 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Thursday Endoscopy Conference 20160707]
[Thursday Endoscopy Conference 20160707]
![]() 1. Local recurrence 2 years after total gastrectomy
1. Local recurrence 2 years after total gastrectomy
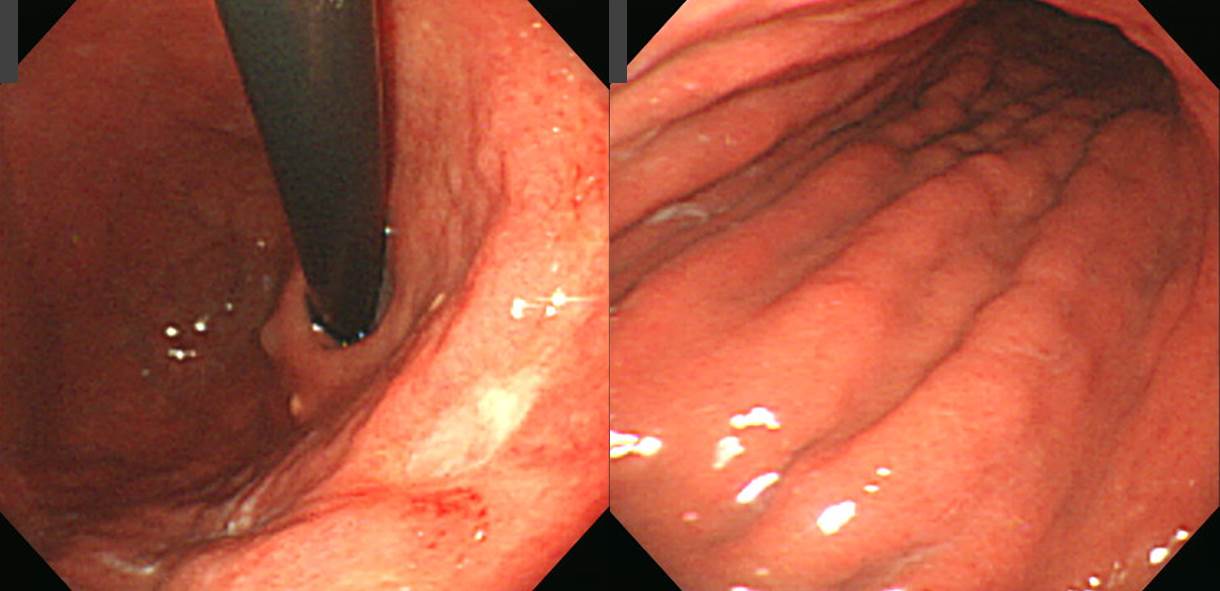
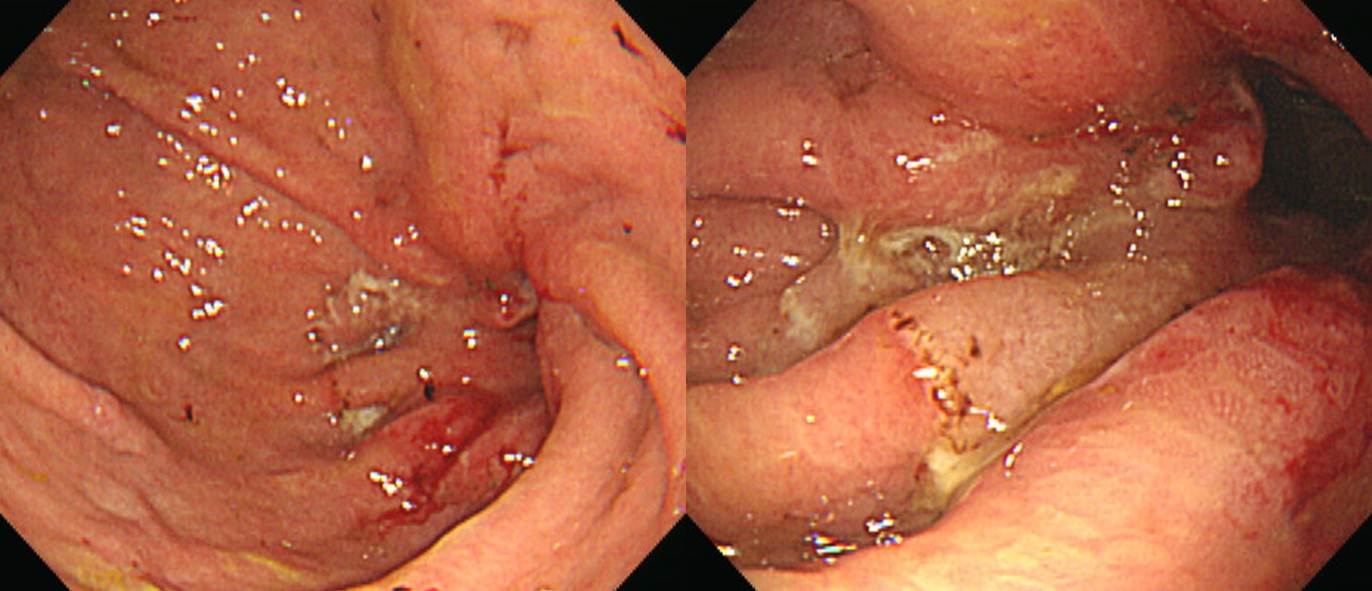
건진 발견 진행성 위암이었습니다. 장경 10.8cm였고 serosa까지 침윤된 다발성 림프절 전이(11 out of 69)를 동반한 poorly differentiated type 보만 4형 진행성 위암이었습니다.
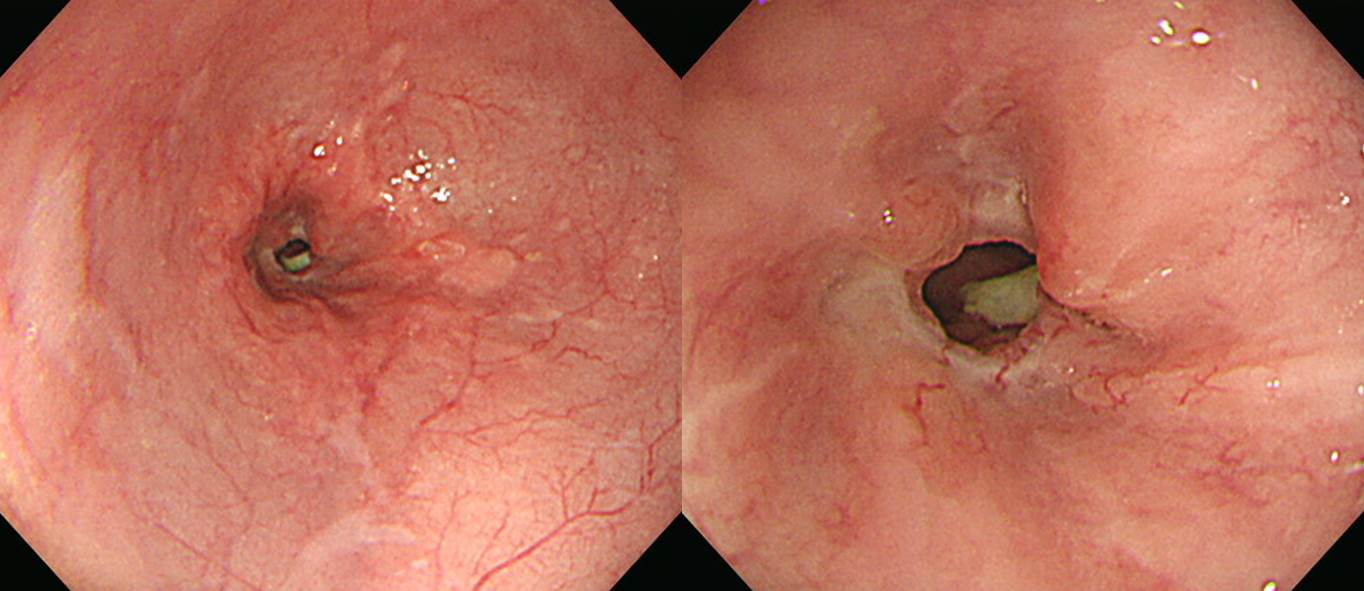
Total gastrectomy 후 약간의 dysphagia가 지속되었던 분인데 최근 좀 더 증상이 발생하였습니다. 아주 근경을 보면 recur를 판단하기 어려운 모양이지만 조금 물러서 멀리서 바라보면 문합부 직상방이 약간 좁아져있고 infiltration 소견이 있었습니다. 조직검사에서는 pooly differentiated adenocarcinoma로 나왔고 curative surgery는 불가능하였습니다.
Total gastrectomy 후 recur 양상에 대한 EndoTODAY 자료를 다시 옮깁니다.
위암 수술 후 문합부 협착이 발생할 수 있습니다. 특히 total gastrectomy 후 식도와 소장의 연결부가 membraneous하게 좁아지는 경우가 많습니다. 최근에는 많이 줄었지만 2005년에 발표된 삼성서울병원의 자료(Lee SY. EJSO 2005)를 보면 total gastrectomy후 8-9% 전후에서 stricture가 발생하였습니다.
수술한 환자에게 미리 obstruction 증상을 설명해 주는 것은 매우 중요합니다. 간혹 obstruction 증상을 수술 후 당연히 발생할 수 있는 변화로 생각하여 몇 달이나 참고 지내는 환자들을 만날 수 있습니다.
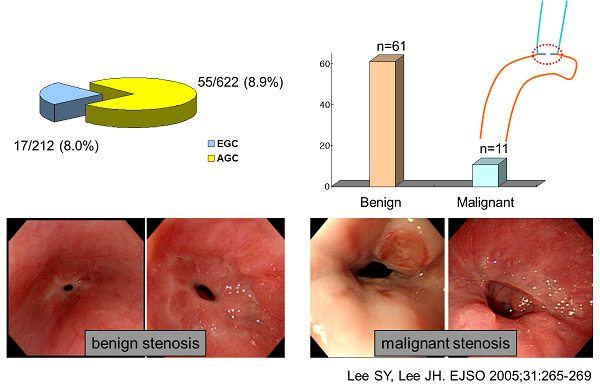
Anastomosis site의 benign postoperative stricture가 흔하지만 드물게 local recurrence도 가능합니다. Benign stricture는 수술 직후부터 수개월 이내에 호발하고 1년 이후에 발생되는 경우는 드뭅니다. 반면 위암의 local recurrence에 의한 stricture는 위암 수술 반년 경부터 2-3년 사이에 발견되는 경향이 있습니다. 일찍 발견되면 benign, 늦게 발견되면 malignancy라는 경향입니다.

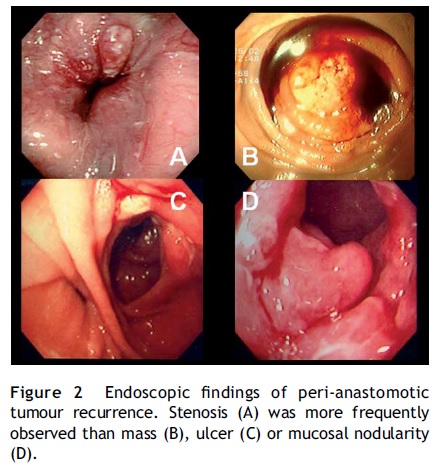
문합부 주위의 재발은 문합부 소만측에 많으며, 문합부 주위 점막의 결절상 융기나 점막 비후로 나타날 수 있습니다. 수술 후에는 문합 부위의 부종과 발적, 잔존하는 봉합사 주변으로 염증 및 부분적인 궤양 등은 잔위암 또는 암의 재발과 혼돈될 수 있습니다. 자세히 관찰되고 조금이라도 이상하면 조직검사를 하는 수 밖에 없습니다. 아래는 수년 전 삼성서울병원의 논문(Lee SY. EJSO 2005)에 실렸던 재발예들입니다.
Benign post-op stricture는 수술 후 4-8개월에 발생합니다. 1년 이후에 발견된 협착은 대부분 국소재발입니다. 따라서 total gastrectomy후 anastomosis site stenosis로 내원한 환자에서 가장 먼저 확인할 것은 수술 시점입니다. 수술한지 1년 이상 경과하였으면 대부분 local recur입니다. 게다가 수술 당시 병기가 높았다면 거의 틀림없습니다. 그러나 역은 성립하지 않습니다. 1년 미만이라고 모두 benign post-op stenosis인 것은 아닙니다. 조금이라고 의심스러우면 바로 dilatation을 할 것이 아니고 조직검사를 해야 합니다.
* 참고: EndoTODAY 위암 수술 후 소견
![]() 2. Remnant gastric cancer
2. Remnant gastric cancer
40년 전에 궤양으로 위부분절제술을 받은 분입니다.
Status post subtotal gastrectomy due to gastric ulcer perforation
Advanced gastric carcinoma
1. Location : lower third, Center at low body and greater curvature
2. Gross type : Borrmann type 3
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size : 4.5x4 cm
6. Depth of invasion : invades serosa (pT4a)
7. Resection margin: free from carcinoma, safety margin: proximal 4 cm, distal 1.5 cm
8. Lymph node metastasis : no metastasis in 20 regional lymph nodes (pN0)
9. Lymphatic invasion : present
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
13. AJCC stage by 7th edition: T4a N0
* 참고: EndoTODAY 잔위암
![]() 3. Recurred HCC with stomach invasion
3. Recurred HCC with stomach invasion

Left lateral segment의 간세포암으로 수술을 시행받은 환자의 수술 전 CT 및 MRI입니다.
Liver, left lateral segmentectomy:
Progressed hepatocellular carcinoma, S2 and S3 :
1. Gross type : Nodular type
2. Differentiation : Edmondson grade III
3. Histologic type : microtrabecular
4. Cell type : hepatic
5. Tumor size : 10.1x8x5.7 cm
6. Tumor number : one
7. Fatty change : no
8. Tumor necrosis : yes (50%)
9. Hemorrhage : no
10. Fibrous capsule : partial
11. Tumor invasion in tumor capsule : yes
12. Septum formation : yes
13. Microvessel invasion : peritumoral
14. Portal vein invasion : no
15. Bile duct invasion : no
16. Intrahepatic metastasis (satellite nodule) : no
17. Multicentric occurrence : no
18. Surgical margin invasion : no (safety margin : 0.4 cm)
19. Serosa invasion : no
20. Pathologic T stage (modified UICC, 2000): pT3
21. Pathologic T stage (AJCC, 2010) : pT2
22. Regional lymph nodes : Metastasis in 8 out of 11 lymph nodes
23. Distant metastasis : not applicable
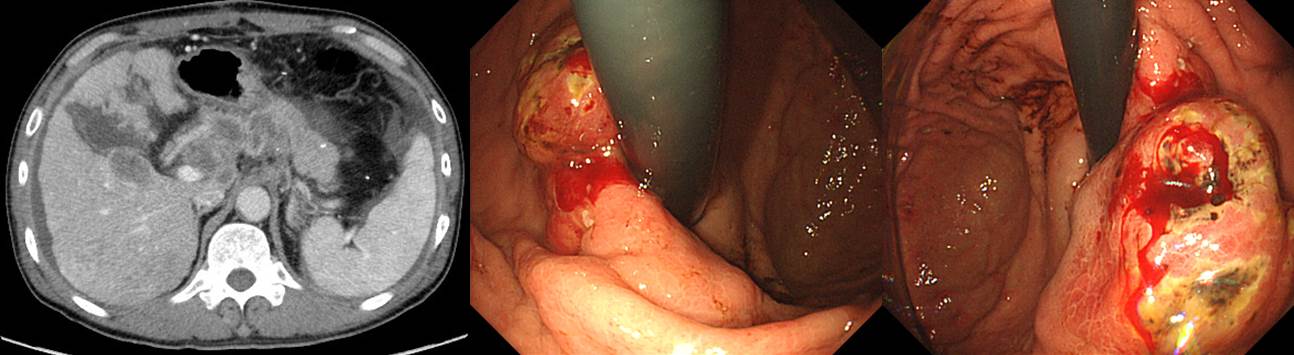
추적검사 CT에서 재발이 확인되었습니다. "Remnant liver에 multiple low-density lesion들이 새롭게 보여 recurrent tumor로 생각되며 양측 portal vein 및 main portal vein 내에 tumor thrombus가 형성되어 있음. Hepatoduodenal ligament와 pancreas 주변 그리고 aorta 주변으로 metastatic lymph node들의 size가 모두 증가되었음."
위내시경에서도 재발암의 위침윤이 의심되었고 조직검사에서 아래와 같은 소견이 나왔습니다.
Poorly differentiated carcinoma with clear cells (see note)
Note: The possibility of clear cell type adenocarcinoma or hepatoid adenocarcinoma is suspicious. Based on immunohistochemistry findings, the former is preferred.
Clear cell type이라는 보고가 낯설지만 간암의 한 subtype으로도 언급된 바 있어서 '간암 재발 위침윤'이 틀림없습니다. 한 리뷰에서는 간암 subtype으로 아래와 같이 언급되어 있습니다 (Schlageter M. WJG 2014).
* 참고: EndoTODAY 위전이
![]() [References]
[References]
1) SMC Endoscopy Unit 삼성서울병원 내시경실
2) SMC Monday GI conference 삼성서울병원 일원내시경교실 월요점심소화기집담회
3) SMC Endoscopy conference 삼성서울병원 일원내시경교실 목요점심내시경집담회
© EndoTODAY Endoscopy Learning Center. Jun Haeng Lee.