EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [The 18th Recent Update of Neurogastroenterology & Motility Symposium - 연세대강남세브란스 기능성질환 심포지엄]
[The 18th Recent Update of Neurogastroenterology & Motility Symposium - 연세대강남세브란스 기능성질환 심포지엄]
주제: New & evolving therapies for managing FGIDs.
시간: 2017년 6월 17일 오후 1시 30분
장소: 강남세브란스병원 본관 2동 3층 중강당 (신청서)

이준성, Justin Wu, Hiroto Miwa, 박효진, 윤영훈 교수님과 함께
윤영훈, Justin Wu, 박효진, 박정호 교수님과 함께

![]() 1. New & Evolving drugs (좌장: 박효진, 이준행)
1. New & Evolving drugs (좌장: 박효진, 이준행)
1) Gastroesophageal Reflux Disease. Justin Wu (HK, China)
[Abstract]Gastroesophageal reflux disease is on the rise in Asia. Risk factors of GERD are evolving in Asia: Westernized diet, obesity and metabolic syndrome are also contributing factors to the rising prevalence of GERD in Asia. Asian GERD patients share similar pathophysiology with the Western counterparts, with transient lower esophageal sphincter relaxation as the single most important mechanism. Lower prevalence of hiatus hernia and lesser impact of obesity may account for the milder severity of erosive esophagitis and other GERD complications in Asia.
GERD is primarily a clinical symptom-based diagnosis and there is a lack of sensitive confirmatory investigation. Despite the low diagnostic yield, upper endoscopy and Helicobacter pylori eradication are recommended in the population with high prevalence of H. pylori by the WGO Guidelines because the symptoms of GERD and H. pylori related diseases may be difficult to distinguish. The current guidelines also recommend extended course of proton pump inhibitor therapy up to 8 weeks to ascertain the symptom-based diagnosis of GERD.
Despite the less severe disease profile in terms of complications, Asian GERD patients have lower symptom response rate to proton pump inhibitor. Patients with poor response to PPI may benefit from adjunct alginate-antacid, modified-release PPI or double-dose PPI. Esophageal manometry and reflux testing (pH alone or combined pH-impedance) help define the esophageal acid exposure and symptom-reflux association. The latest international consensus suggests ambulatory off-PPI pH monitoring as the primary investigation of choice for PPI non-responders. Combined pH-impedance monitoring is indicated if there is severe esophagitis and high suspicion of persistent acid or non-acid reflux. Laparoscopic fundoplication remains the operative treatment of choice with comparable long-term efficacy with PPI if there is objective evidence of reflux as confirmed by reflux testing. Emerging therapies such as LES augmentation therapy (implanted magnetic device, electrical stimulation and radiofrequency energy) have been marketed but their role in the management algorithm is yet to be determined.
Porto Consensus (Neurogastroenterol Motil 2017) - LA A, B에서는 off PPI 검사를 시행하고, LA C, D에서는 on double dose PPI를 시행할 것을 권유
Antidepressant: Functional hearburn에서 SSRA가 TCA보다 효과적이다 (Weijenborg CGH 2015).
Produg인 PPI와 달린 P-CAP은 chemical conversion이 없이 작용하므로 action onset이 빠르다.
Prokinetics and reflux inhibitors are not effective for PPI-resistent symptoms.
[이준행 질문] "You mentioned two types of novel laparoscopic LES augmentation, and one of them is implantable electrical stimulation, Endostim. Could you tell me a little bit about Endostim, its mode of action, clinical efficacy until now."
[Justin Wu 선생님 답변] Sham trial에서 효과가 입증되었습니다. Hiatal hernia가 있는 환자에서는 효과가 없는 것 같습니다. 장기 자료는 부족하므로 long term study가 필요할 것 같습니다.
심장 pacemaker와 비슷한 방식인데 약 10년 정도 battery time을 가진다고 합니다.
2) Visceral hyperalgesia. Jung Ho Park (Sungkyunkwan Univ)
Mechanisms of nociceptor sensitisation (including to acid): (1) decreased transduction threshold by phosphorylation of ion channels (mediated by intracellular activation of protein kinases in response to G-protein-coupled release of cAMP); (2) upregulation of ion channel expression?for example, TRPV1 in response to trophins?for example, to nerve growth factor (NGF) with retrograde transport from the cell body to nerve terminals; (3) bidirectional neuroimmune interactions, especially in respect of neuronal substance-P (SP) release acting on mast cells to release NGF. GPCR. G-protein-coupled receptor; 5-HT, 5-hydroxytryptamine; NK1, neurokinin 1; PAR, protease-acivated receptor; PKA, protein kinase A; PKC, protein kinase C; TrkA, tyrosine kinase receptor A.
Molecular mechanisms of central sensitisation. Incoming action potentials lead to release of various neurotransmitters and neuromodulators that act via G-protein-coupled receptors (GPCRs) (prostaglandins (PGs), 5- hydroxytryptamine (5-HT)), neurokinin recptors (substance-P) and tyrosine kinase (brain-derived neurotrophic factor (BDNF)) as well as ligand-gated ion channels (glutamate). Subsequent intracellular messaging systems (predominantly via increased intracellular calcium and activation of protein kinases A and C lead to phosphorylation of N-methyl-D- aspartate (NMDA) receptors with a reduction in voltage-dependent magnesium block. This potentiates its responsiveness to glutamate and leads to central sensitisation in the neuron concerned and those adjacent to it (secondary hyperalgesia). AMPA, a-amino-5-hydroxy-3-methyl-4-isoxazole proprionic acid; PKA, protein kinase A; PKC, protein kinase C.
Mesalazine treatment for 2 weeks significantly reduced the total mucosal immune cell counts as compared to placebo (P = 0.0082). No significant effects were observed for T cells, B cells or macrophages; however, mast cell counts (Figure 3) were significantly reduced by mesalazine treatment as compared with placebo. Mesalazine treatment had a significant effect on general well-being (P = 0.038) and patients in the mesalazine group rated the treat- ment better than did patients randomized to placebo (P = 0.035). In contrast, there was no significant effect of mesalazine on abdominal pain (P = 0.084), bloating (P = 0.177) or stool frequency. Mesalazine is an effective and safe approach to reduce mast cell infiltration and may improve general well-being in patients with IBS
Kappa Opioid receptor agonist, asimadoline and fedotozine decrease visceral hypersensitivity and The fundamental mechanism of action is an inhibition of the excitability of visceral afferent nerve terminals in the gut wall, causing a reduction of action potential firing and neurotransmitter release from those sensory nerves

Gut microbiota in uences the bidirectional communication between the enteric nervous system and the central nervous system, modulating gut development and several physiological functions, including intestinal motility, sensitivity, secretion and immunity. In irritable bowel syndrome (IBS), the altered composition and/or activity of microbiota may induce a disruption of this communication leading to activation of immune system and production of pro- in ammatory cytokines, production of microbial metabolites as short-chain fatty acids (SCFAs) that are toxic at high concentration, activation of hypothalamic-pituitary- adrenal (HPA) axis with increase of cortisol that feeds back to the pituitary, hypothalamus (HYP), amygdala (AMG), hippocampus (HIPP) and prefrontal cortex to shut off the HPA axis and increase of corticotropin releasing factor (CRF). These effects lead to alterations of intestinal motility and sensation, disruption of epithelial barrier and impaired production of neurotransmitters with an increased response to stressful events. On turn, stress may provoke systemic pro-in ammatory cytokines production that activates the HPA axis that signals to both enteric nervous system and the central nervous system and may alter microbiota composition.

[질문] There are so many new and fancy drugs, but no comparison studies between them. I don't know which one will be coming in to the market first. Which one is the most promising one?
[박정호 교수님 답변] Asimadoline의 임상연구가 끝났기 때문에 아마도 가장 promising 한 것으로 생각합니다.
3) Recent update of pathogenesis of functional dyspepsia. Hiroto Miwa (Hyogo, Japan)
소개의 말: It's great honor to introduce the next speaker professor Hiroto Miwa. After graduating Kagoshima University, he has been working as one of the best researchers in the field of functional gastrointestinal disorders. He is now the professor of Medicine, Hyogo College of Medicine and has been serving as the Vice president of Japanese Society of Gastroenterology. His topic today is funtional dyspepsia.
[Abstract] Dyspepsia is one of most common symptom and approximately 10% of general population has chronic dyspeptic symptoms without apparent organic causes, which is functional dyspepsia. Although FD is one of most important functional GI disorders, its pathogenesis is highly complicated. Possible pathogenic factors for FD includes, acid, H.pylori infection, motility disorders, gastric hypersensitivity and so on. Among those, it is well recognized that motility disorders and gastric hypersensitivity are the factors that directly induce GI symptom manifestation. However, what brings these physiological impairment has remained to be addressed.
Recently the importance of duodenum as a pathogenic center of functional dyspepsia has been gradually and widely recognized. Stimulus or inflammation to duodenum may bring the physiological impairment of the stomach. In fact, early reports demonstrated that intraduodenal application of lipid and acid alter visceromotor function of the stomach. These data suggest that stimulation to duodenum causes motility and sensory dysfunction of the stomach which result in generation of dyspeptic symptoms even in normal subjects. However, unlike the normal subjects, FD patients have dyspeptic symptoms chronically. What is the difference between duodenum of FD patients and that of normal subjects?
I assume duodenum of FD patients is primed, in other words, the duodenum of FD patients is ready to be activated. Two factors, which is presence of low grade inflammation and increased mucosal permeability may be responsible for this phenomenon. There are many reports describing low grade inflammation in FD patients, and the consensus seems to be made recently that both mast cells and eosinophils were increased especially in the second portion of the duodenum. One of the factors that brings the infiltration of eosinophils or mast cells in duodenal mucosa may be severe GI infection, which is known as “post-infectious FD”. Low grade inflammation must be a remaining of severe inflammation, however other clear causes for low grade infiltration is not known. The increased permeability of duodenal mucosa in FD patients was first reported recently by Belgium group, which was proven using biopsy specimens from duodenum mucosa and Ussing chamber. Regarding the factors that makes mucosal permeability increased in duodenal mucosa, much is not known. However, there is a recent report demonstrating that small intestinal permeability is increased in psychological stress condition, which is inhibited by pre-administration of mast cell stabilizer, suggesting that the psychological stress increases intestinal permeability by a mast cell-dependent mechanism possibly through CRH axis.
Very recently, the data have been presented suggesting the important role of bile in pathogenesis of functional dyspepsia. The researchers have shown that the bile was associated with increased mucosal permeability and especially secondary bile is correlated with the permeability in FD patients. Furthermore, they showed that one of several bile salt receptor in duodenum is increase in FD patients. It is a future matter of debate that “what’s happening in duodenum of FD patients?” Luminal factors or luminal antigens must play some roles in duodenum, which include acid, bile, nutrients including lipid, microbiome and product of microbiome. It would be possible that interaction of such factors with duodenum may explain pathogenesis of functional dyspepsia.
[이준행 질문] You emphasized the role of low grade inflammation and increased mucosal permeability of the duodenum in the pathogenesis of FD symptom development. I wonder what is the role of Helicobacter pylori in the development of chronic low grade inflammation or permeability change of the duodenal mucosa. After eradication treatment, could you tell me what kind of histological or functional changes happen?
[Miwa 선생님 답변] 헬리코박터 양성 FD 환자와 음성 FD 환자 사이에서 십이지장 염증이나 permeability는 차이가 없습니다. 헬리코박터 제균치료가 크게 효과적이지 않은 것은 이것 때문인 것으로 생각합니다.
[이동호 교수님 질문] 항염증제나 probiotics의 효과는 어떠합니까?
[Miwa 선생님 답변] Rebamipide는 여러 임상연구에서 효과가 없었습니다. Probiotics에 대해서는 희망이 있지만 자료가 부족합니다. 연구가 필요합니다.
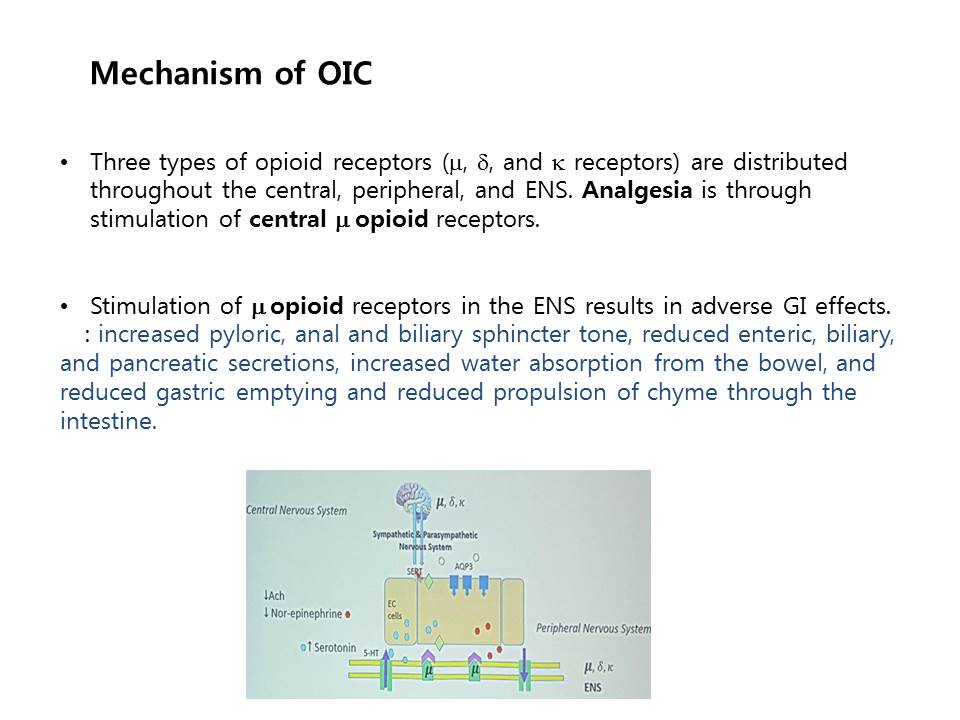
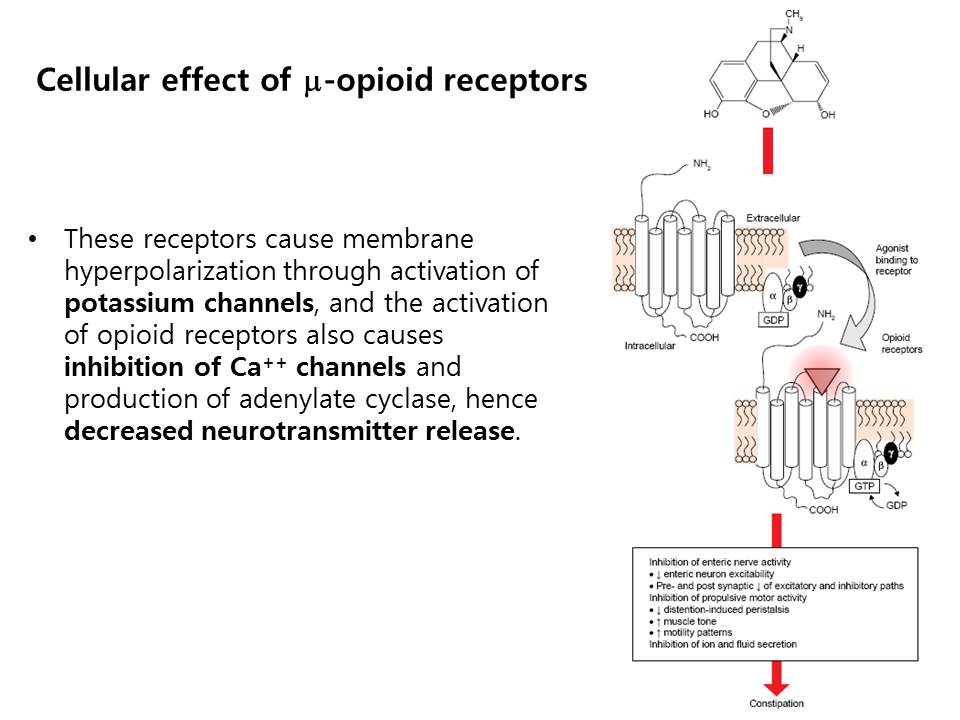
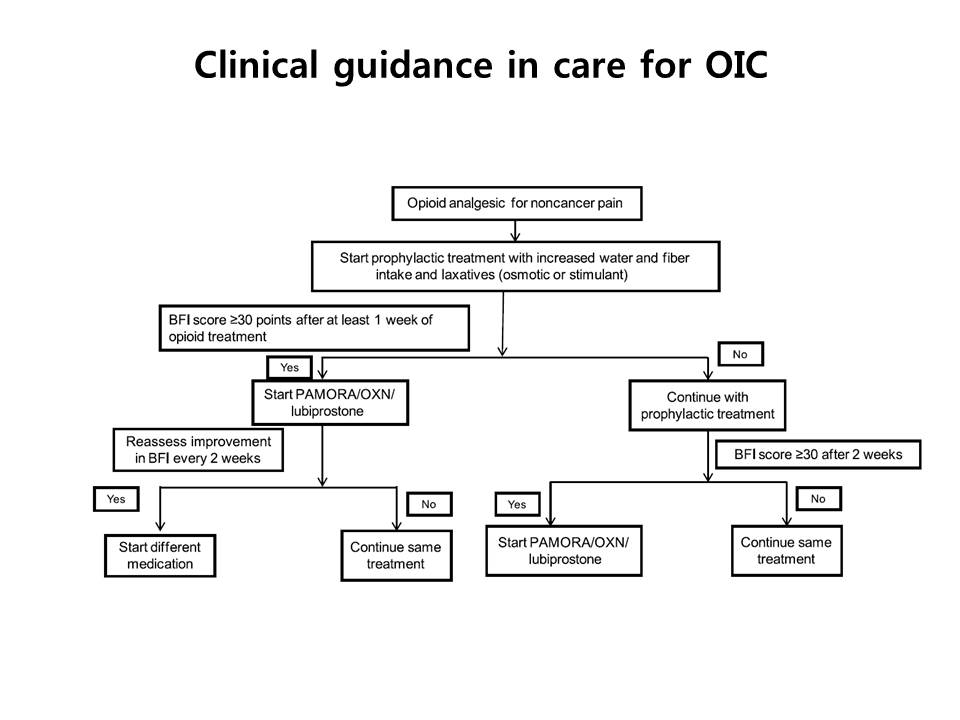
4) Opoid-induced constipation (OIC). Hyojin Park (Yonsei Univ)
소개의 말: The next speaker is Hyojin Park, the president of this prestigious symposium. He is the professor of Internal Medicine, Yonsei University College of Medicine, and the General director of Gangnam Severance Cancer Hospital. As you know, he is the current President of Asian Neurogastroenterology and Motility Association, ANMA. His topic today is opoid-induced constipation (OIC).
![]() 2. New & Evolving techniques (좌장: 최명규, 정훈용)
2. New & Evolving techniques (좌장: 최명규, 정훈용)
1) Endoscopic treatment for esophageal motor disorders. Young Hoon Youn (Yonsei Univ)
(1)Heller myotomy: Open보다는 laparoscopic이 좋고, thoracoscopic보다 laparoscopic이 좋고, full 보다 partial이 좋습니다.
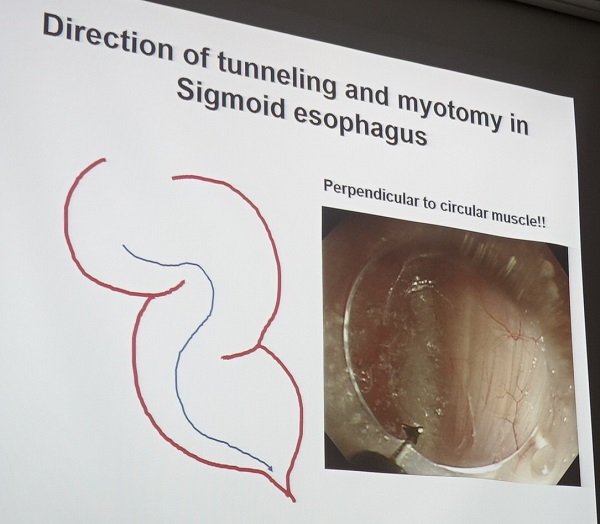
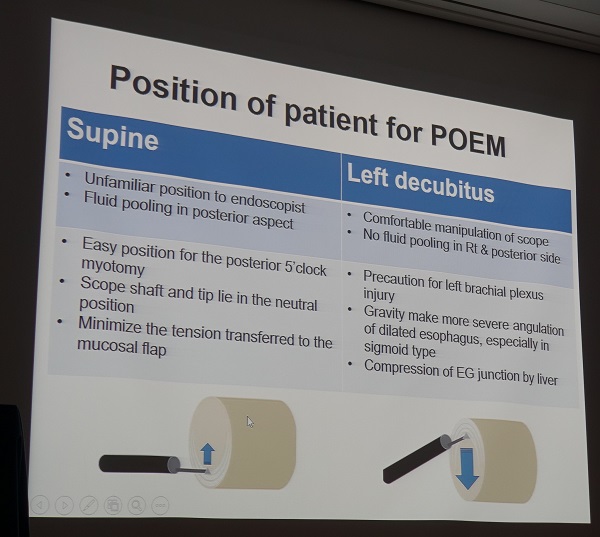
(2) POEM
- ESD와 달리 general anesthesia, positive pressure ventilation, CO2 insufflator, IV antibiotics가 필요합니다.
- 가능하면 deep tunneling을 해야 합니다. (1) 어짜피 myotomy를 할 것이므로 일부 손상이 되어도 상관이 없습니다. (2) Muscle이 두꺼워서 천공이 잘 발생하지 않습니다. (3) Mucosal flap을 보호하는 것이 훨씬 더 중요하기 때문입니다.(4) 방향을 잃지 않기 위하여 muscle fiber를 보고 직각으로 방향을 잡아야 하기 때문입니다.
- POEM 후 peristalsis가 돌아오는 환자가 있습니다. Type III, 증상 기간이 1년 이하로 짧았을 때는 POEM 후 peristalsis가 돌아오는 경우가 많습니다. (정훈용 교수님 comment: Type III에서 호전되어 보이는 것은 POEM에 의하여 과장된 contractility가 없어지므로 거품이 걷히면서 원래 있던 peristalsis가 호전되는 것처럼 보이는 것일 수 있습니다.)
- Non-achalasia에서 POEM을 할 경우에는 환자 selection에 훨씬 주의해야 합니다. Diffuse esophageal spasm의 manometry 소견은 GERD에서도 일시적으로 보일 수 있으므로 진단에 주의해야 합니다. Non-achalasia에서 POEM을 하면 LES pressure가 떨어져 산역류가 증가하여 오히려 GERD 증상이 악화될 수 있습니다.
- Spastic motility disease에서 ice water를 사용하여 contraction을 유발하면 치료범위 결정에 도움이 될 수 있습니다.
[정훈용 좌장님 comment] Dysphagia로 오는 non-achalasia spastic disease 환자에서 circular muscle contraction이 주된 증상의 원인입니다. IRP가 높다고 POEM을 하면 누워서 자지 못하는 경우가 발생할 수 있으므로 우선 PPI를 써서 증상 호전 여부를 보는 것이 좋겠습니다.
[이준행 질문] Non-achalasia spastic disorder에서 body peristalsis를 하고 LES myotomy를 하지 않으면 좋을 것 같은데... body와 LES의 연결부분을 어떻게 구분할 수 있습니까?
[윤영훈 교수님 답변] Incisor로부터의 거리로 판단할 수 밖에 없으며, 간혹 oblique한 muscle fiber가 보이면 LES에 가까이 온 것으로 판단할 수 있습니다.
* 참고: EndoTODAY 식도이완불능증
2) Fecal microbiota transplantation for functional GI disorders. Jae Joon Park (Yonsei Univ)
IBS 환자에서 장내세균총의 변화가 있습니다. Restoration of normal intestinal homeostasis via FMT may result in symptomatic improvement.
1958년 FMT가 최초로 보고되었습니다. (Ben Eiseman 박사)
2016년 제4차 신의료기술평가에서 안전성,유효성이 있는 의료기술로 인정되었으므로 현재 '인정비급여'로 시행할 수 있습니다. 적응증은 '재발성 또는 기존 항생제 치료에 반응하지 않는 Clostridium difficile 감염 환자' 입니다. 비용은 70-80만원 수준.
강남세브란스 병원에서는 stool을 진단검사의학과에서 preparation을 하고 소화기내과에서는 주입만 하는 방식이 시도되고 있습니다.
PDF 2.6M
[최명규 교수님 comment] 성모병원에는 20예가 조금 넘는 증례가 있으며, fresh stool만으로 신속히 시술하기 어려워 frozen stool로 시술할 수 있는 시스템을 만들고 있습니다. Stool bank를 설립 중입니다. 이 분야에 대한 시스템 구축과 질관리가 필요합니다.
* 참고: EndoTODAY Fecal microbiota transplantation
![]() [References]
[References]
20141011 강남세브란스병원 single topic symposium 2014 (Stricture after ESD)
20151017 강남세브란스병원 motility symposium 2015 (Achalasia)
20151017 강남세브란스 single topic symposium 2015 (대장 ESD)
20161117 강남세브란스 single topic symposium 2016 (위 ESD)
20170617 강남세브란스 motility symposium 2017 (New and evolving therapies)
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.