EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [위암 103 - Amphicrine tumor]
[위암 103 - Amphicrine tumor]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
![]() 1. Amphicrine tumor란 무엇인가?
1. Amphicrine tumor란 무엇인가?
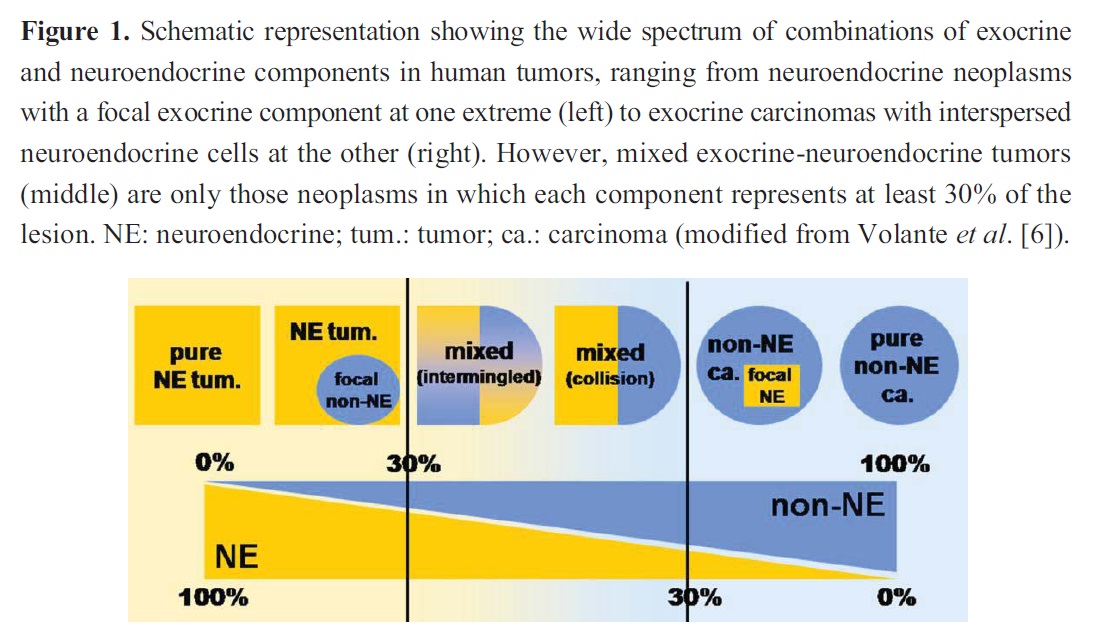
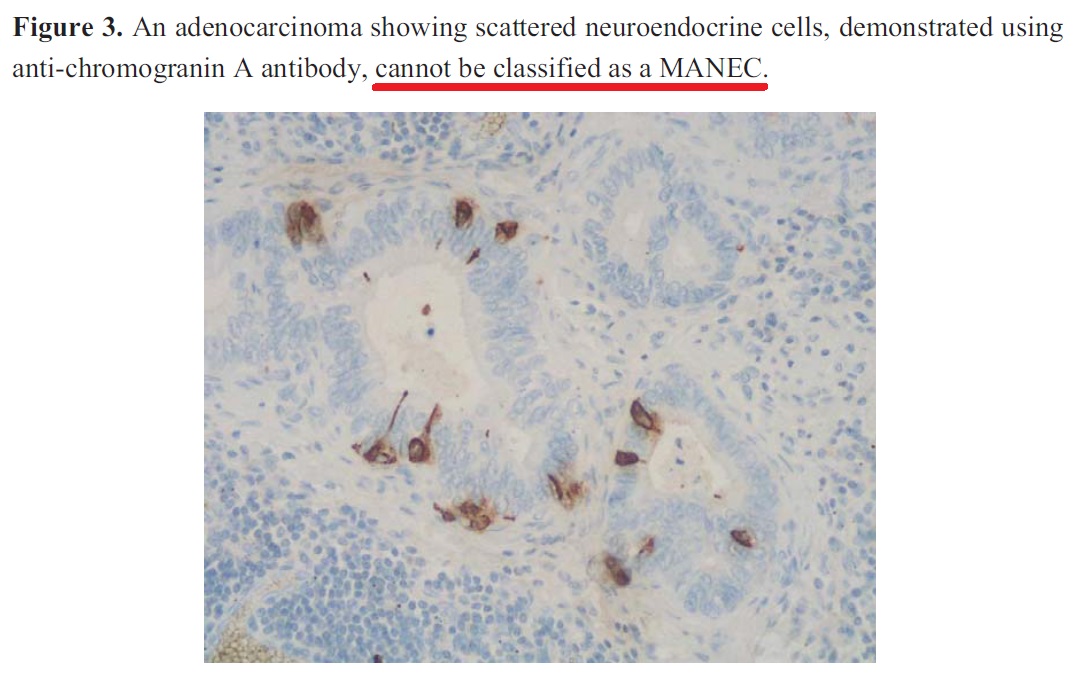
간혹 위선암에 신경내분비세포(neuroendocrine cell)이 산재된 경우가 있다는 것은 잘 알려진 사실입니다. 그러나 endocrine tumor와 non-endocrine tumor가 함께 섞인 경우에 대해서는 약간의 혼선이 있습니다. Amphicrine tumor는 한 세포에서 dual epithelial and neuroendocrine differentiation이 일어난 종양입니다. 질병 자체는 aggressive합니다. 반면 composite tumor의 예후는 좋습니다. .
2005년 Fujiyoshi는 mixed endocrine and non-endocrine epithelial tumor를 아래와 같이 분류하였고 amphicrine tumor는 그 중 하나입니다.
@ Images in Pathology - Amphicrine Gastric Carcinoma (Arch Pathol Lab Med. 2001)
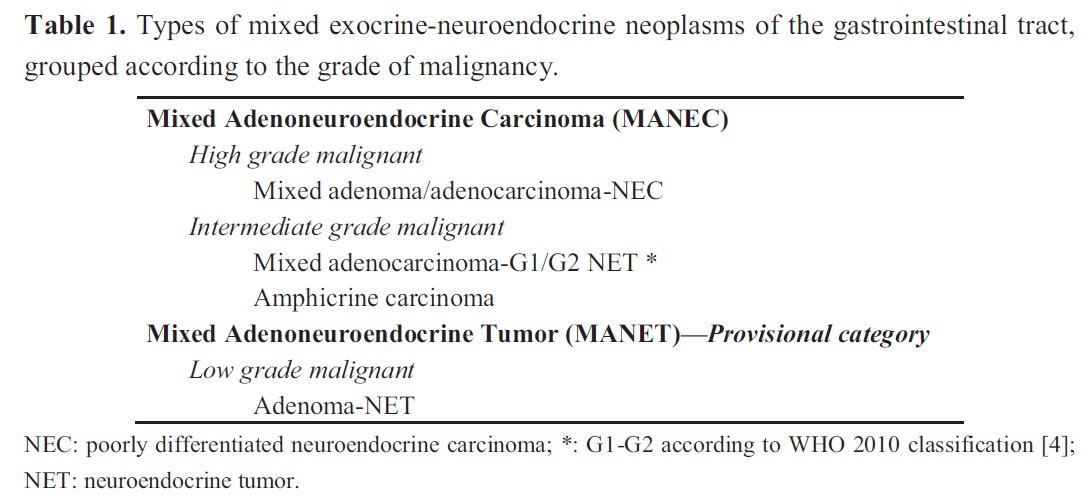
최근에는 Mixed Adenoneuroendocrine Carcinomas (MANECs)라는 이름으로 통일되고 있는 것 같습니다 (Cancers 2012;4:11-30).
胃 amphicrine tumor와 비슷한 것이 appendix의 goblet cell carcinoid입니다. Goblet cell carcinoid tumors of the appendix: An overview"라는 2010년 종설을 소개합니다. 요약의 일부를 옮깁니다. Appendix의 이야기인데 위도 비슷합니다.
The tumor is thought to arise from pluripotent intestinal epithelial crypt-base stem cells by dual neuroendocrine and mucinous differentiation. GCCs present in the fifth to sixth decade and show no definite sex predominance. The most common clinical presentation is acute appendicitis, followed by abdominal pain and a mass. Fifty percent of the female patients present with ovarian metastases. The histologic hallmark of this entity is the presence of clusters of goblet cells in the lamina propria or submucosa stain for various neuroendocrine markers, though the intensity is often patchy. Atypia is usually minimal, but carcinomatous growth patterns may be seen. These may be of signet ring cell type or poorly differentiated adenocarcinoma. Recently molecular studies have shown these tumors to lack the signatures of adenocarcinoma but they have some changes similar to that of ileal carcinoids (allelic loss of chromosome 11q, 16q and 18q). The natural history of GCC is intermediate between carcinoids and adenocarcinomas of the appendix. The 5-year overall survival is 76%. The most important prognostic factor is the stage of disease. Appendectomy and right hemicolectomy are the main modalities of treatment, followed by adjuvant chemotherapy in select cases.
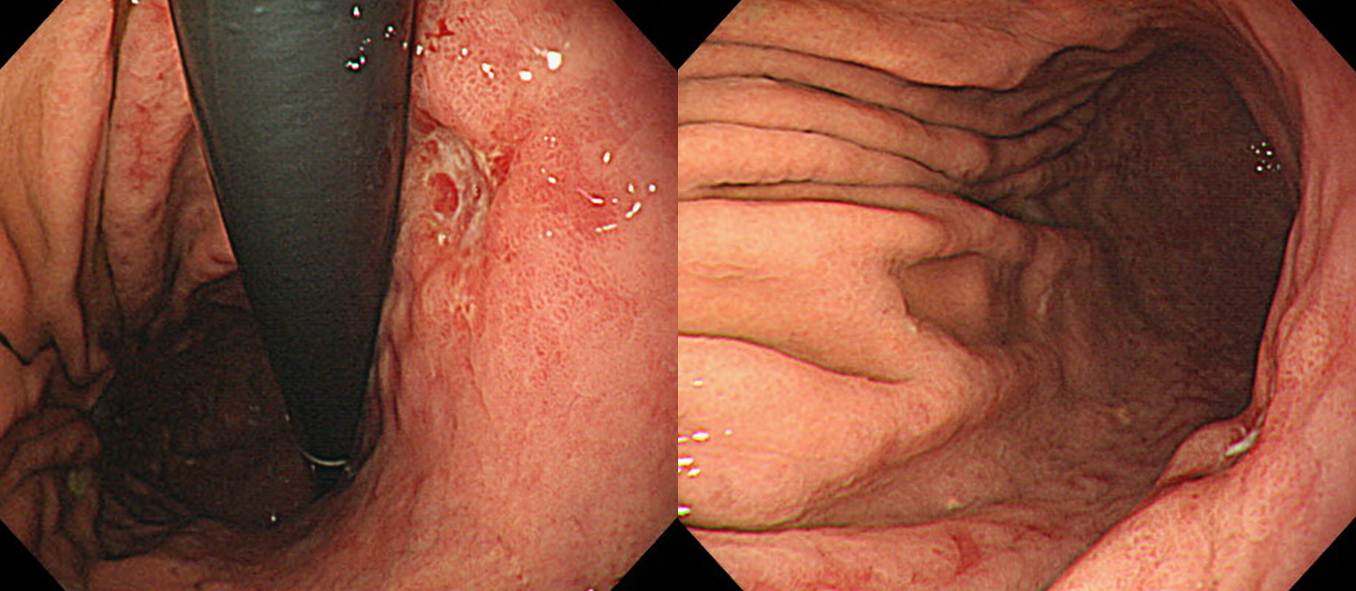
![]() 2. 수술로 치료한 증례
2. 수술로 치료한 증례
Mixed exo- and endocrine carcinoma (G3) (Specify : amphicrine carcinoma)
1. Name of Procedure: Subtotal gastrectomy
2. Site of Tumor: Stomach (Body and posterior wall)
3. Diagnosis: Mixed exo-and endoccrine carcinoma (G3) (specify: Amphicrine carcinoma)
4. WHO classification(2010): Mixed exo- and endocrine carcinoma (Specify : amphicrine)
5. Multiplicity: Single
6. Size: 2.4x1.7 cm
7. Extent: Proper Muscle (pT2)
8. Grading: Mitotic Count(/10HPF): > 20 , Ki-67 labeling index: G3>20%
9. Immunohistochemical Stains: Synaptophysin: Positive, Chromogranin A: Positive
10. Lymphovascular invasion: Present
11. Perineural invasion: Present
12. Lymph node metastasis: Number of positive nodes/Total number of nodes(0/30)
13. Resection Margins: Negative
![]() 3. 내시경으로 치료한 증례
3. 내시경으로 치료한 증례
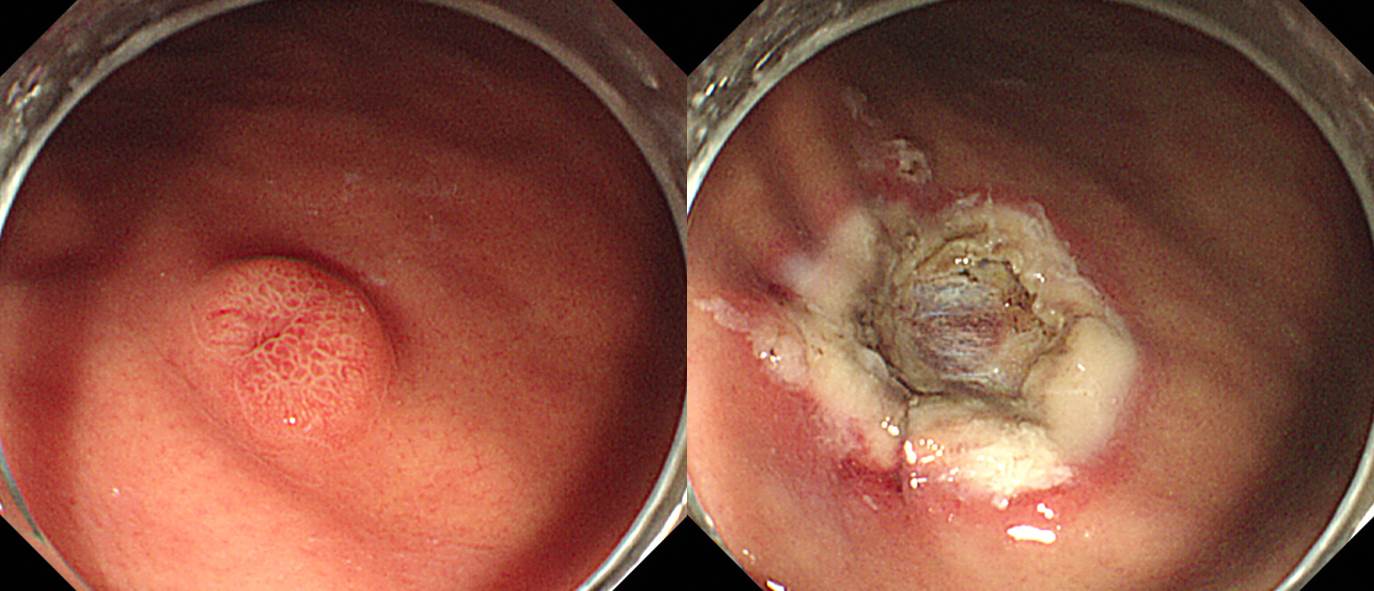
Stomach, mid body, anterior wall, endoscopic mucosal resection:
Adenocarcinoid (amphicrine tumor)
1. Name of Procedure: EMR
2. Site of Tumor: Stomach (Body)
3. Diagnosis: Mixed exo- and endocrine tumor
4. WHO classification(2010): Mixed exo- and endocrine carcinoma, grade 2 (specify: adenocarcinoid)
5. Multiplicity: Single
6. Size: 0.4x0.4 cm
7. Extent: Mucosa and submucosa
8. Grading: Mitotic count(/10 HPF): 0-1, Ki-67 labeling index: G2 3-20% (Positive in about 5% of tumor cells)
9. Immunohistochemical Stains: a. Synaptophysin: Positive, b. Chromogranin A: Positive
10. Lymphovascular invasion: Not identified
11. Perineural invasion: Not identified
12. Lymph node metastasis: not evaluated
13. Resection Margins: Negative, safety margin: 50㎛ (deep)
![]() [Cases]
[Cases]
위암 604
Stomach, subtotal gastrectomy: Advanced gastric carcinoma
1. Location : lower third, Center at antrum and lesser curvature
2. Gross type : Borrmann type 2
3. Histologic type : tubular adenocarcinoma, moderately differentiated with focal neuroendocrine differentiation
4. Histologic type by Lauren : intestinal
5. Size : 3.5x4.5 cm
6. Depth of invasion : penetrates subserosal connective tissue (pT3)
7. Resection margin: free from carcinoma, safety margin: proximal 4.5 cm, distal 4 cm
8. Lymph node metastasis : metastasis to 5 out of 52 regional lymph nodes (pN2) (perinodal extension: present) (5/52: "3", 2/17; "4", 1/14; "5", 1/2; "6", 0/4; "7", 0/2; "8a", 0/2; "9", 0/1; "11p", 0/2; "12a", 1/3; "4sb", 0/4; "1", 0/0; "4d", 0/1)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Associated findings : ulceration
13. Peritoneal cytology : negative
14. AJCC stage by 7th edition: pT3 N2
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.