EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Thursday Endoscopy Conference 20161229]
[Thursday Endoscopy Conference 20161229]
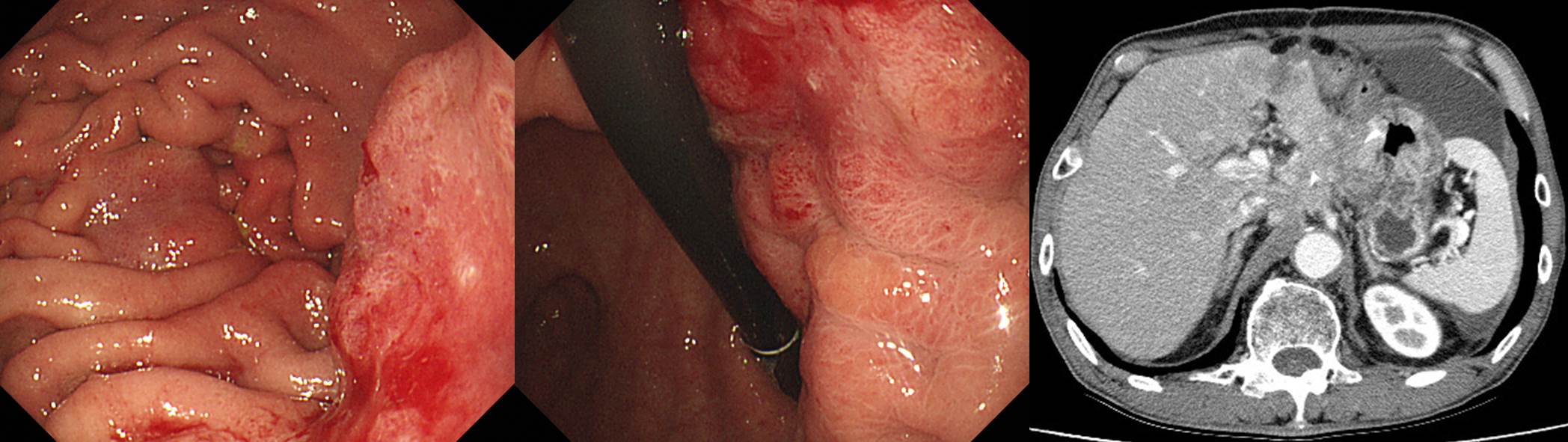
![]() 1. Remnant gastric cancer (recurrent)
1. Remnant gastric cancer (recurrent)
Stomach, subtotal gastrectomy:
Advanced gastric carcinoma
1. Location : lower third, Center at antrum and lesser curvature
2. Gross type : Borrmann type 3
3. Histologic type : tubular adenocarcinoma, poorly differentiated
4. Histologic type by Lauren : diffuse
5. Size : 5x3 cm
6. Depth of invasion : penetrates subserosal connective tissue (pT3)
7. Resection margin: free from carcinoma, safety margin: proximal 3 cm, distal 3 cm
8. Lymph node metastasis : metastasis to 21 out of 35 regional lymph nodes (pN3b) (perinodal extension: present) (21/35 : "1", 0/5; "3", 5/9; "4", 11/13; "4sb", 0/0; "5", 0/0; "6", 1/2; "7", 0/2; "8a", 0/0; "9", 3/3; "11p", 0/0; "12a", 1/1)
9. Lymphatic invasion : present
10. Venous invasion : not identified
11. Perineural invasion : present
12. AJCC stage by 7th edition: T3 N3b
수술 후 항암 방사선치료를 하였습니다. 2년 후 추적 내시경을 시행하였고 조직검사에서 moderately differentiated tubular adenocarcinoma가 나왔습니다. CT에서 locally invasive recurrent cancer였기 때문에 재수술은 불가능한 상태였습니다.
잔위암은 원발암의 종류와 수술 후 잔위암 발견까지의 시간 간격에 따라 아래와 같이 3 가지로 나눕니다. 이 환자는 recurrent type으로 분류하는 것이 무난할 것 같습니다.
* 참고: EndoTODAY 잔위암
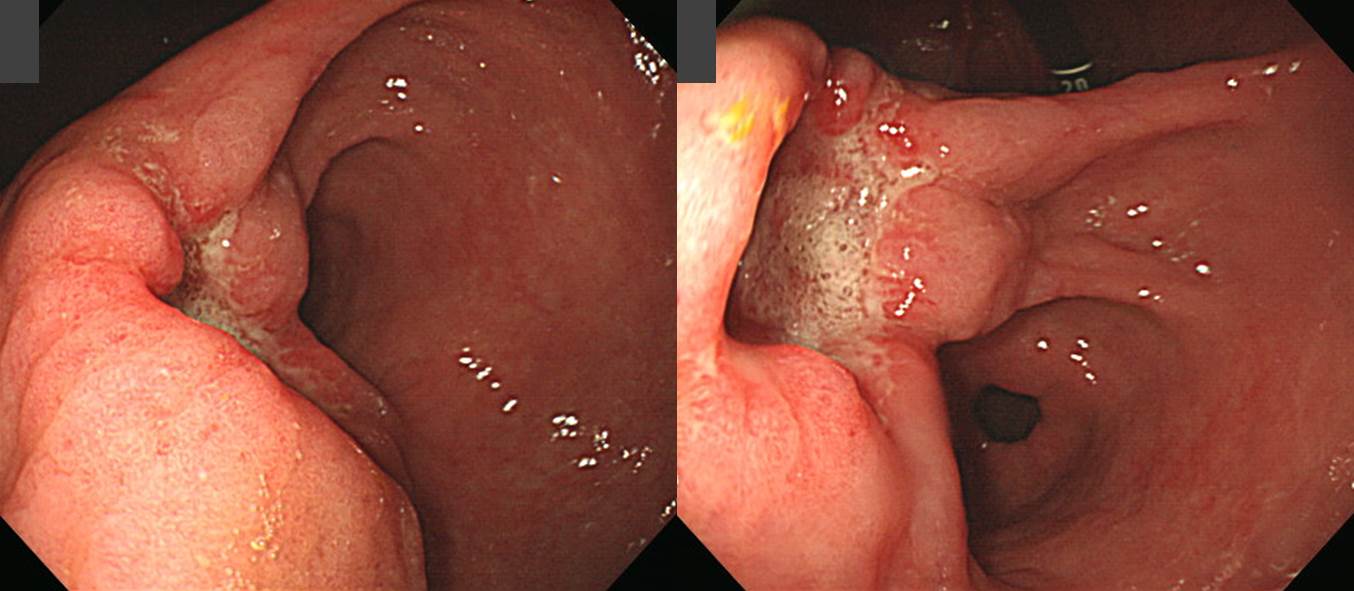
![]() 2. Glomus tumor (mimicking gastric neuroendocrine carcinoma)
2. Glomus tumor (mimicking gastric neuroendocrine carcinoma)
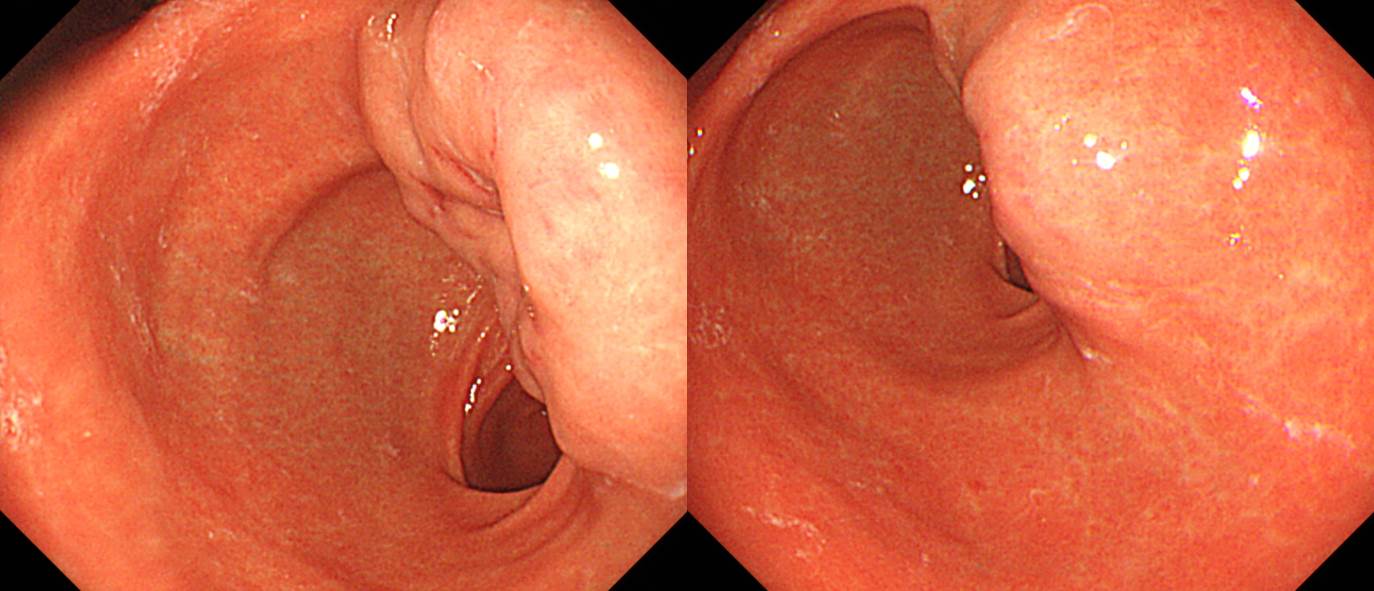
Stomach, subtotal gastrectomy:
Glomus tumor of unknown malignant potential
1) tumor site: antrum and posterior wall
2) tumor size: 3x2 cm
3) mitosis: 0/10 HPFs
4) necrosis: absent
5) cellularity: intermediate
6) cellular atypia: mild
7) invasion into mucosa and serosa
8) infiltrative growth
9) lymphovascular invasion: not identified
10) perineural invasion: present
11) resection margin: negative (safety margin: proximal, 4 cm; distal, 5 cm)
12) no metastasis in 19 regional lymph nodesChromogranin : Negative in tumor cells
Synaptophysin : Positive in tumor cells
Ki-67 : Positive in 5 % of tumor cells
SMA: Diffusely positive in tumor cells
CD 31 : No tumor emboli
D2-40 Podoplanin : No tumor emboli
c-erbB-2(HER2): Negative
Epstein-Barr virus : Negative
병리과에서 처음에는 neuroendocrine carcinoma를 고려하였으나 mitotic index가 너무 낮은 점이 이상하여 여러 추가검사를 한 후 최종적으로 glomus로 진단한 흥미로운 예입니다.
* 참고: EndoTODAY glomus tumor
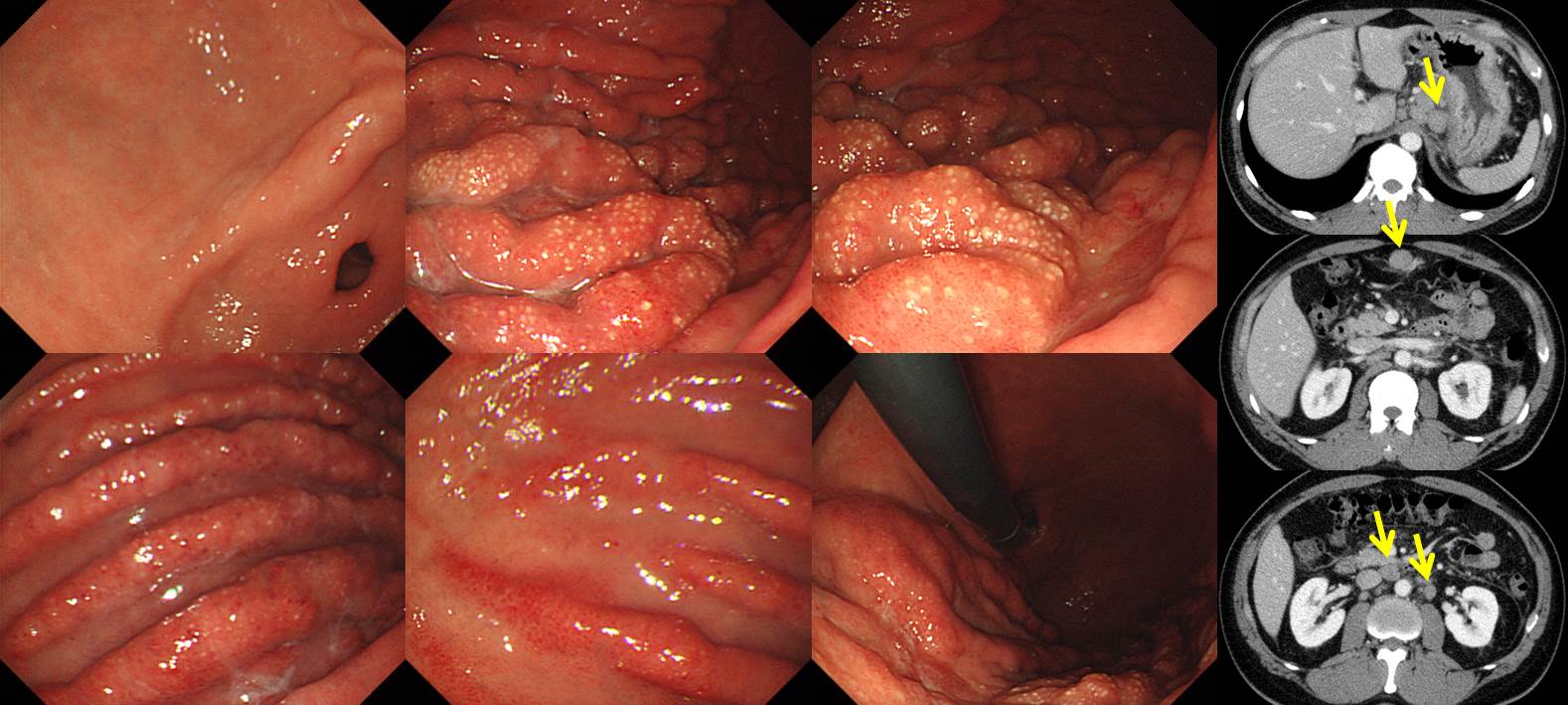
![]() 3. AGC, Borrmann type IV
3. AGC, Borrmann type IV
혈뇨를 주소로 찍은 abdominal CT에서 extensive lymphadenopathy 소견이 보여 lymphoproliferative disorder로 생각하고 의뢰된 내시경입니다. 그런데 의외로 위의 악성질환이었습니다.
임상강사 선생님께서 보만 4형 진행성 위암이라는 impression을 주셨습니다. 저는 (1) fold가 상당히 두꺼워졌으나 탱탱하지 않은 점, (2) air expansion이 잘 되는 점, (3) fold 사이의 거리가 유지되고 있고 골짜기가 제법 깊은 점, (4) 노란색 점처럼 보이는 점막변화는 보만 4형 진행성 위암에서 관찰되기 어려운 점, (5) CT에서 extensive lymphadenopathy가 있었다고 한 점 등을 고려할 때 보만 4형 진행성 위암보다는 lymphoma일 가능성이 높다고 comment 하였습니다. 그러나 막상 조직검사는 poorly differentiated tubular adenocarcinoma로 나왔습니다. 선생으로서 상당히 창피했습니다.^^ 보만 4형 진행성 위암에 관심을 갖고 20년 이상 진료,연구에 힘쓴 내시경 전문 교수도 진단하기 어려운 병이 바로 보만 4형 진행성 위암입니다. 그만큼 어렵습니다.
![]() [References]
[References]
1) SMC Endoscopy Unit 삼성서울병원 내시경실
2) SMC Monday GI conference 삼성서울병원 일원내시경교실 월요점심소화기집담회
3) SMC Thursday endoscopy conference 삼성서울병원 일원내시경교실 목요점심내시경집담회
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.