EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Remnant gastric cancer. 잔위암] - 終
[Remnant gastric cancer. 잔위암] - 終
1. 잔위암의 종류와 빈도
2. 잔위암의 내시경 진단
3. 가장 무서운 암 - Borrmann type IV cancer in the remnant stomach
6. 잔위암의 수술적 치료
7. 잔위암의 내시경 치료
8. Subtotal gastrectomy 후 추적관찰
9. FAQs
10. References
![]() 1. 잔위암의 종류와 빈도
1. 잔위암의 종류와 빈도
잔위암은 원발암의 종류와 수술 후 잔위암 발견까지의 시간 간격에 따라 아래와 같이 3 가지로 나눕니다.
문합부에 많고 다음으로 들문에 많은 듯 합니다.
잔위암의 발생 빈도는 연구에 따라 큰 차이가 있지만 5년 2.4%, 10년 2.6%, 15년 3.2%, 20년 4%라는 이탈리아 자료가 있습니다 (Am J Surg 2015). 이 수치는 우리나라의 잔위암 발생률보다 조금 낮은 것 같습니다.
![]() 2. 잔위암의 내시경 진단
2. 잔위암의 내시경 진단

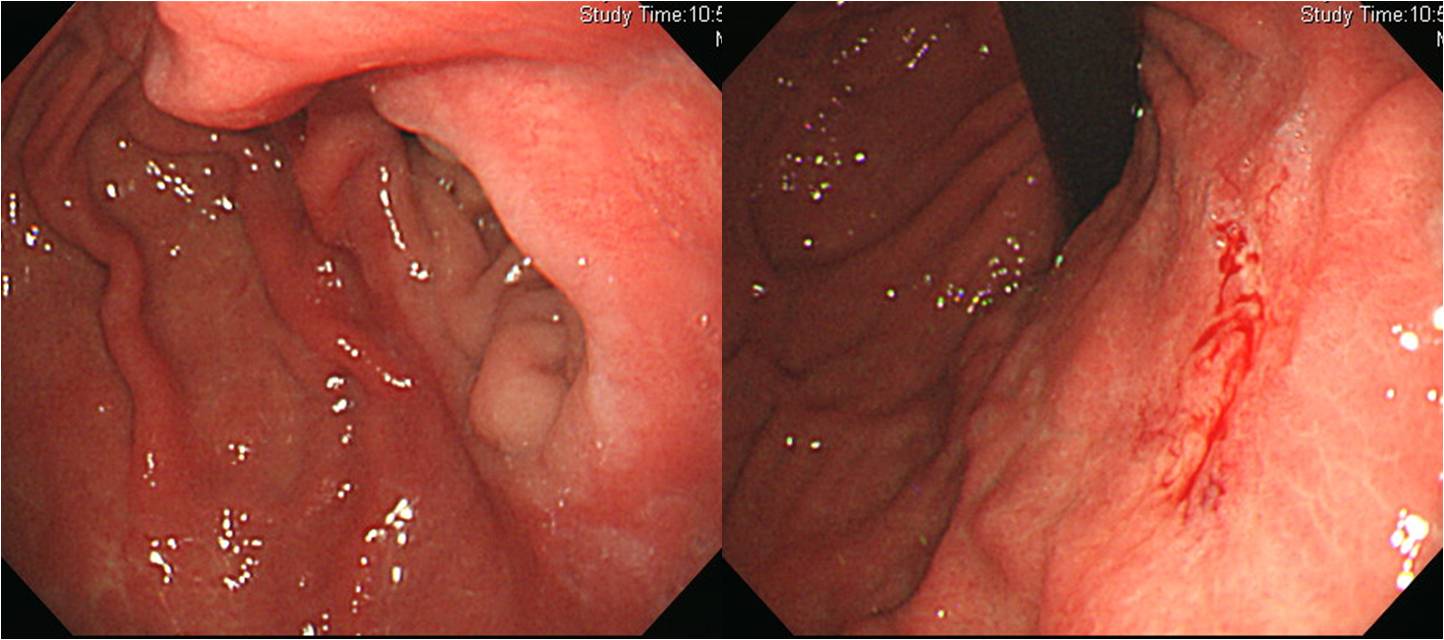
30년 전 궤양 수술. 문합부 잔위암
40년 전에 궤양으로 위부분절제술을 받은 분입니다. 다행스럽게 잔위암 수술이 가능했습니다.
Status post subtotal gastrectomy due to gastric ulcer perforation
Advanced gastric carcinoma
1. Location : lower third, Center at low body and greater curvature
2. Gross type : Borrmann type 3
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size : 4.5x4 cm
6. Depth of invasion : invades serosa (pT4a)
7. Resection margin: free from carcinoma, safety margin: proximal 4 cm, distal 1.5 cm
8. Lymph node metastasis : no metastasis in 20 regional lymph nodes (pN0)
9. Lymphatic invasion : present
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
13. AJCC stage by 7th edition: T4a N0
50년 전에 궤양으로 위부분절제술을 받은 분입니다. 잔위암이 발견되었고 아쉽게도 처음부터 간전이 상태였습니다.
Stomach, subtotal gastrectomy:
Advanced gastric carcinoma
1. Location : lower third, Center at antrum and lesser curvature
2. Gross type : Borrmann type 3
3. Histologic type : tubular adenocarcinoma, poorly differentiated
4. Histologic type by Lauren : diffuse
5. Size : 5x3 cm
6. Depth of invasion : penetrates subserosal connective tissue (pT3)
7. Resection margin: free from carcinoma, safety margin: proximal 3 cm, distal 3 cm
8. Lymph node metastasis : metastasis to 21 out of 35 regional lymph nodes (pN3b) (perinodal extension: present) (21/35 : "1", 0/5; "3", 5/9; "4", 11/13; "4sb", 0/0; "5", 0/0; "6", 1/2; "7", 0/2; "8a", 0/0; "9", 3/3; "11p", 0/0; "12a", 1/1)
9. Lymphatic invasion : present
10. Venous invasion : not identified
11. Perineural invasion : present
12. AJCC stage by 7th edition: T3 N3b수술 후 항암 방사선치료를 하였습니다. 2년 후 추적 내시경을 시행하였고 조직검사에서 moderately differentiated tubular adenocarcinoma가 나왔습니다. CT에서 locally invasive recurrent cancer였기 때문에 재수술은 불가능한 상태였습니다.
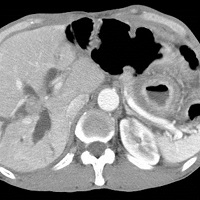
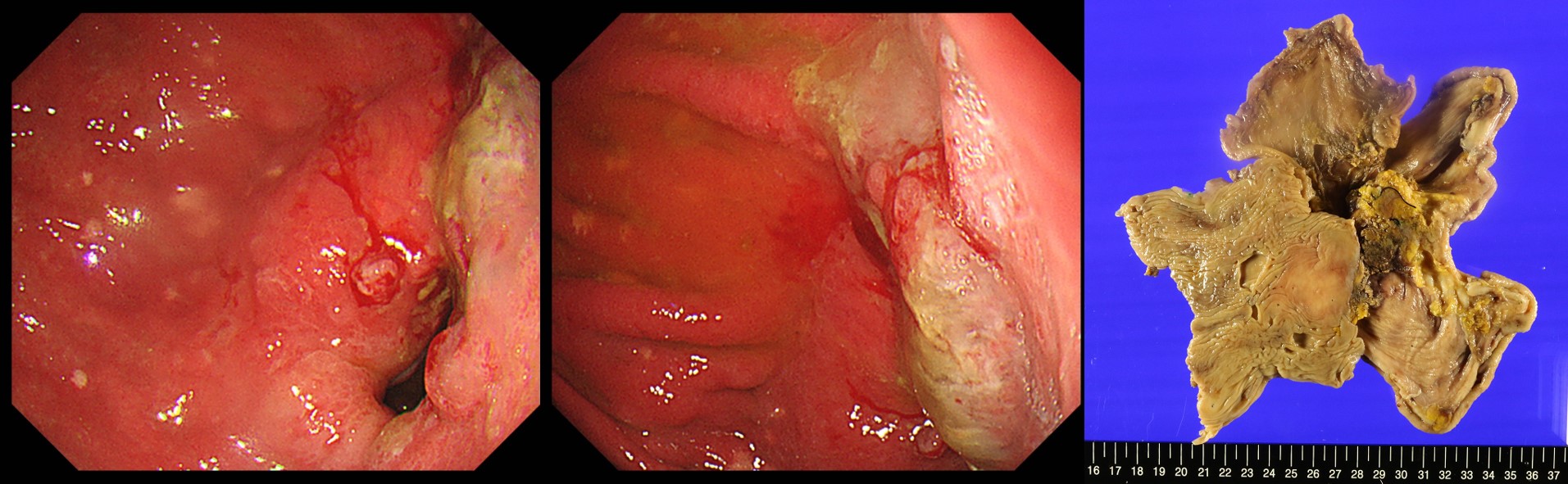
40년 전 궤양 천공으로 subtotal gastrectomy 받은 분입니다.. 양 하지 부종으로 타원 방문하여 CT 검사를 하였고 위암 소견이 보여 내시경 검사를 받았고 진단되어 의뢰되었습니다. CT 판독은 "Gastrojejunostomy site 직상방에 약 4 cm segment에 걸쳐 enhancing wall thickening이 있음." 였는데... 다시 CT 사진을 보아도 진단이 쉽지 않았을 것 같습니다. 내시경 소견에서도 진단이 쉽지 않은 모양이었습니다. 뚜렷한 궤양은 없이 anastomosis site 직상방이 조금 부어 있는 정도가 대부분의 소견이었으므로.
Status post subtotal gastrectomy due to gastric ulcer perforation
Advanced gastric carcinoma
1. Location : lower third, Center at low body and greater curvature
2. Gross type : Borrmann type 3
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size : 4.5x4 cm
6. Depth of invasion : invades serosa (pT4a)
7. Resection margin: free from carcinoma, safety margin: proximal 4 cm, distal 1.5 cm
8. Lymph node metastasis : no metastasis in 20 regional lymph nodes (pN0) (0/20: "1", 0/1; "3", 0/1; "4", 0/1; "4sb", 0/0; "8a", 0/4; "7", 0/3; "9", 0/2; "11p", 0/5; "12a", 0/3)
9. Lymphatic invasion : present
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
13. AJCC stage by 7th edition: T4a N0
Stomach, (completion) total gastrectomy:
Early gastric carcinoma
1. Location : center at anastomosis site and lesser curvature
2. Gross type : EGC type IIc
3. Histologic type : signet-ring cell carcinoma
4. Histologic type by Lauren : diffuse
5. Size : 2.6x1.8x0.2 cm
6. Depth of invasion : extension to mucosa (muscularis mucosa) (pT1a)
7. Resection margin: free from carcinoma, safety margin: proximal, 4.6 cm; distal, 4.3 cm
8. Lymph node metastasis : no metastasis in 2 regional lymph nodes (pN0) (0/2: "1", 0/2; "2", 0/0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified

Stomach, completion total gastrectomy:
Early gastric carcinoma
1. Location : Remnant stomach, Center at anastomosis site
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size : 2.7x1.8 cm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin: free from carcinoma, safety margin: proximal 1.2 cm, distal 8 cm
8. Lymph node metastasis : cannot be assessed
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
13. AJCC stage by 7th edition: pT1a Nx
Completion total gastrectomy: Advanced gastric carcinoma (arising in an villotubular adenoma)
1. Location : Center at anastomosis site body and lesser curvature
2. Gross type : Borrmann type 3
3. Histologic type : mucinous adenocarcinoma (mucinous carcinoma portion: 60 %)
4. Histologic type by Lauren : intestinal
5. Size : 4.5x4 cm
6. Depth of invasion : penetrates subserosal connective tissue (pT3)
7. Resection margin: free from carcinoma
8. Lymph node metastasis : no metastasis
9. Lymphatic invasion with D2-40 immunohistochemistry : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
13. AJCC stage by 8th edition: pT3 N0
This is a remnant gastric cancer 30 years after partial gastrectomy for peptic ulcer bleeding. Endoscopic resection was impossible due to it's location (anastomosis site).

Stomach, completion total gastrectomy: Status post subtotal gastrectomy. Early gastric carcinoma
1. Location : middle third and anastomosis site, Center at anastomosis site
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size : 1.9x0.9 cm
6. Depth of invasion : invades mucosa (muscularis mucosae) (pT1a)
7. Resection margin: free from carcinoma, safety margin: proximal 9.2 cm, distal 6.5 cm
8. Lymph node metastasis : no metastasis in 26 regional lymph nodes (pN0) (0/26 : "2", 0/4; "3", 0/10; "4", 0/0; "6", 0/0; "7", 0/1; "9", 0/3; "8a", 0/6; "11p", 0/0; "12a", 0/2; "4sb", 0/0; "1", 0/0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
13. AJCC stage by 8th edition: pT1a N0
S/P surgery for duodenal ulcer perforation (30 years ago)
Stomach, completion total gastrectomy : Advanced gastric carcinoma
1. Location : middle third Center at mid body (anastomosis site)
2. Gross type : Borrmann type 3
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size : 10x4.5 cm
6. Depth of invasion : invades adjacent structures/organs (pT4b) (invades to muscularis propria of transverse colon and liver parenchyme)
7. Resection margin: free from carcinoma. safety margin: proximal 2 cm, distal 2.5 cm
8. Lymph node metastasis : metastasis to 4 out of 30 regional lymph nodes (pN2) (perinodal extension: present) (4/30: "11p", 0/6; "12a", 0/6; "14", 0/2; "3,5", 2/2; "4,6", 0/2; "colon LN", 2/7; perigastric LN, 0/5)
9. Lymphatic invasion : present
10. Venous invasion : present(extramural)
11. Perineural invasion : present
12. AJCC stage by 8th edition: pT4b N2
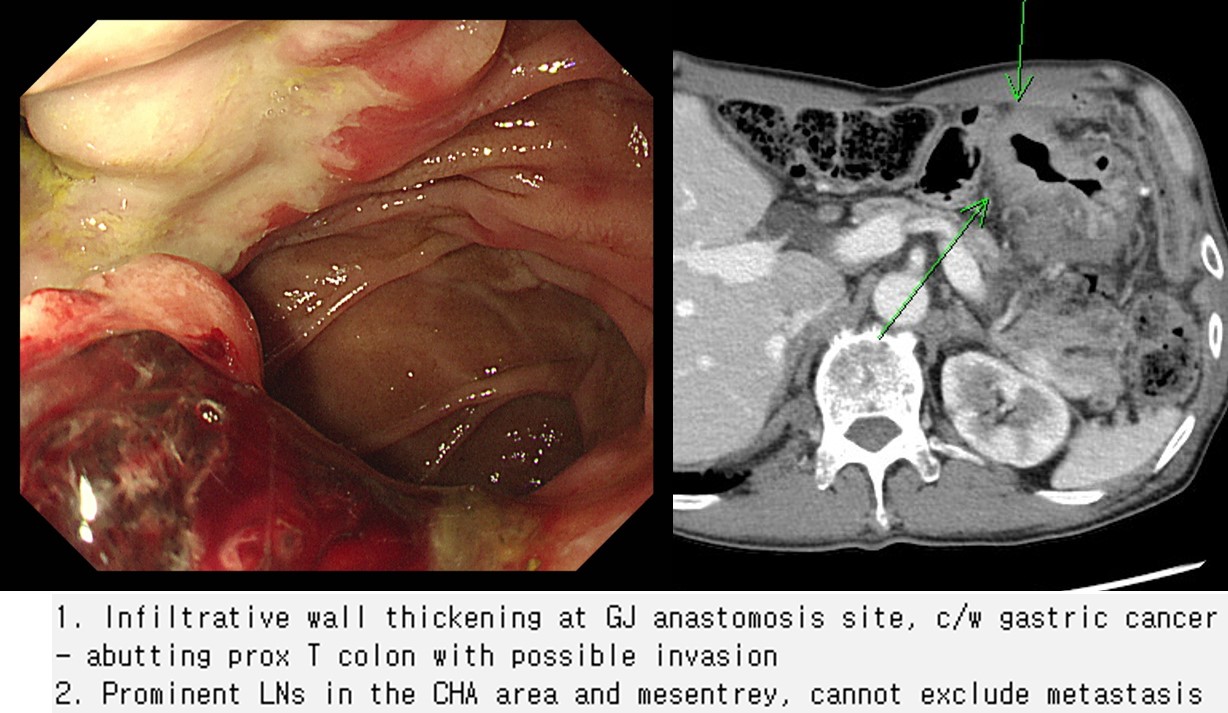
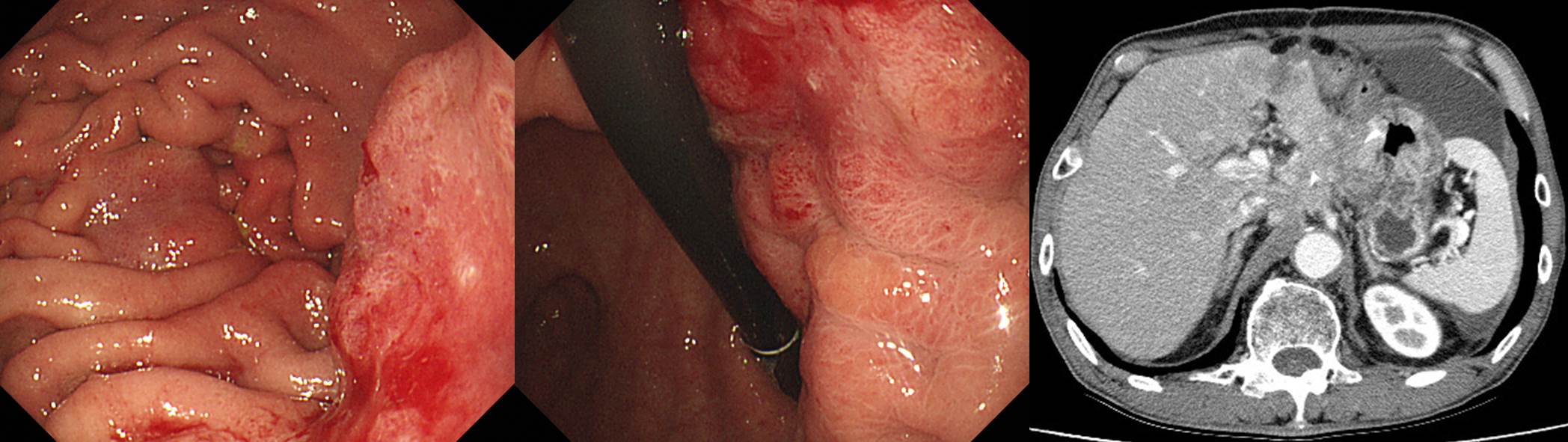
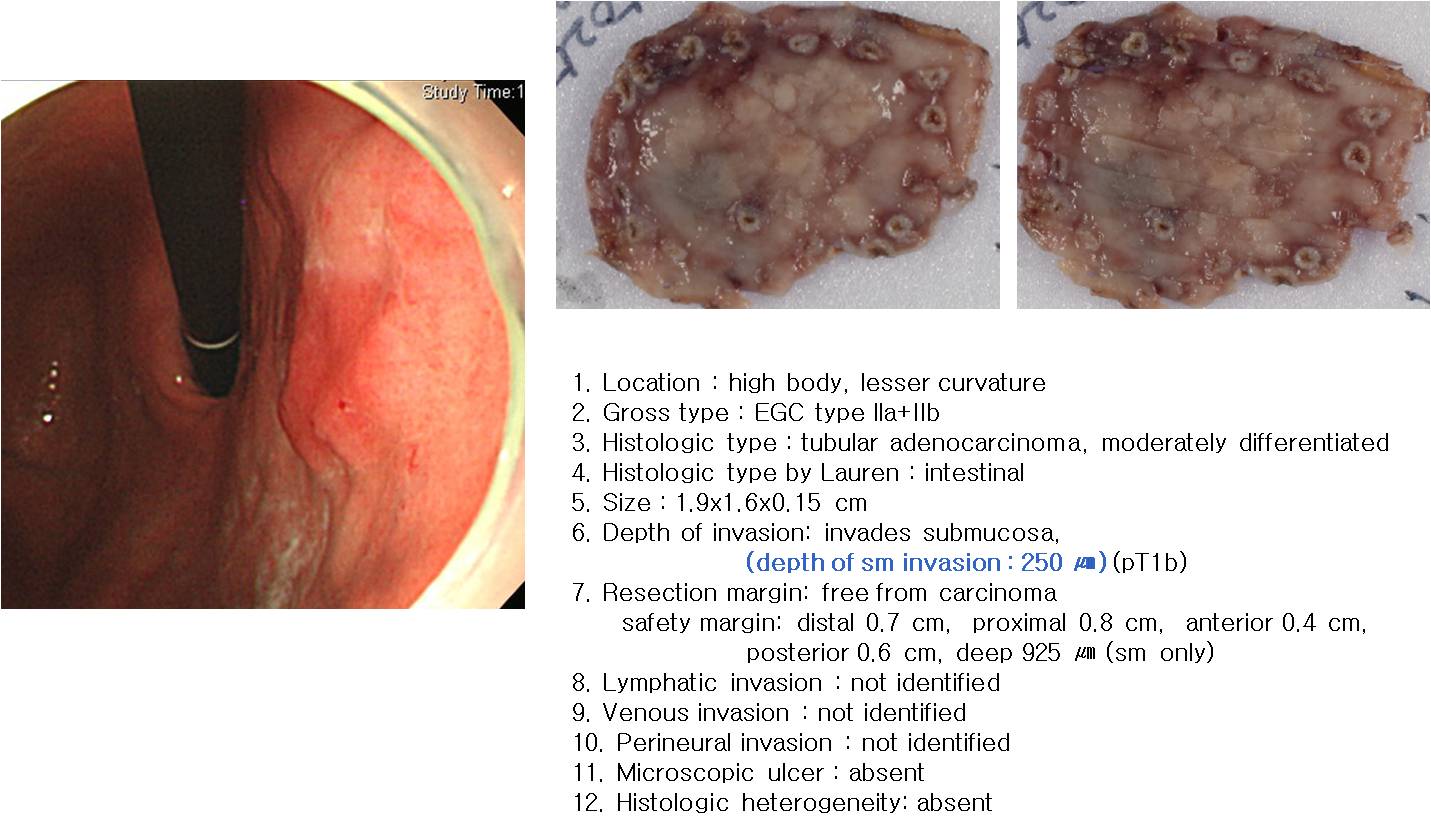
[위암 929]
57세 여성의 잔위암입니다. Initial workup CT에서 colonic invasion이 의심되었습니다.
대장내시경을 하였는데 colonic invasion이 관찰되지 않았습니다.
수술을 시행하였는데 뚜렷한 colonic invasion이 있는 것으로 나왔습니다. T4b였습니다.
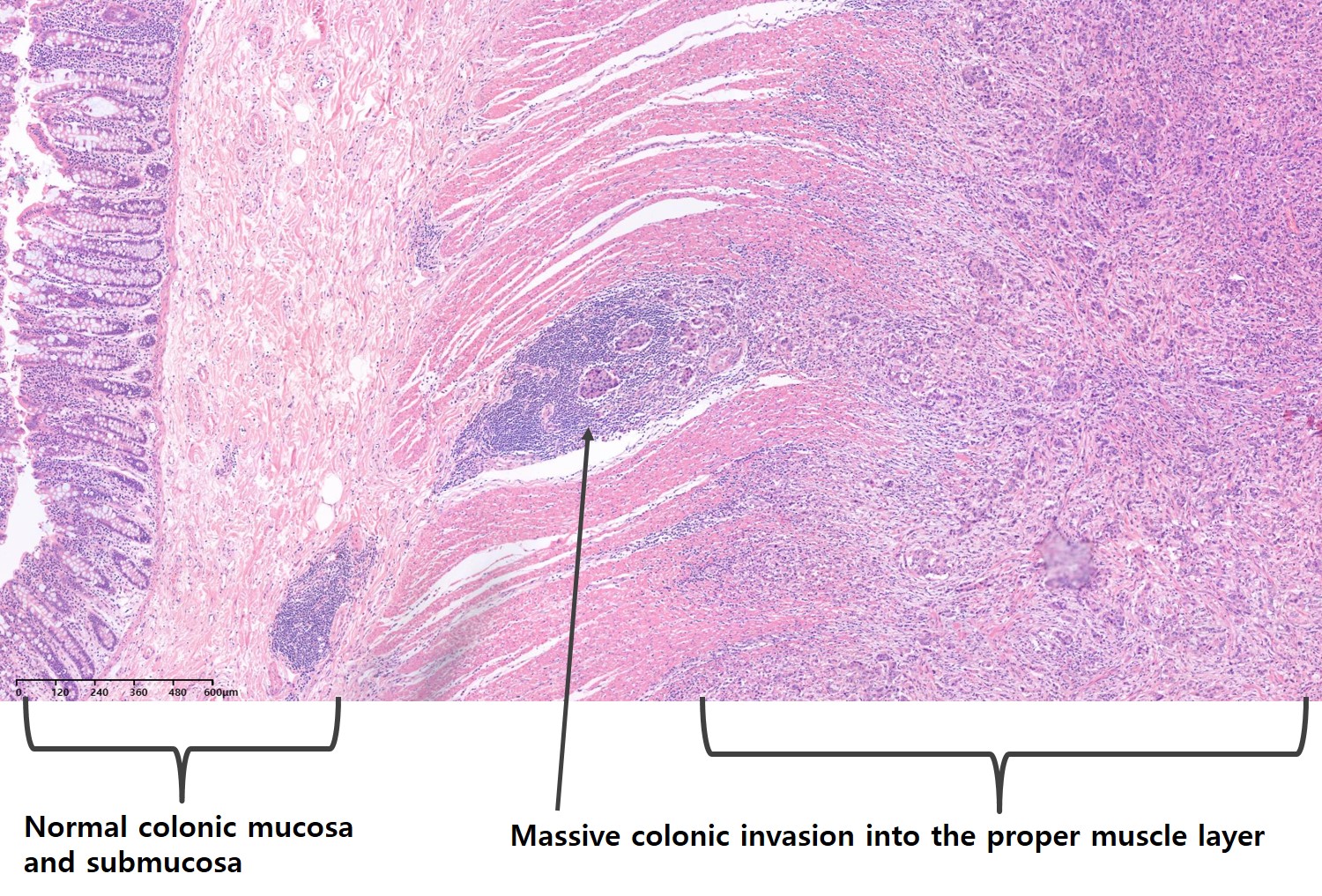
병리 사진입니다.
Massive한 대장 proper muscle invasion이 있었지만 mucosa와 submucos는 정상이었습니다. 이 떄문에 대장내시경에서 이상 소견이 발견되지 않았던 것으로 생각됩니다. Massive한 근육층 침범을 고려하면 subtle한 변화가 있었을 수도 있으나 찾아내는 것은 쉽지 않았을 것 같습니다.
Remnant gastric cancer 특히 anastomosis site cancer는 일반 위암에 비하여 direct colonic invasion이 많은 것 같습니다. Subtotal gastrectomy를 하면 colon이 문합부와 아주 가까워지기 때문인 것으로 추정됩니다.
![]() 3. 가장 무서운 암 - Borrmann type IV cancer in the remnant stomach
3. 가장 무서운 암 - Borrmann type IV cancer in the remnant stomach
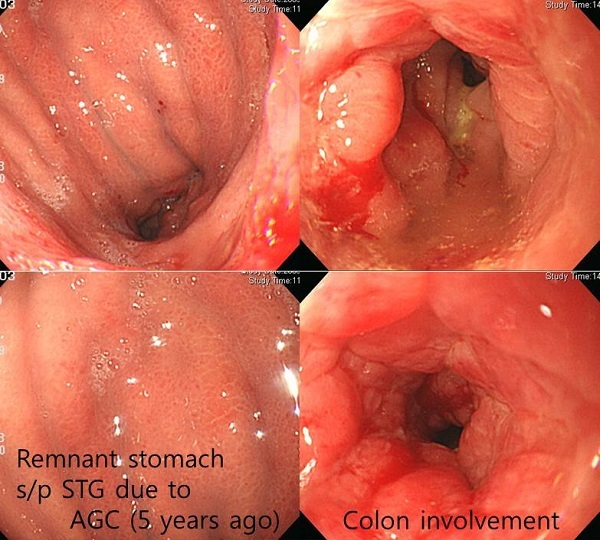
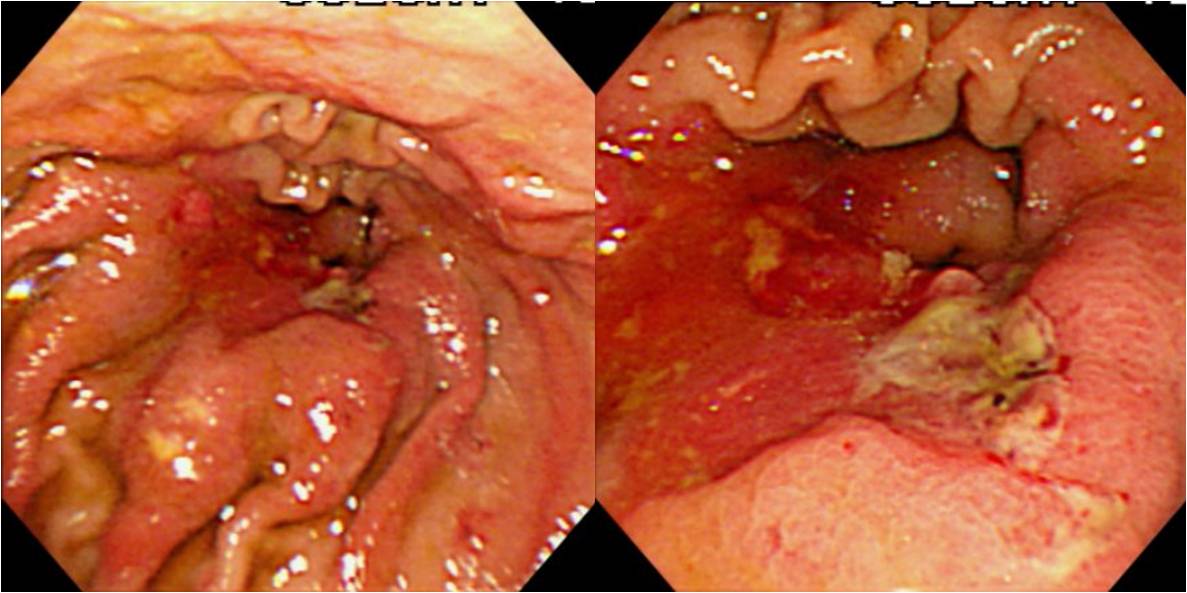
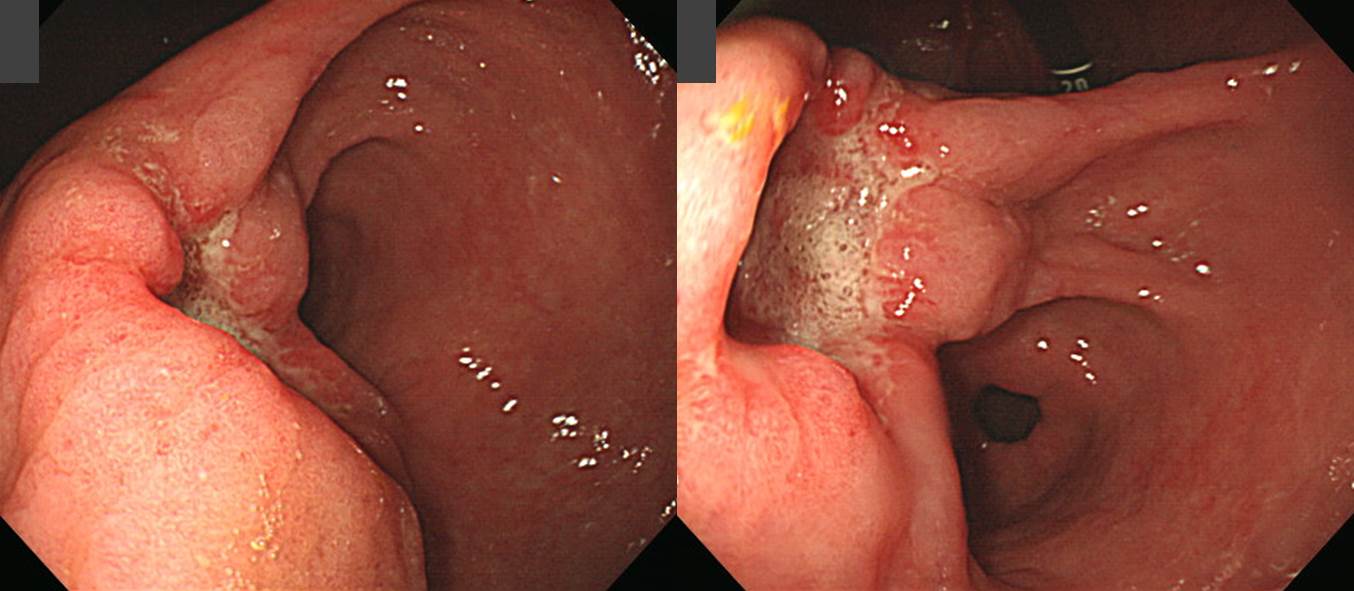
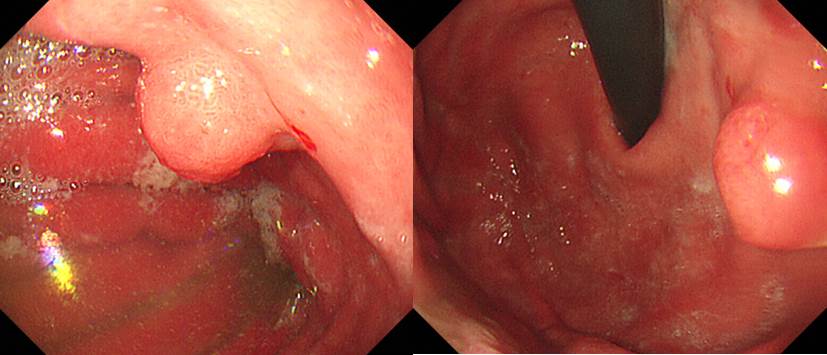
Remnant gastric cancer 중 가장 진단도 어렵고 예후도 나쁜 것은 잔위에서 발생한 보만 4형 진행성위암입니다 (EndoTODAY 20130404).
위아전절제술 5년 후 잔위의 보만 4형 진행성위암으로 진단된 환자입니다. 대장 침범도 있었습니다. 무척 진단하기 어렵습니다. 평상시에도 잔위의 점막은 약간 부어보이기 때문에 보만 4형 진행성 위암과 구분하기 어렵습니다.
또 다른 증례입니다.
[위암 660]
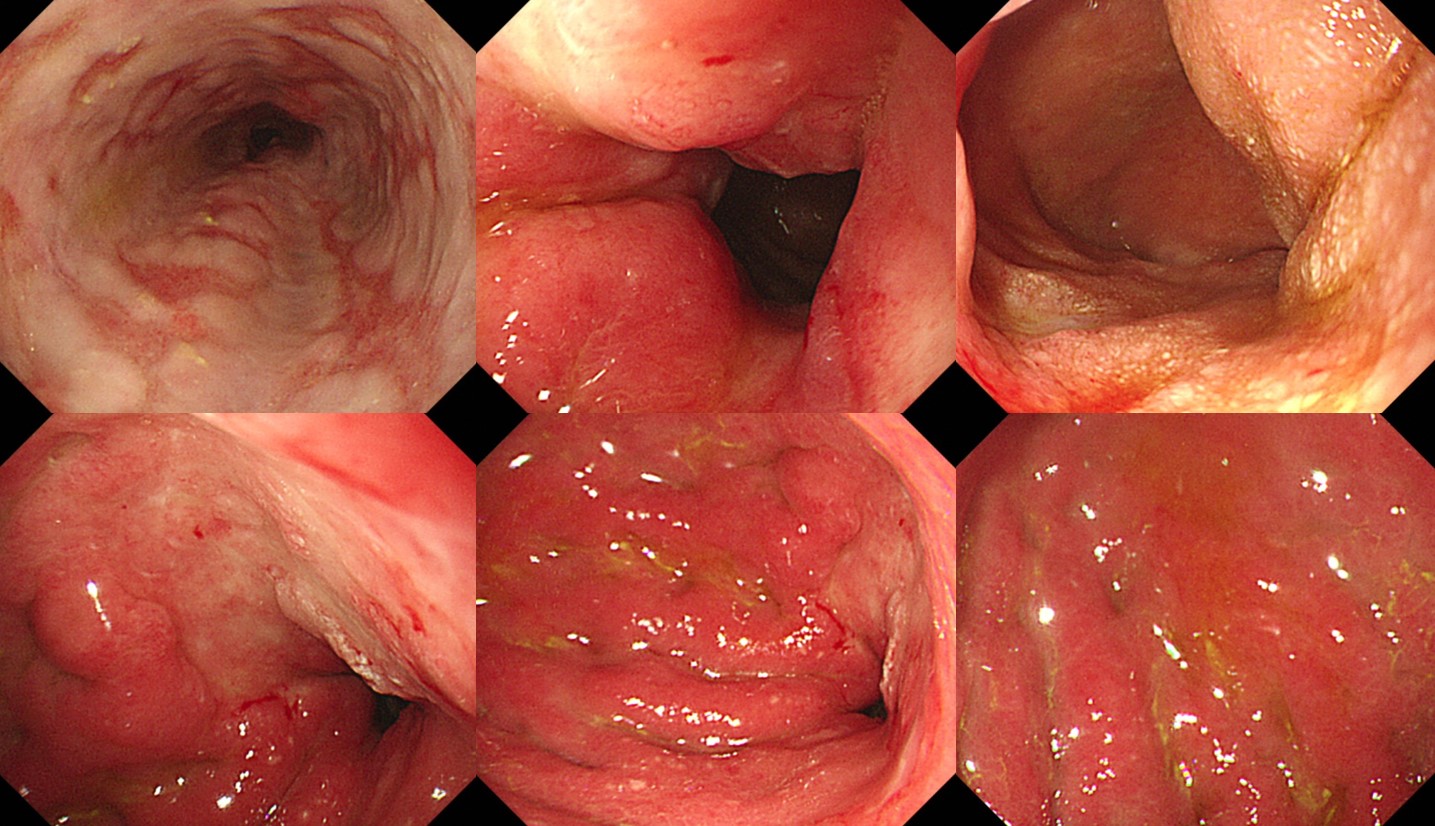
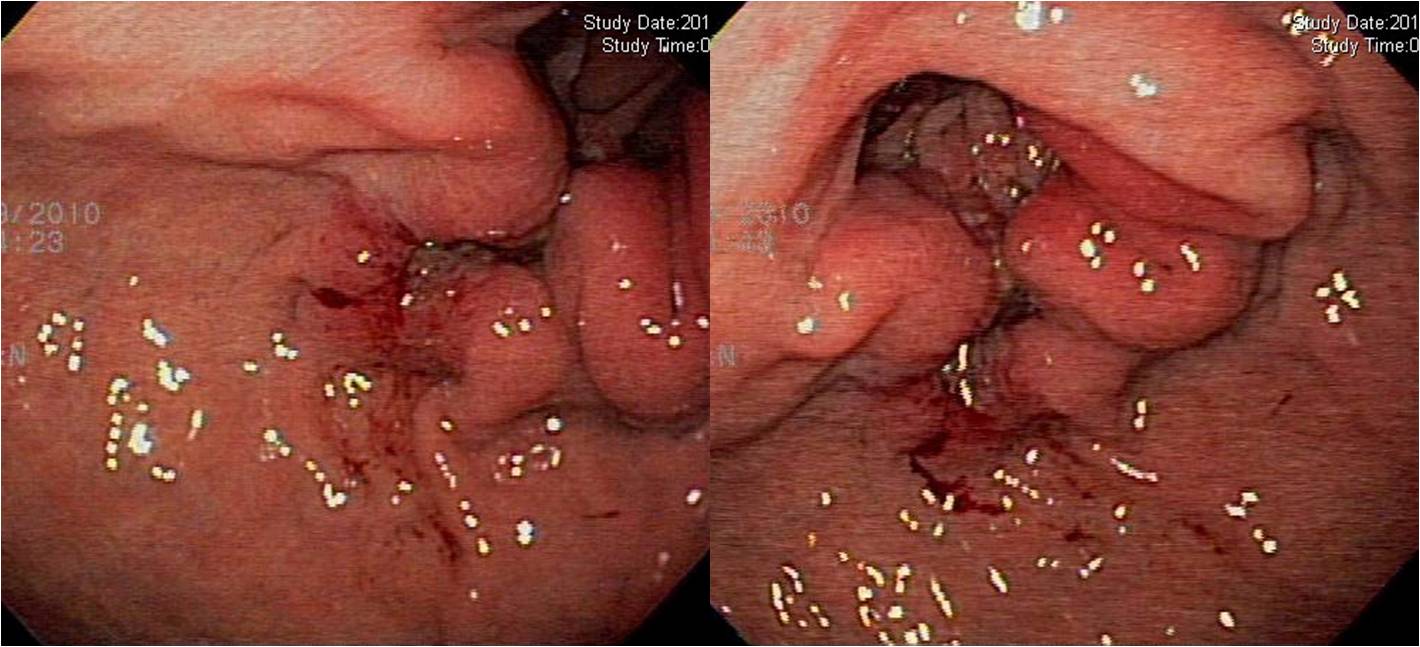
Advanced gastric cancer Borrmann type IV can be difficult to find. It is especially true after subtotal gastrectomy. Remnant stomach is difficult to see clearly. Mucosa of the remnant stomach is usually edematous, and covered with bile-tinged fluid. Subtle mucosal changes, which are critical for the diagnosis of Borrmann type IV, cannot be noticed in this setting. As a result, Borrmann type IV of the remnant stomach is usually found in far advanced stages. Curative resection is possible only in very selected cases.
In this lady, subtle ill-defined erosive lesion was found in the lesser curvature side of the remnant stomach, and the biopsy was signet ring cell carcinoma. Surgery was done, and the tumor was 11cm in diameter. Most of the remnant stomach was infiltrated by undifferentiated-type of gastric cancer.
(2015, F/60)
Left: AGC, signet ring cell carcinoma, T2N0 (proper muscle invasion)
Middle: There was no evidence of recurrence in the follow up endoscopy after surgery ( 1 year before final diagnosis of remnant gastric cancer)
Right: Remnant gastric cancer, Borrmann type IV, poorly cohesive differentiated, 11x8cm
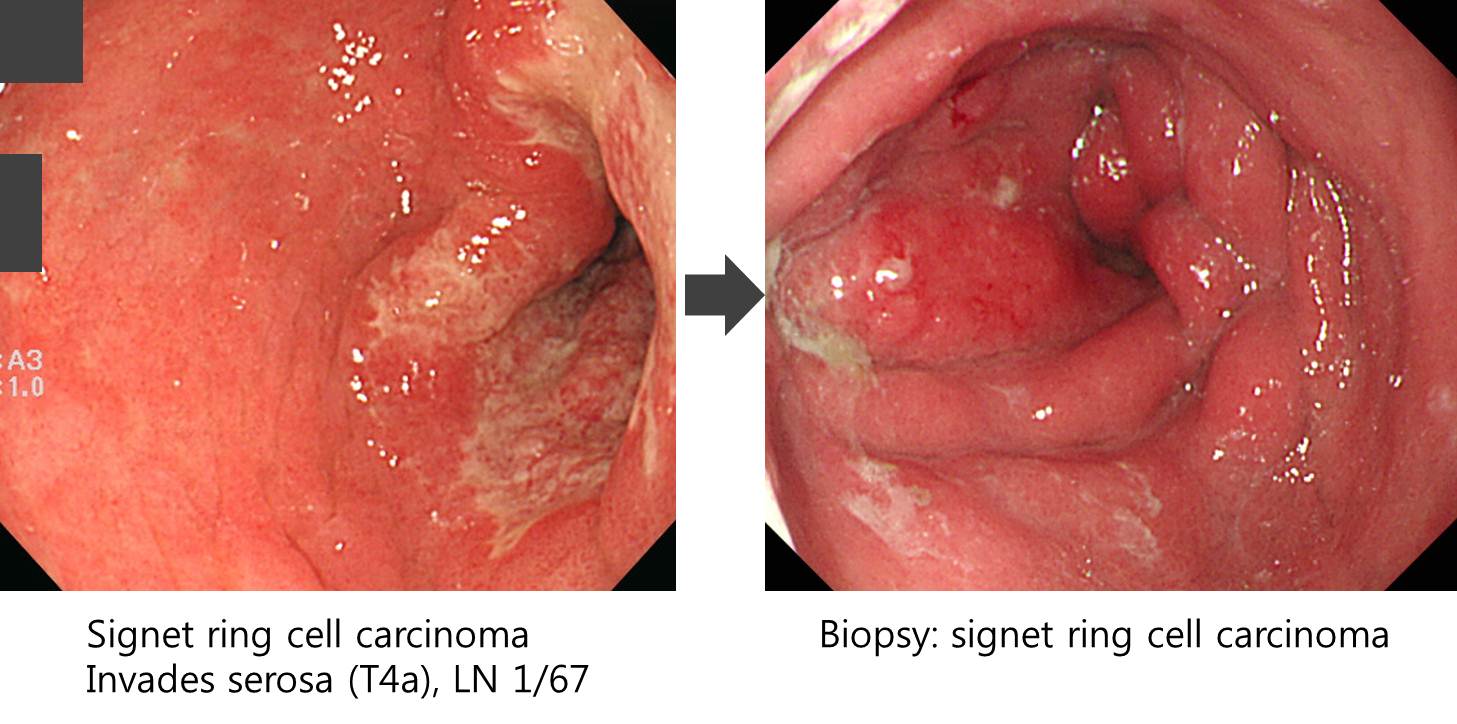
전정부 진행성 위암(signet ring cell carcinoma T4 N1)으로 subtotal gastrectomy with STG B-II 수술 및 adjuvant chemotherapy 시행받고 추적관찰 중 위내시경에서 remnant stomach의 AGC B-IV 소견이 보였습니다. 조직검사를 하였고 signet ring cell carcinoma가 나왔습니다.
[위암 380]
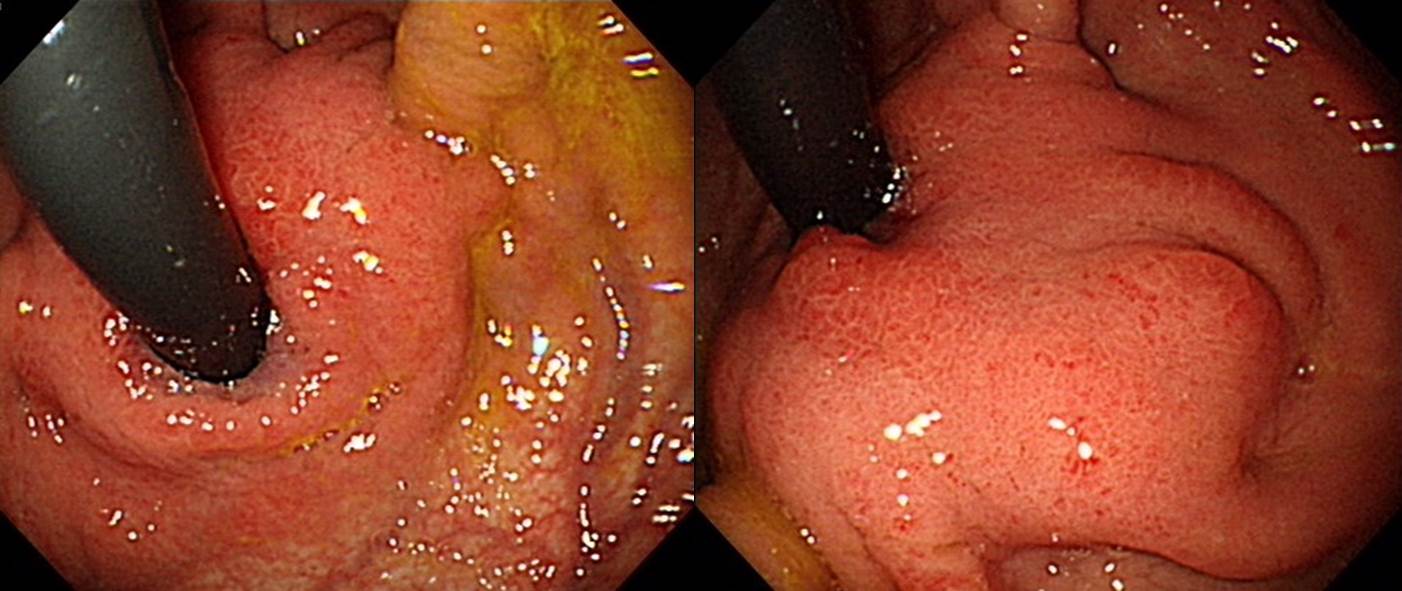
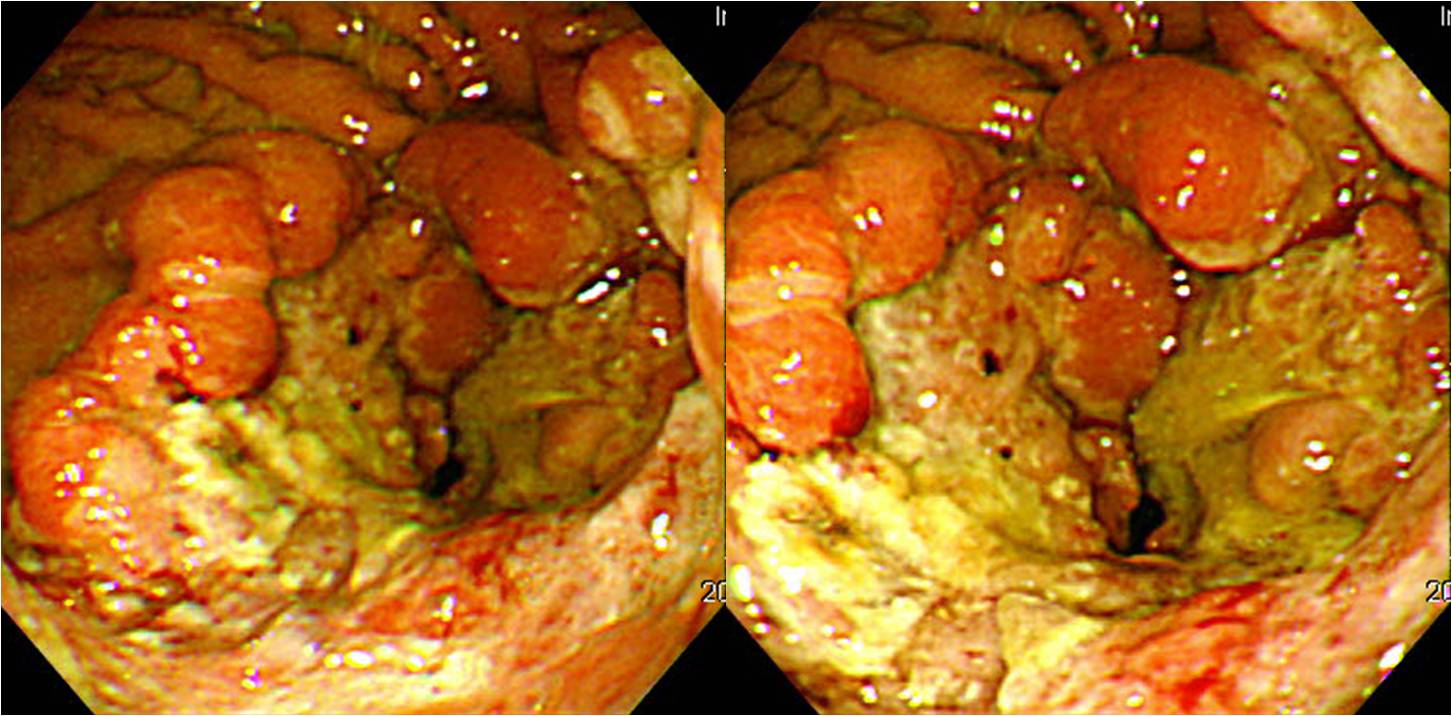
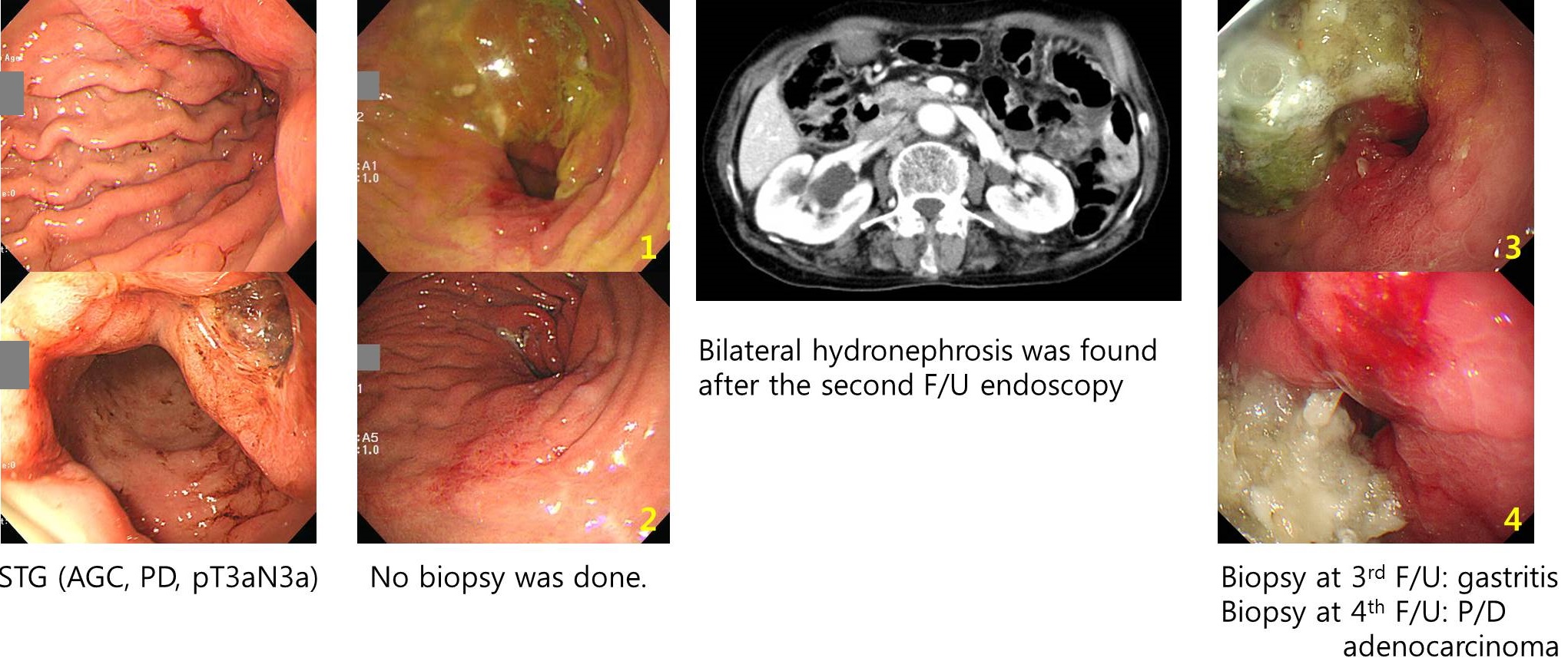
70대 여성입니다. 2012년 위암 수술을 받은 후 약 1년 반만에 재발 의심으로 의뢰되었습니다. 잔위의 anastomosis site 쪽에서 재발하셨는데 마치 보만 4형 양상으로 위벽이 두꺼워졌고 mucosal erosion이나 ulcer는 없었습니다. 첫 조직검사에서 암이 확인되지 않았습니다. 즉시 재검하였고 P/D adenocarcinoma를 확인하였습니다. 첫 수술에서 proximal resection margin이 어느 정도였는지는 확인할 수 없었습니다.
[2016년 연세대학교 소화기학 연수강좌 박준철 교수님 소개 증례]
암 중에서 가장 진단이 어려운 암이 무엇일까요? Remnant stomach의 보만 4형 진행성 위암입니다. 저는 '위암 진단의 王中王'으로 설명하고 있습니다. 박준철 교수님께서도 Remnant stomach의 보만 4형 진행성 위암 1예를 소개해 주셨습니다. 정말 어렵습니다.
[위암 484]
Dysphagia가 발생하여 내시경 재검을 받았고 암으로 나와 수술이 진행되었던 것 같습니다. M/D tubular adenocarcinoma, 6x3cm, invades adjacent structure (pT4bN0)였습니다. Cardia 근방에 국한되 보만 4형으로 나타난 잔위암으로 생각하고 있습니다 (위암 484).
![]() 4. 잔위암의 lymphatic spread 양상
4. 잔위암의 lymphatic spread 양상
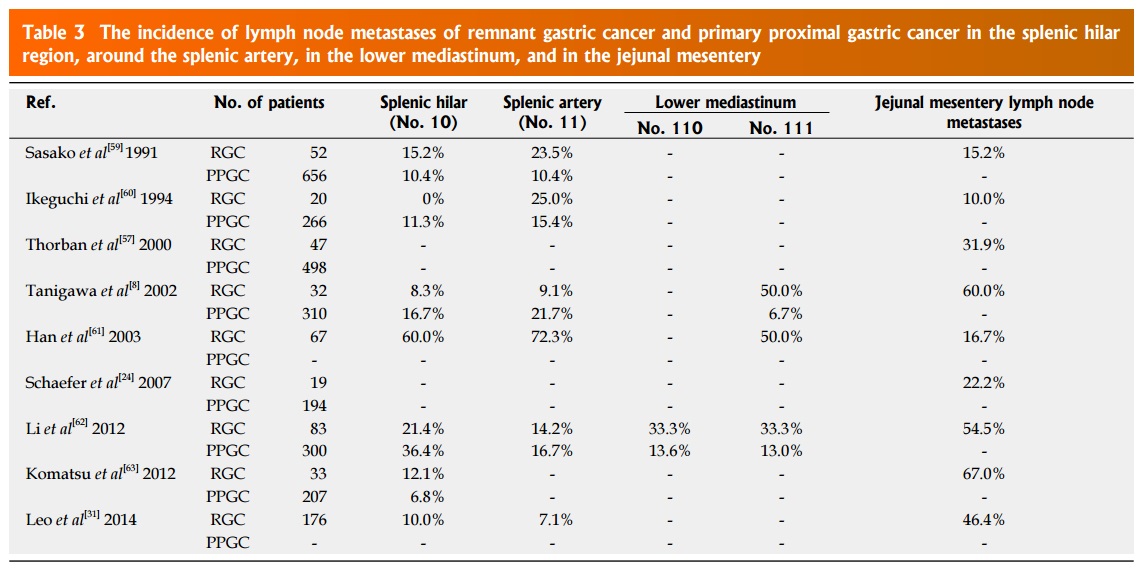
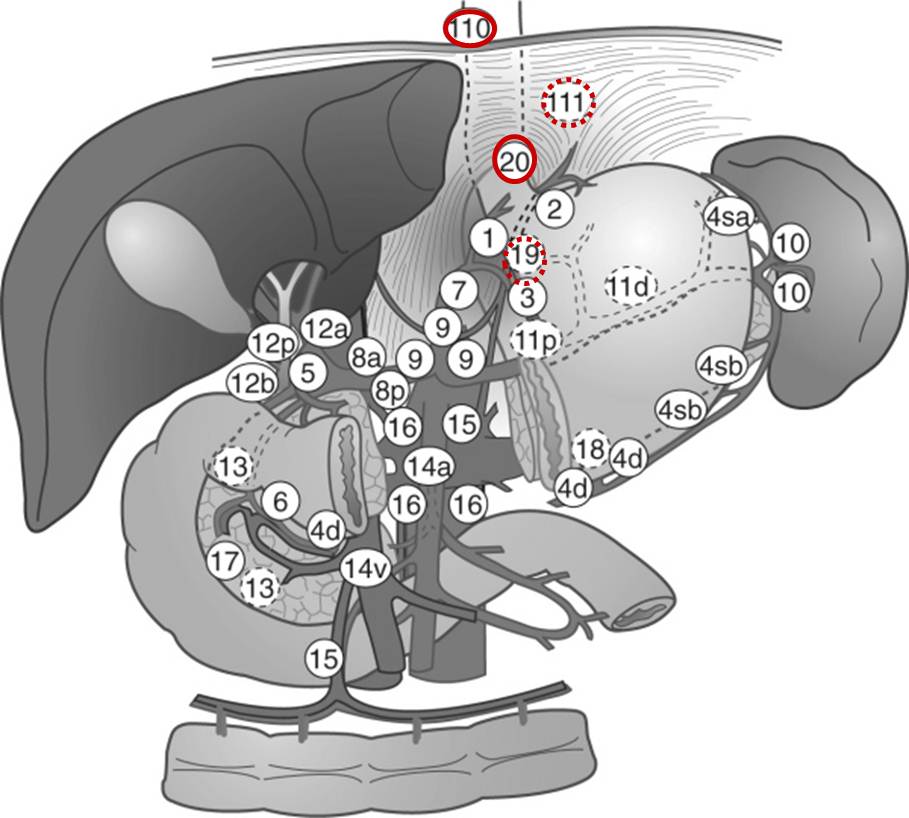
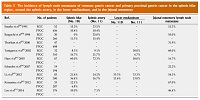
원위 위절제술 후 lymphatic drainage 양상에 변화가 일어납니다 (Ohira. WJG 2016). 아마도 수술 과정에서 정상적인 lymphatics가 절제되기 때문일 것입니다. 그 결과 잔위암과 원발성 근위부 위암(primary proximal gastric cancer)의 림프절 전이에 약간의 차이가 발견됩니다. 잔위암에서는 splenic artery (11번), splenic hilum (10번), lower mediastinum (110, 111번), jejunal mesentery의 림프절 침윤이 흔합니다.
It has been reported that RGC has unique patterns of lymph node metastasis compared with PPGC. In PPGC, the main lymphatic flow drains to the lymph nodes along the celiac artery through the lymph nodes at the lesser curvature, the left gastric artery, and the right side of the cardia. In RGC, it has been considered that the characteristics of lymph node metastases are different from PPGC because abnormal lymphatic formation is induced as a result of cutting off these lymphatic pathways at the initial surgery. Furthermore, Tokunaga et al mentioned that altered lymphatic drainage after DG may affect the long-term survival of RGC patients with advanced stage disease. Previous studies have investigated the incidence of lymph node metastasis focusing on around the splenic artery, in the splenic hilum, at the lower mediastinum, and in the jejunal mesentery. Some authors demonstrated a higher incidence of lymph node metastasis around the splenic artery, in the splenic hilum, and at the lower mediastinum in RGC; therefore, lymphadenectomy of these regions is recommended for curative surgery. In patients with previous B-II reconstruction, the rate of lymph node metastases in the jejunal mesentery has been reported to be 10.0%-67%. Thorban et al reported that RGC patients with lymph node metastases in the jejunal mesentery had a poor prognosis, with a median survival time (MST) of 13.2 mo. Similarly, Leo et al reported that RGC patients with lymph node metastases in the jejunal mesentery had worse outcomes than those with metastases in other lymph node stations. Therefore, jejunal mesentery lymph node dissection including the origins of each involved jejunal artery is recommended for RGC patients with previous B-II reconstruction. However, the details of the spread of lymph node metastases in RGC patients are still uncertain, because the number of patients examined in these studies was too small. (Ohira. WJG 2016)
보다 상세한 자료는 2022년 6월 29일 EndoTODAY webseminar에서 안지영 교수님께서 잘 정리해 주셨습니다.
Splenic hilar node와 jejunal mesenteric node에 대한 치료 전략이 중요합니다.
Early stage의 잔위암에서는 림프절 전이가 없었다는 자료
암 수술 후 발생한 잔위암에서의 림프절 전이 양상
암이 아닌 benign disease 수술 후 발생한 잔위암에서의 림프절 전이 양상
2018년 일본 가이드라인은 잔위암 수술 시 림프절 절제술에 대한 내용과 이에 대한 수정 의견
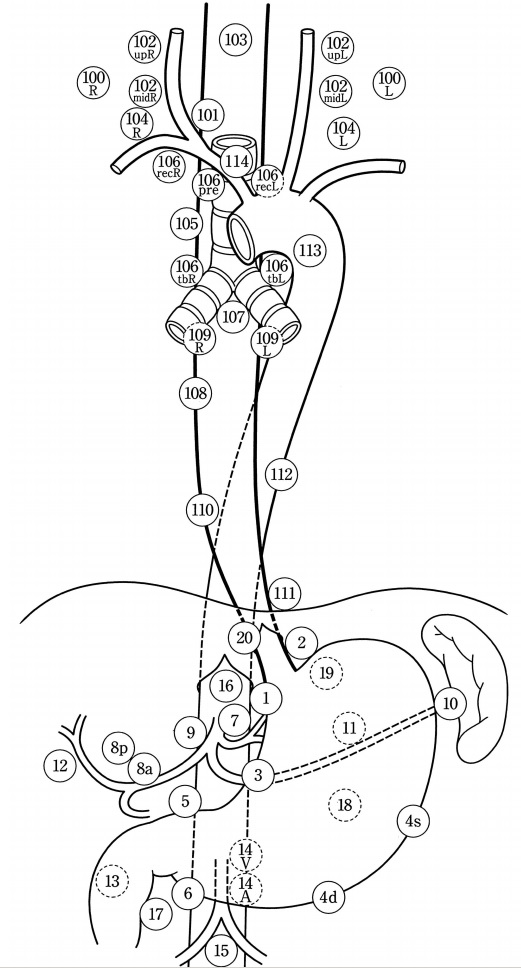
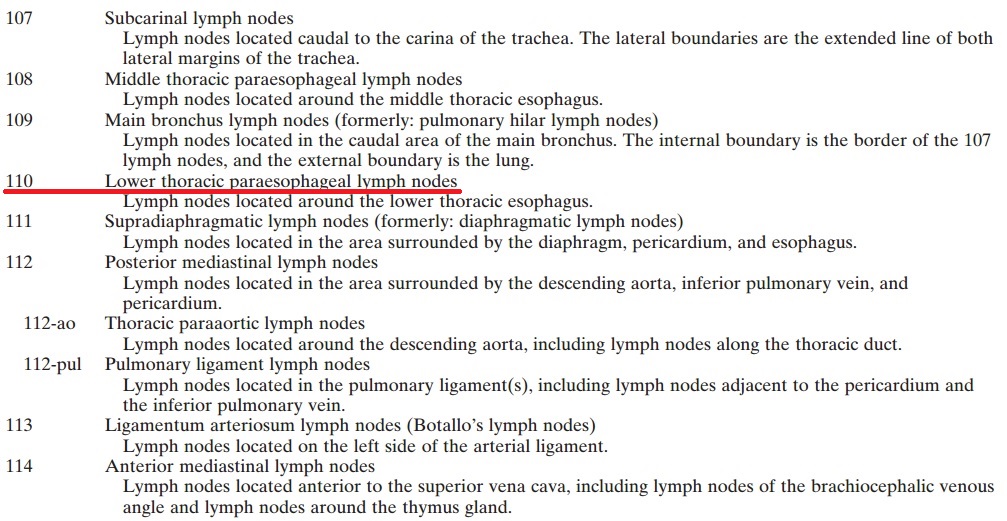
미국와 일본의 흉부 림프절 명명법이 서로 다릅니다. 위 table에서 언급된 110, 111번은 일본식입니다. 미국 흉부외과쪽에서는 조금 다르게 부릅니다. 예를 들어 lower paratracheal nodes는 일본식으로는 110번, 미국식으로는 8L번입니다.
| 위치 | 서양식 | 일본식 |
| Lower paratracheal nodes | 8L | 110 |
| Diaphragmatic nodes | 15 | 111 |
| Paracardial nodes | 16 | 1 (右) 또는 2 (左) |
1) AJCC 7판에 따른 림프절 명명법
1L = left supraclavicular, 1R = right supraclavicular, 2L = left upper paratracheal, 2R = right upper paratracheal, 4L = left lower paratracheal, 4R = right lower paratracheal, 5 = aortopulmonary, 6 = anterior mediastinal, 7 = subcarinal, 8L = lower paraesophageal, 8M = middle paraesophageal, 9 = pulmonary ligament, 10L = left tracheobronchial, 10R = right tracheobronchial, 15 = diaphragmatic, 16 = paracardial, 17 = left gastric, 18 = common hepatic, 19 = splenic, 20 = celiac. The posterior mediastinal lymph node (3P) is not shown.
2) 일본 식도질환학회 림프절 명명법 (Esophagus 2004;1:61-88)
![]() 5. 잔위의 Helicobacter 제균치료
5. 잔위의 Helicobacter 제균치료
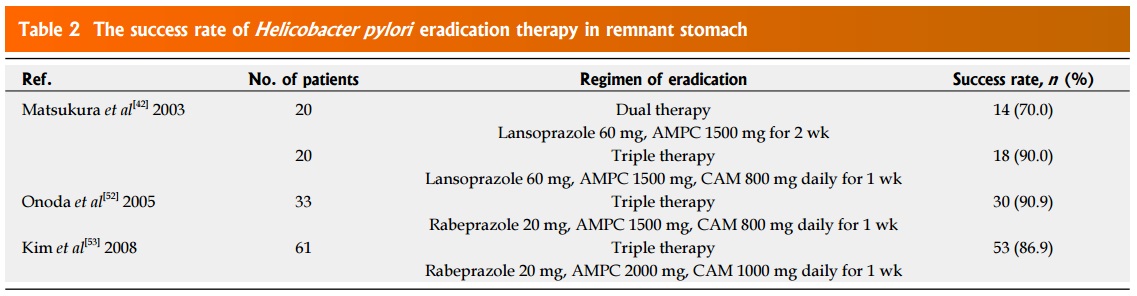
원위 위절제술 후 Helicobacter 제균율이 다소 낮아질 것이라는 우려가 있습니다만, 몇몇 연구에서 그렇지 않다고 보고된 바 있습니다 (Ohira. WJG 2016). 종설에 실린 마지막 연구는 우리나라 국립암센터 김찬규 선생님의 2008년 Am J Gastroenterology 논문이어서 반가웠습니다.
![]() 6. 잔위암의 수술적 치료
6. 잔위암의 수술적 치료
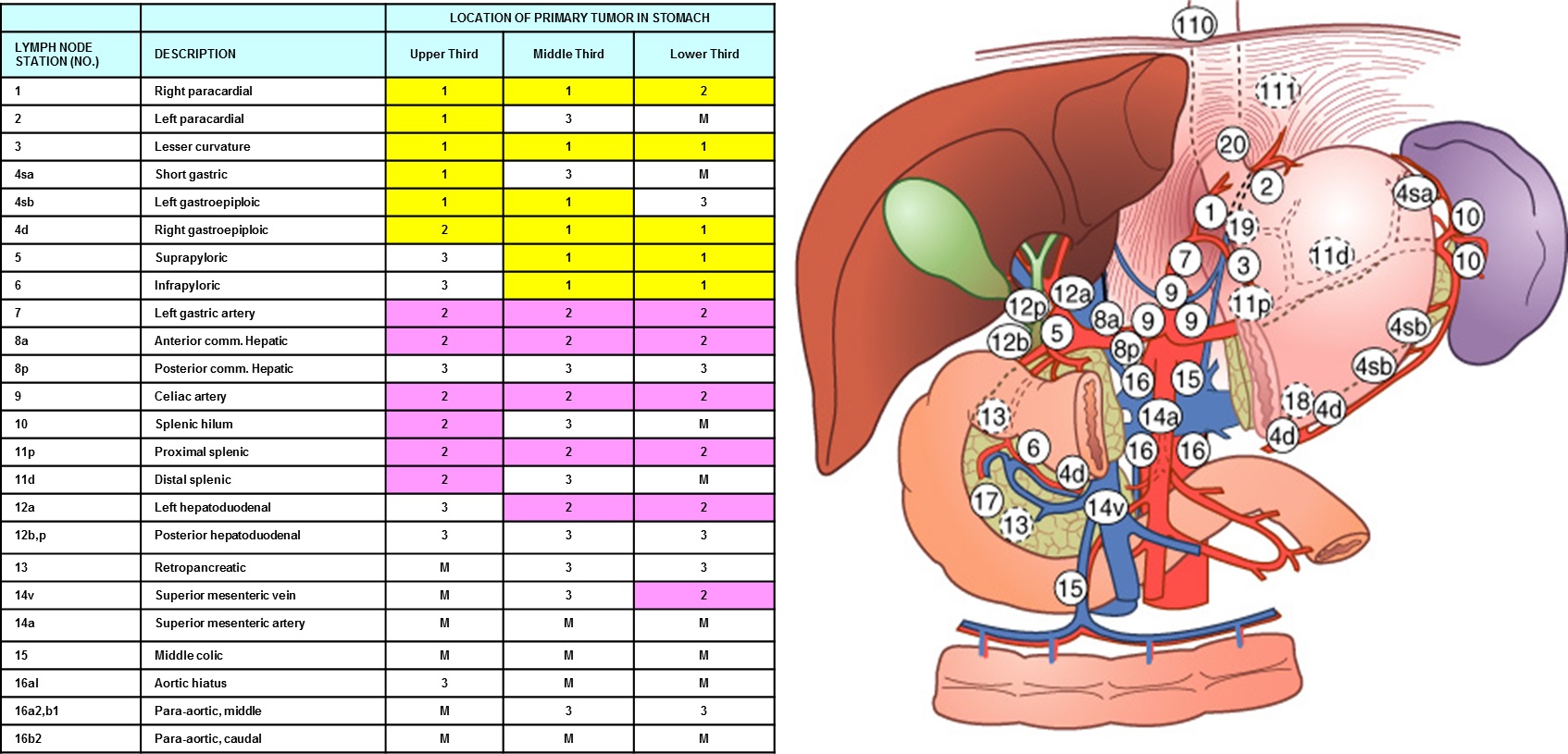
2007년 삼성서울병원 외과에서 잔위암 수술예를 분석한 바 있습니다 (An JY. Am J Surg 2007). 당시 primary upper 1/3 cancer와 survival이 비슷했습니다.
The mean interval between previous gastrectomy and diagnosis of remnant primary gastric cancer was 18.8 years for patients who had undergone their first gastrectomy for malignant disease (n = 13) and 28.6 years for patients with benign disease (n = 25). Patients with remnant primary gastric cancer showed a greater male predominance compared with patients having upper one-third cancer (92.1% vs 65.5%, respectively, P = .001). Patient distribution according to operative curability, tumor size, stage, and histology showed no significant differences between the 2 groups. Overall 5-year survival rates of patients with remnant primary gastric cancer and those with upper one-third cancer were 53.7% and 62.9% (P = .346), respectively. Differences in the 5-year survival rates at each stage between the groups were not statistically significant.
![]() 7. 잔위암의 내시경 치료
7. 잔위암의 내시경 치료
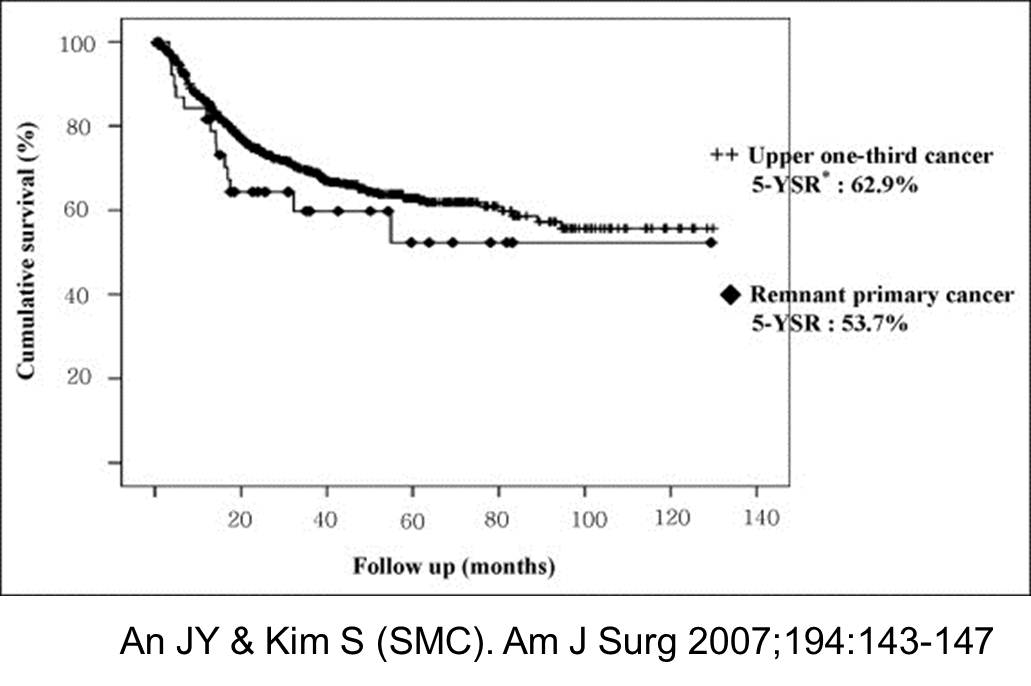
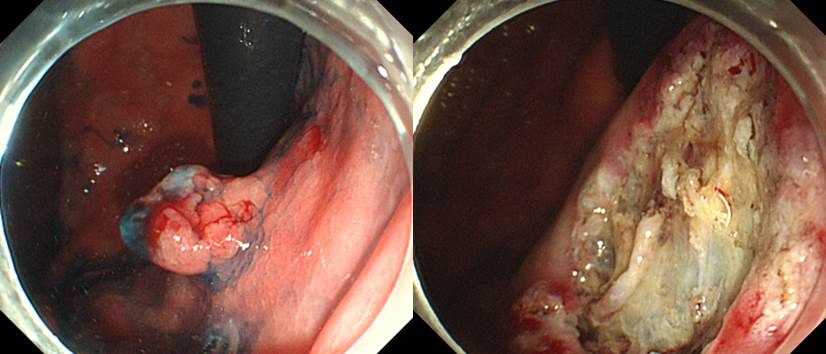
삼성서울병원의 잔위암 ESD 결과를 소개합니다 (Lee JY. Clin Endosc 2016). 약 절반 정도가 suture line에 위치하고 있었는데 다행스럽게 시술은 잘 되었고 재발도 없었습니다.
Results: Two-thirds of the lesions were located on the body, and half were located on the suture line. En bloc resection, R0 resection, and en bloc with R0 resection rates were 88.9%, 100%, and 88.9%, respectively. Curative resection rate for EGC was 91.7%. Perforation occurred in one patient (5.6%) and was successfully managed by endoscopic closure with metallic clips and conservative management. There was no significant bleeding after ESD. During a median follow-up of 47.5 months, no local, metachronous, or extragastric recurrence was seen for either EGC or adenoma lesions.
Fig. 1. (A) A 1.5-cm, flat, elevated-type early gastric cancer (arrows) is noted on the suture line (arrowheads) of the lesser curvature of high body in the remnant stomach. (B) Chromoendoscopy with indigo carmine dye. (C) Dissection of the submucosal layer after circumferential incision of the mucosa. Staples (arrowhead) and severe fibrosis are observed around the suture line. (D) The tumor is completely removed by en bloc resection.
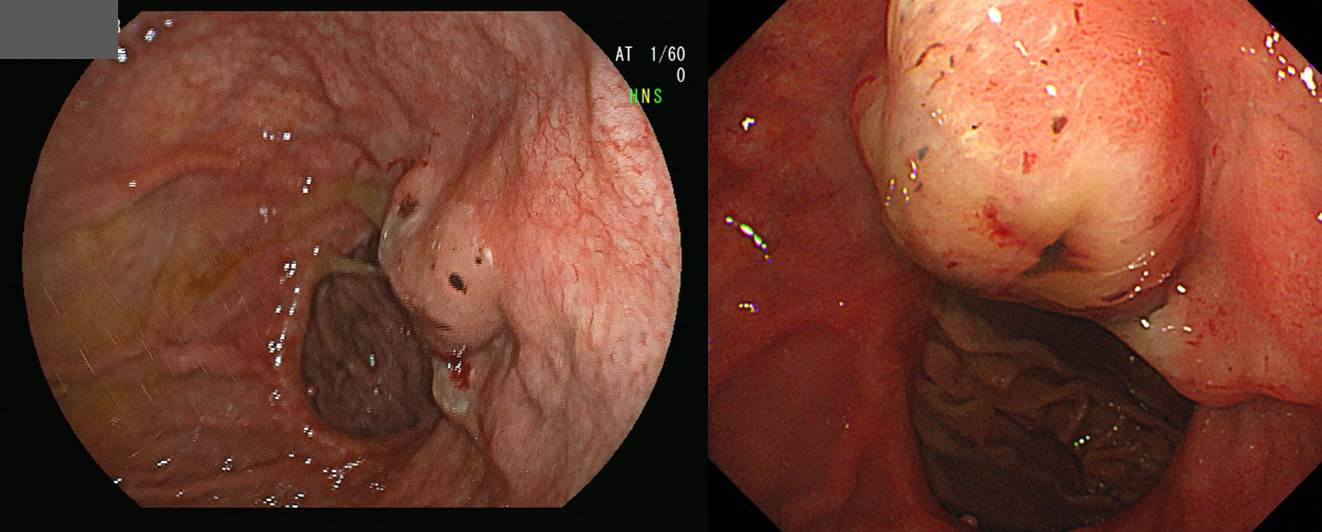
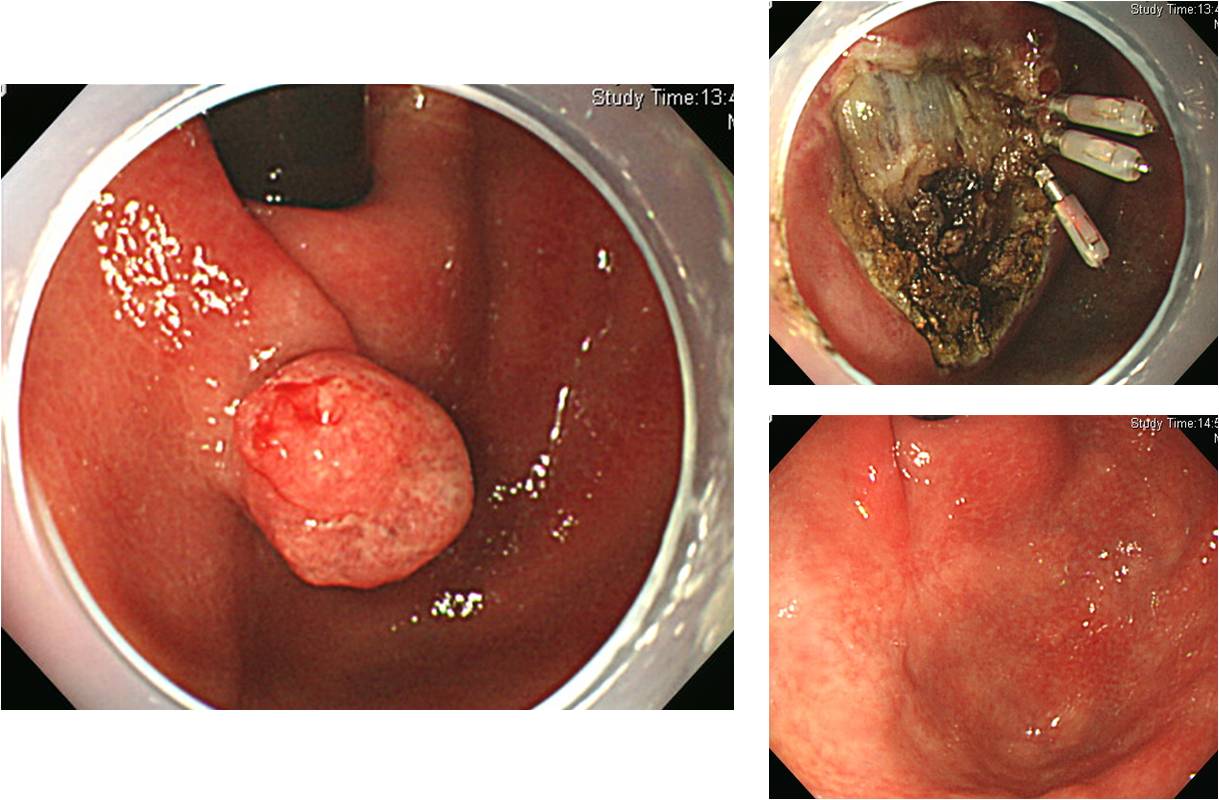
[2016-10-27. 목요집담회 증례]
잔위암이었습니다. ESD를 시행하였습니다. 병소의 깊이에 비하여 조금 더 많이 돌출된 형태였습니다. Gastritis cystica profunda가 있었기 때문으로 추정하였습니다.
Stomach, endoscopic submucosal dissection:
Early gastric carcinoma
1. Location : high body, lesser curvature
2. Gross type : EGC type IIa
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 12 mm (2) vertical diameter, 9 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 2 mm, proximal 2 mm, anterior 4 mm, posterior 2 mm
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
13. Associated finding: gastritis cystica profunda
[More cases of ESD for remnant cancer]
36밀리, 미분화 혼재암, MM
Early gastric carcinoma
1. Location : body, lesser curvature
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 5 mm (2) vertical diameter, 4 mm
6. Depth of invasion : invades mucosa (muscularis mucosa) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 2 mm, proximal 10 mm, anterior 10 mm, posterior 12 mm
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
잔위 선종으로 inject and cut 후 360도 marginal ablation treatment 시행하였습니다. 잔위가 매우 작아서 내시경을 마음대로 움직일 공간이 부족했습니다.
![]() 8. subtotal gastrectomy 후 추적관찰
8. subtotal gastrectomy 후 추적관찰
[2014-7-4. 애독자 질문]
안녕하십니까? 요즘 제가 고민하고 있던 이슈에 대해 많은 연구적 근거 및 고민들을 보내주셔서 감사합니다. 추적 내시경에 대하여 또 다른 이슈가 있습니다. 바로 부분 위절제술을 받은 환자군입니다. 그럼 Distal gastrectomy이 후의 진료 strategy는 어떤지.. 그리고 그 때의 Helicobactor의 감염에 대해서는 검사하는 건 의미가 있는지요. 물론 저는 매번 외과 선생님의 처방에 따른 검사만 할 뿐 여기에 대해서 자세히 고민하진 못했습니다. 흔한 위암 발생 부위인 antrum이 없어지고 upper body나 midbody까지만 남아 있는 상황에서 얼마나 자주 어떤 방식으로 검사하는 것이 좋은건지요? 공부할께 너무 많지만 교수님의 메일을 하루에 한번씩 공부하는 기분으로 열어보며 출근하는 기쁨이 큽니다. 감사합니다.
[2014-7-6. 이준행 답변]
Subtotal gastrectomy 후 최적의 추적관찰에 대한 정답은 없을 것 같습니다. 2010년 서울대 외과 공성호 교수님의 조기위암의 수술 후 추적관리 (J Korean Med Assoc 2010;53:324 - 330)를 여러분과 함께 읽어봅니다. 매우 잘 정리된 종설이므로 길게 인용하겠습니다.
PDF 0.5 M
"조기위암의 수술 후 추적관리 프로그램의 필요성
2% 이내의 재발률을 보이는 조기위암에서 증상이 없는 환자를 포함한 모든 환자를 대상으로 재발 여부를 관찰하기 위한 추적관찰 프로그램이 필요한 것일까? Kodera 등은 2003년 위암 수술 후 재발이 증상 없는 상태에서 일찍 발견된 경우와 증상이 생긴 이후 발견된 경우의 환자를 비교하여, 일찍 발견된 경우 발견된 이후의 생존 기간은 더 길었으나 전체적인 수술 후 총 생존률의 차이는 없다는 자료를 바탕으로 위암 재발 발견을 위한 추적관리 프로그램이 생존 증가에 기여하는 증거는 없다는 내용을 발표하였다. 그럼에도 항암화학요법이 계속 발전하고 있는 지금, 가능한 한 조기에 재발을 발견하여 재발에 따른 증상을 완화하고 생존율을 향상시키기 위해 노력하기 위한 추적관리 프로그램이 필요하다는 것에 대해서는 대부분의 의사들이 동의하는 것으로 보인다.
한편, 위절제술 후 잔위에 생긴 위암의 경우에는 재발의 조기 발견이 생존율 향상에 도움이 될 것으로 보인다. 잔위암의 경우에는 근치적 절제가 되지 않는 경우가 30%정도로 비교적 높게 보고되어 있으나, 조기 진단된 경우 절제율과 생존율이 증가될 수 있다. 특히 위암의 발생률이 높은 우리나라의 경우 잔위 초발암의 발생 가능성이 적어도 일반인과 같은 수준이거나 더 높을 것으로 추정되기 때문에 위부분절제술을 받은 환자에서 내시경을 이용한 검사는 꼭 필요한 것으로 보인다.
한편 재발이 없는 98%의 환자, 특히 증상이 없는 환자들에게서 추적관리의 의미에 대해서는 체계적으로 분석된 연구가 없으나 기대 여명이 길어지고 삶의 질에 대한 관심과 중요성이 커지는 현시점에서 재정립할 필요가 있을 것으로 보인다."
공성호 교수님의 의견을 간단히 요약하면, 원발암의 재발을 발견하기 위한 노력은 생존률 향상에 기여하지 못하는 반면, 잔위암의 발견은 생존율 향상에 기여할 것으로 생각된다는 것입니다. 이에 대해서 저도 동의합니다. 그러나 추적관찰의 필요성 여부가 생존률 향상에만 있는 것은 아닙니다. 재발하지 않았다는 것을 확인하는 것(reassurance)도 중요합니다. 암 환자에게는 건강을 확신하고 행복하게 사는 것도 매우 중요한 일이니까요.
먼저 추적관찰 간격을 생각해봅시다. 그야말로 정답이 없는 문제입니다만, 과거 우리나라 외과의사들을 대상으로 조사한 결과(대한위암학회 설문조사)에 따르면 6개월 간격이 가장 보편적인 것 같습니다. 임상의사의 입장에서 적당하다고 생각합니다. 다시 인용합니다.
"추적관리의 간격은 수술 후 2~3년까지의 경우 진행위암은 3개월 이하 42.2%, 4~6개월 54.4%, 12개월 3.3%였으며, 조기위암은 20%, 70%, 10%였다. 3년이 지난 후 추적관리의 간격은 진행위암은 3개월 이하, 4~6개월, 12개월이 각각 20%, 55.6%, 23.6%였으며, 조기위암은 7.8%, 56.7%, 35.6%인 것으로 응답되었다."
다음은 추적검사 중단시점입니다. 조기위암은 재발률은 낮지만 재발 시점은 진행성 위암보다 늦어지는 경향이 있습니다. 다시 인용합니다.
"조기위암의 재발은 그 발현 시점이 다소 늦은 경향을 보인다고 보고된 바 있다. Lee 등의 보고에서도 3년 이후 재발한 환자는 28.6% (6/21)에 이른다. Sano 등의 보고에서도 National Cancer Center의 환자들은 무려 55% (11/20)의환자들이 3년 이후에 재발하였으며, 20개의 보고를 정리한 결과에서도 평균 재발시간은 40개월(최소값 4개월, 최대값 183개월), 5년 이후에 재발한 경우는 23% (28/123명)에 이르는 것을 나타나 조기위암이라는 이유로 추적관리 기간을 짧게 정하는 것은 근거가 충분치 않은 것으로 보인다."
진행성위암의 경우는 어떠할까요? 저는 조기위암과 진행성위암의 수술 후 추적관찰이 달라야 할 뚜렷한 이유를 알지 못합니다. 다만 진행성 위암의 재발률이 훨씬 높기 때문에 추적관찰을 좀 더 자주하는 경향일 뿐입니다. 환자 입장에서는 검사를 소홀히 해서 위암 재발이 늦게 발견되어 치료기회를 놓쳤다고 생각하기 쉽지만, 의학적 근거는 그렇지 않습니다. 복막 전이, 간 전이, 뼈 전이 등을 조금 일찍 발견하더라도 예후에는 큰 차이가 없을 것입니다. 다만 수술이나 항암치료가 급격히 발전되고 있으므로 앞으로는 달라질지 모릅니다. 대장암의 경우에는 절제할 수 있는 모든 전이병소는 수술로 절제하는 경향입니다. 위암에도 비슷한 전략이 적용될 날이 올 수도 있으니까요...
![]() [FAQs]
[FAQs]
[2021-7-4. 삼성서울병원 소화기병심포지엄 실시간 질문]
잔위암 발견을 위해 검사 스케쥴은 어떻게 하시는지요/ 평생 매년인가요?
[2021-7-8. 이준행 답변]
Academic한 부분과 실제 현장에서의 관행이 매우 다릅니다. Academic한 부분은 엔도투데이에서 과거 한 애독자의 질문에 대한 저의 답변(http://endotoday.com/endotoday/remnant.html#followup)을 참고하시기 바랍니다.
실제 현장에서의 관행은 '수술 후 3년까지는 6개월에 한번 내시경 이후로는 평생 1년에 한번 내시경'입니다.
[2021-7-4. 삼성서울병원 소화기병심포지엄 실시간 질문]
십이지장으로 전이된 암으로 나타나는 경우가 있는지요?
[2021-7-8. 이준행 답변]
두 가지 경우가 있습니다. (1) 먼저 좀 더 드문 경우인데요, distal resection margin이 충분하지 않은 경우 문합부 하단의 재발암으로 나올 수 있습니다. 이 경우는 내시경 검사가 나름대로 의미가 있습니다. 뒤늦게라도 수술할 수 있기 때문입니다. (2) 보다 흔한 경우는 복막에서 재발하면서 소장이 눌려서 extrinsic compression 형태로 보이는 경우입니다. 이런 경우 curative surgery는 거의 불가능합니다. 내시경에서 발견되었지만 내시경 자체의 survival gain은 없다고 판단할 수 밖에 없는 경우입니다.
[2021-7-4. 삼성서울병원 소화기병심포지엄 실시간 질문]
Borrmann type IV가 의심되는 경우에 조직검사 방법을 다르게 해야 진단률을 향상 시킬 수 있을 것 같은데, 추천하시는 방법이 있으신가요
[2021-7-8. 이준행 답변]
보만 4형 진행성 위암의 조직검사의 요점은 미란이나 궤양부를 잘 찾아서 정확히 target biopsy 하는 것입니다. 만약 미란이나 궤양부가 없으면 주름의 top에서 검사하는 것과 골짜기의 바닥에서 검사하는 것의 정확도는 거의 비슷합니다. 흔히 bite on bite 방법의 조직검사를 하지만 정말로 도움되는지 명확하지 않습니다. 보만 4형 진행성 위암이 의심되지만 조직검사에서 나오지 않으면 내시경 재검을 하면서 동시에 위를 팽창시킨 프로토콜로 stomach CT를 찍어서 함께 보는 것이 좋습니다. 영 의심되지만 암이 확인되지 않으면 지체없이 진단적 개복술을 할 것을 권합니다. 조직검사 못지 않게 내시경 소견이 중요합니다. 어쩌면 내시경 소견이 더 중요합니다.
[2021-7-4. 삼성서울병원 소화기병심포지엄 실시간 질문]
보만 4형 진행성 위암에서 CT, CEA검사가 도움이되나요?
[2021-7-8. 이준행 답변]
Stomach protocol의 CT는 분명 도움이 됩니다. 그러나 CEA는 의문입니다. 높아졌으면 의미가 있지만 높아져있지 않으면 CEA 검사는 무시하면 좋겠습니다.
[2021-7-4. 삼성서울병원 소화기병심포지엄 실시간 질문]
잔위의 보우만 4형 진행성위암은 어떤 것을 주로 유의하시나요?
[2021-7-8. 이준행 답변]
잔위는 관찰이 어렵습니다. 원래 수술로 인한 해부학적 변화가 있고, 원래 담즙 역류가 있고, 원래 주름이 비후되어 있고, 원래 음식물이 조금 남아있기 마련이기 때문입니다. 제가 추천하는 방법은 전 내시경 검사의 잔위 소견을 잘 살펴본 후 이번 내시경의 잔위 소견과 비교하라는 것입니다. 아무리 바뻐도 전 검사 사진을 살펴보는 습관을 가지지 바랍니다. 1분이면 됩니다. 과거 사진 관찰 1분, 금번 내시경 검사 관찰 3분이면 대부분의 잔위암을 진단할 수 있습니다. 물론 사전에 환자에게 잘 설명하여 stomach preparation일 잘 되는 것이 좋습니다. 비급여인 관계로 사용이 쉽지 않지만 mucolytics (엔도나제)를 쓰면 더 좋을 것 같습니다.
[2021-7-4. 삼성서울병원 소화기병심포지엄 실시간 질문]
Total gastrectomy 후에도 정기 내시경 필요한가요?
[2021-7-8. 이준행 답변]
Resection margin이 충분한 상황에서 total gastrectomy를 했을 때 정기적인 추적내시경의 의미는 불명확합니다. 특히 조기위암이었던 경우는 더욱 그러합니다. 2005년 이선영 선생님과 제가 연구하였던 자료를 참고하시기 바랍니다 (EJSO 2005;31:265?269). 그러나 현실에서는 누구나 다 검사하고 있습니다. 학문적 측면과 의사나 환자의 심리적인 측면은 매우 다릅니다.
내시경을 하면서 문합부와 식도 점막이라도 잘 관찰하면 좋지 않을까 생각합니다.
[2021-7-4. 삼성서울병원 소화기병심포지엄 실시간 질문]
Hyperplastic polyp이 cancer로 되어가는 증례를 보여주셨는데, hyperplastic polyp의 f/up 은 주로 어떻게 계획하시고, size가 얼마나커졌을때 절제를 고려하시는지요.
[2021-7-8. 이준행 답변]
과거에는 2cm를 기준으로 하였는데 최근에는 0.5cm를 주장하는 지침도 있습니다. 저는 1cm를 기준으로 하고 있습니다.
![]() [References]
[References]
2) EndoTODAY Subtotal gastrectomy 후 내시경 소견
3) Endoscopic screening for remnant gastric cancer: points to be considered. Park JH, Lee JH. Gut Liver 2007
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.