. 소화성 궤양
2. 소화성 궤양

소화성궤양이었습니다. 제균치료를 하였습니다. 그런데 환자가 추적검사를 받으러 오시지 않았습니다. 제균이 잘 되었는지 확인되지 않은 상태였습니다. 그런데 어느 날 환자가 급성 복통으로 응급실을 방문하였습니다. 소화성 궤양 천공이었고 수술을 받았습니다.

외래에서 추적검사를 권한 환자 중 일부는 병원을 찾지 않습니다. Follow up loss된 환자 모두에게 연락을 취하여 재검을 권하는 것은 쉬운 일이 아닙니다. 옳은 일인지도 모르겠습니다. '추천한 날에 환자가 오시지 않으면 전화로 연락하겠다'고 동의를 받은 것도 아니기 때문입니다.
환자에게 충분히 설명할 시간을 마련하지 않은 대한민국 의료는 무척 후진 시스템입니다. 싸고 후집니다.
![]() 3. Total gastrectomy 후 anastomosis site 직하방 재발
3. Total gastrectomy 후 anastomosis site 직하방 재발

위암 수술 10개월 후 dysphagia로 내원하신 분에서 발견된 anastomosis site 직하방 재발입니다. 이 환자는 anastomosis site 하방이므로 benign stricture는 아니라는 것을 쉽게 알 수 있습니다. 그러나 경우에 따라서는 anastomosis site recur와 국소재발의 구분은 쉽지 않을 수 있습니다. 보통 7-8개월 이전에 발생하면 benign stricture가 많고 그 이후는 암 재발이 많습니다. 예전 자료를 옮깁니다.
위암 수술 후 문합부 협착이 발생할 수 있습니다. 특히 total gastrectomy 후 식도와 소장의 연결부가 membraneous하게 좁아지는 경우가 많습니다. 최근에는 많이 줄었지만 2005년에 발표된 삼성서울병원의 자료(Lee SY, Lee JH et al. EJSO 2005;31:265-269 )를 보면 total gastrectomy후 8-9% 전후에서 stricture가 발생하였습니다.
수술한 환자에게 미리 obstruction 증상을 설명해 주는 것은 매우 중요합니다. 간혹 obstruction 증상을 수술 후 당연히 발생할 수 있는 변화로 생각하여 몇 달이나 참고 지내는 환자들을 만날 수 있습니다.
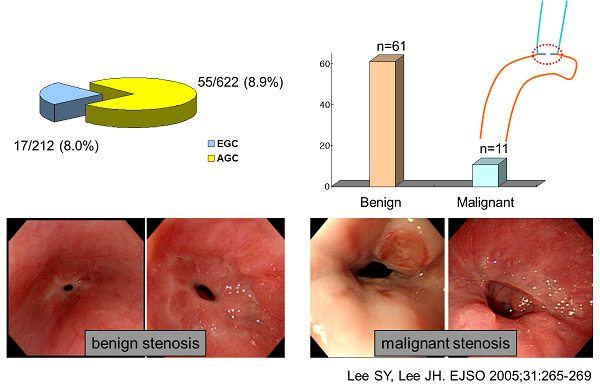
Anastomosis site의 benign postoperative stricture가 흔하지만 드물게 local recurrence도 가능합니다. Benign stricture는 수술 직후부터 수개월 이내에 호발하고 1년 이후에 발생되는 경우는 드뭅니다. 반면 위암의 local recurrence에 의한 stricture는 위암 수술 반년 경부터 2-3년 사이에 발견되는 경향이 있습니다. 일찍 발견되면 benign, 늦게 발견되면 malignancy라는 경향입니다.

문합부 주위의 재발은 문합부 소만측에 많으며, 문합부 주위 점막의 결절상 융기나 점막 비후로 나타날 수 있습니다. 수술 후에는 문합 부위의 부종과 발적, 잔존하는 봉합사 주변으로 염증 및 부분적인 궤양 등은 잔위암 또는 암의 재발과 혼돈될 수 있습니다. 자세히 관찰되고 조금이라도 이상하면 조직검사를 하는 수 밖에 없습니다. 아래는 수년 전 삼성서울병원의 논문(Lee SY, Lee JH et al. EJSO 2005;31:265-269) 에 실렸던 재발예들입니다.
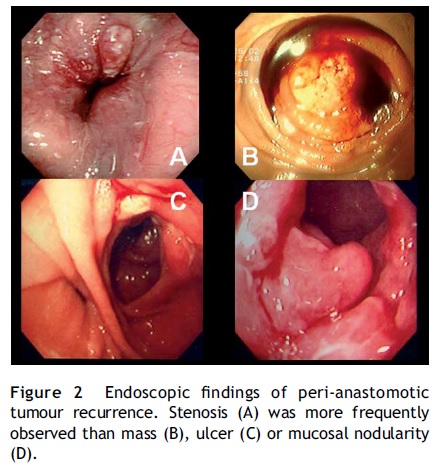
Benign post-op stricture는 수술 후 4-8개월에 발생합니다. 1년 이후에 발견된 협착은 대부분 국소재발입니다. 따라서 total gastrectomy후 anastomosis site stenosis로 내원한 환자에서 가장 먼저 확인할 것은 수술 시점입니다. 수술한지 1년 이상 경과하였으면 대부분 local recur입니다. 게다가 수술 당시 병기가 높았다면 거의 틀림없습니다. 그러나 역은 성립하지 않습니다. 1년 미만이라고 모두 benign post-op stenosis인 것은 아닙니다. 조금이라고 의심스러우면 바로 dilatation을 할 것이 아니고 조직검사를 해야 합니다.
* 참고: EndoTODAY 위암 수술 후 소견
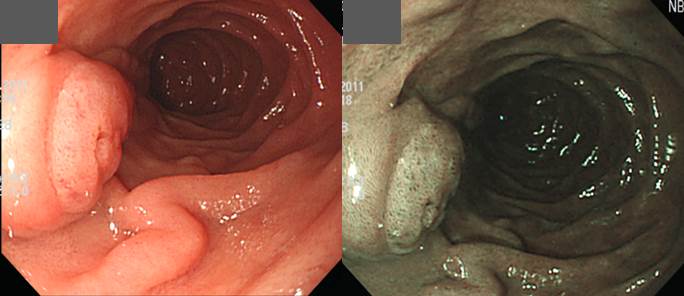
![]() 4. 상부내시경에서 발견된 ampulla of Vater adenoma
4. 상부내시경에서 발견된 ampulla of Vater adenoma
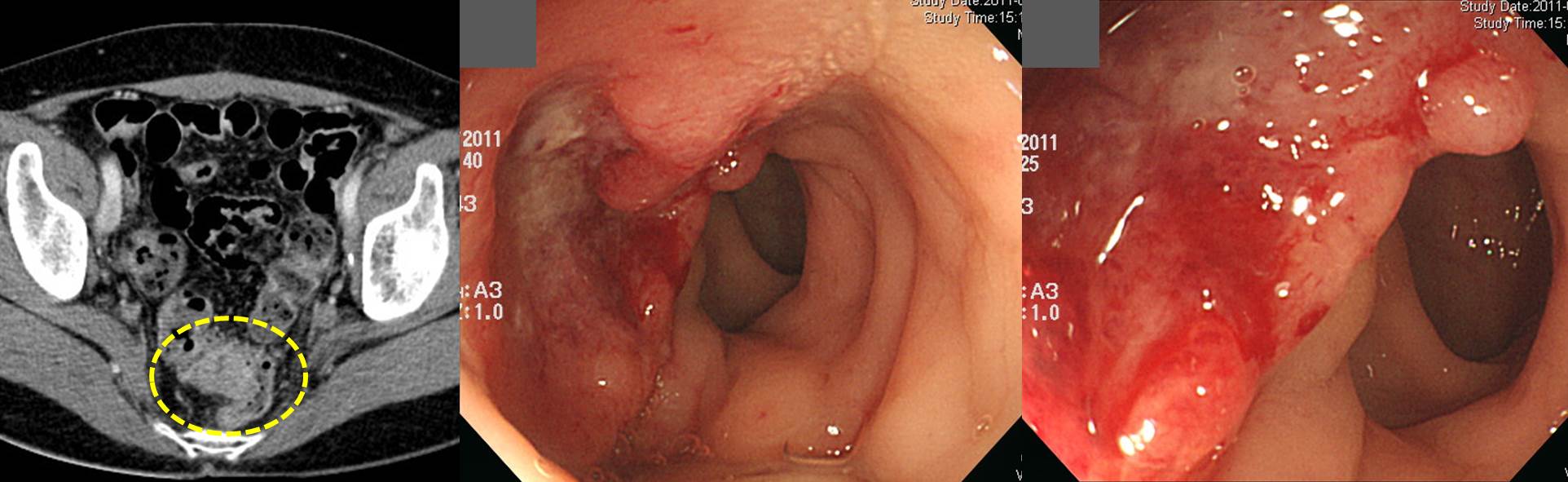
![]() 5. Ovary cancer recur at colon
5. Ovary cancer recur at colon
Ovary cancer 수술 후 CT에서 rectosigmoid junction 부위가 두꺼워 시행한 대장내시경입니다. 조직검사는 metastatic serous carcinoma가 나왔습니다.
![]() [References]
[References]
1) SMC Endoscopy Unit 삼성서울병원 내시경실
2) SMC Monday GI conference 삼성서울병원 일원내시경교실 월요점심소화기집담회
3) SMC Thursday endoscopy conference 삼성서울병원 일원내시경교실 목요점심내시경집담회
© EndoTODAY Endoscopy Learninng Center. Jun Haeng Lee.