 EndoTODAY ГЛНУАц БГНЧ
EndoTODAY ГЛНУАц БГНЧ
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [РЯПјГЛНУАцБГНЧ ИёПфСЁНЩС§ДуШИ 2016-5-19]
[РЯПјГЛНУАцБГНЧ ИёПфСЁНЩС§ДуШИ 2016-5-19]
![]() 1. ЙЋСѕЛѓ НФЕЕ ФЕ№ДйСѕ
1. ЙЋСѕЛѓ НФЕЕ ФЕ№ДйСѕ
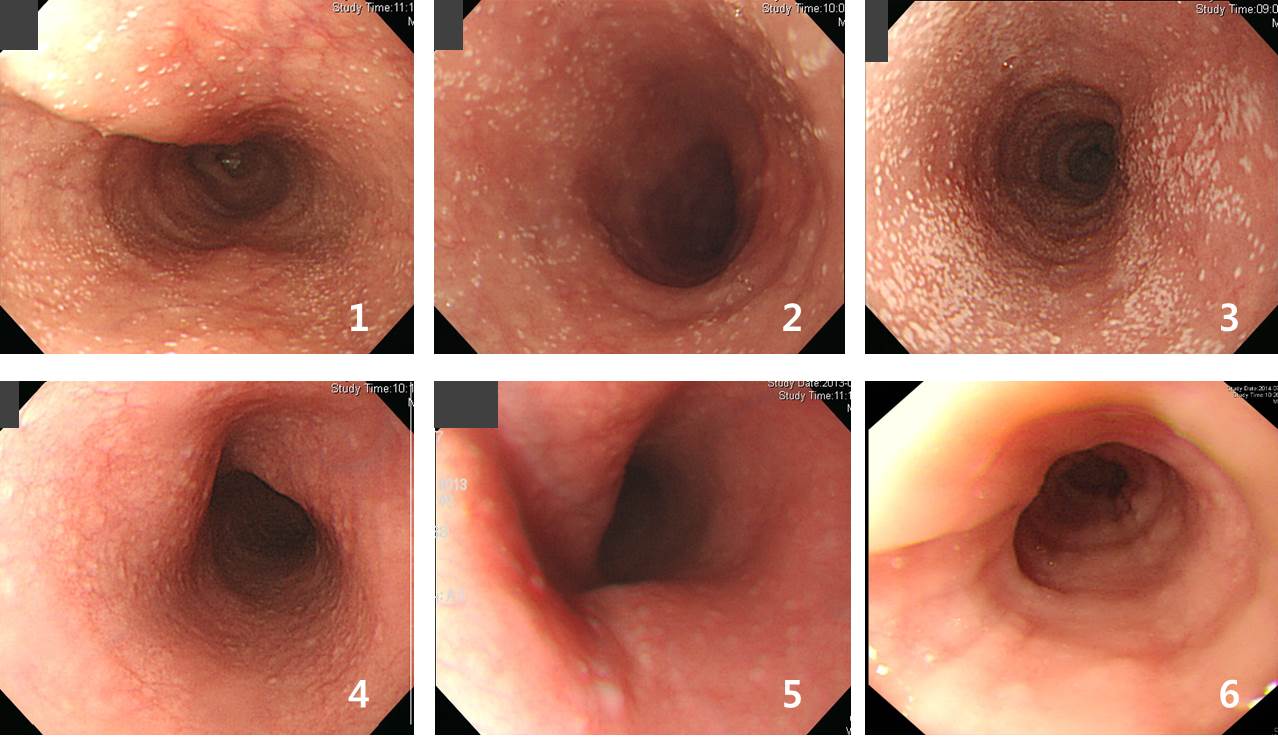 1 Гт АЃАнРИЗЮ ИХГт ГЛНУАц АЫЛчИІ ЙоОвНРДЯДй.
1 Гт АЃАнРИЗЮ ИХГт ГЛНУАц АЫЛчИІ ЙоОвНРДЯДй.
АЧСјПЁМ ИХГт CandidasisАЁ ГЊПЭ РЧЗкЕЧОю ИХГт fluconazoleРЛ ЕхЗШДйАэ ЧеДЯДй. БзЗБЕЅ Ию Гт ПЌМг ГЊПРДйАЁ ОюДР ЧиКЮХЭ ГЊПРСі ОЪОвНРДЯДй. ОюТюЕШ ПЕЙЎРЮСі ОЫ Мі ОјНРДЯДй. ИщПЊРњЧЯШЏРкАЁ ОЦДб АцПь ЙЋСѕЛѓНФЕЕФЕЕ№ДйСѕРК СпПфЧб СњКДРИЗЮ СјЧрЧЯСі ОЪДТ self-limited diseaseАЁ КаИэЧб АЭ ААНРДЯДй. АЫЛчЧЯАэ АсАњЦЧЕЖРЛ ЧЯДТ РЧЛчАЁ Рп МГИэЧЯАэ РЧЗкЧЯСі ОЪРИИщ ФЁЗсЧЯСі ОЪАэ АцАњАќТћРЛ Чв Мі РжНРДЯДй. БзЗЏГЊ РЯДм ШЏРкИІ РЧЗкЙоРИИщ ФЁЗсЧЯСі ОЪБтДТ ОюЗЦНРДЯДй.
АќЗУЧЯПЉ УжБй АЧБЙДыЧаБГ КДПјПЁМ ЙЋСѕЛѓ НФЕЕ ФЕ№ДйСѕРЧ РкПЌ АцАњПЁ ДыЧб ГэЙЎРЛ ЙпЧЅЧб Йй РжНРДЯДй (Lee SP. Scand J Gastroenterol 2015). ФЁЗсАЁ ЧЪПфЧЯСі ОЪДйДТ АсЗаРдДЯДй.
MATERIALS AND METHODS: A total of 49,497 subjects who underwent a health inspection that included upper endoscopy were enrolled. We retrospectively reviewed the subject's self-reporting questionnaires, medical records and endoscopic findings. We considered "long-term" follow-up to be >6 months with at least one more follow-up endoscopy.
RESULTS: One hundred and seventy (0.4%) subjects were endoscopically diagnosed as esophageal candidiasis and 141 subjects were AEC. Multivariate analysisrevealed that old age (ЁУ60 years) was an independent risk factor for AEC (OR, 1.862, p = 0.005). The number of subjects with long-term follow-up was 79 (195.3 person-years). Among these, AEC of 64 subjects (81.0%) had disappeared on the follow-up endoscopy and was not recurrent. The other 15 subjects had AEC diagnosed more than once on the follow-up endoscopy, and 5 of them were spontaneously healed during the follow-up period. The remaining 10 subjects whose candidiasis was sustained up to the last endoscopy did not complain of symptoms during the follow-up period, and their endoscopic findings did not worsen.
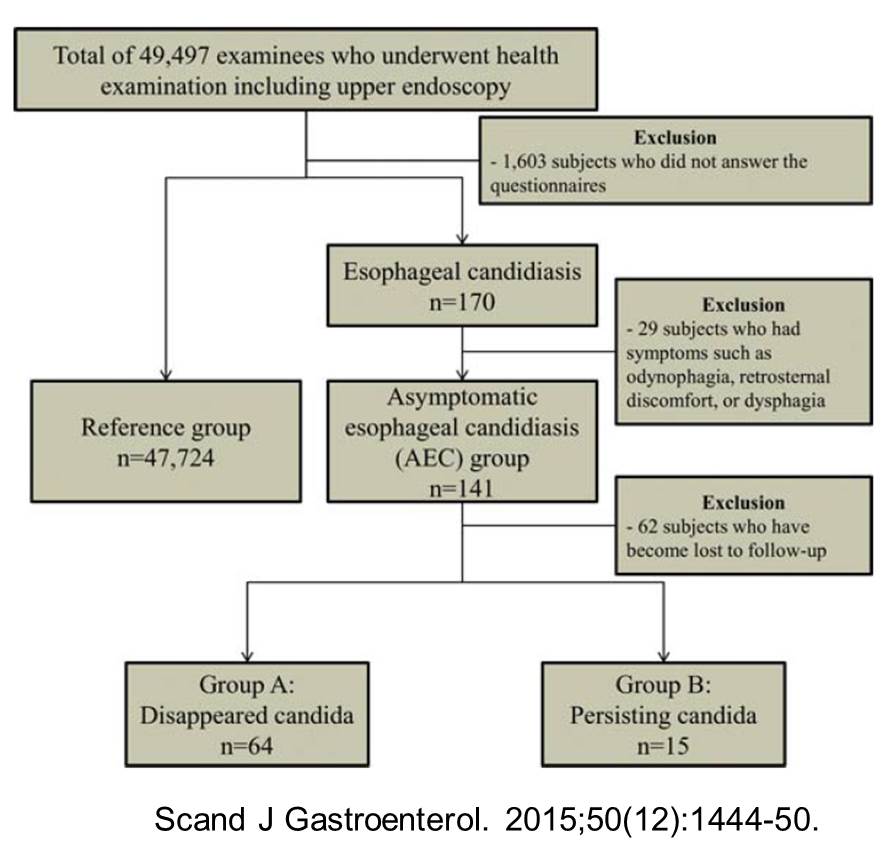
CONCLUSIONS: AEC is rare and old age is the only risk factor. AEC (asymptomatic esophageal candidiasis) does not require medical care because it is a self-limited disease.
РњДТ ГЛНУАц АЫЛч ЕЕСп ЙЋСѕЛѓ НФЕЕ ФЕЕ№ДйСѕРК ННТН ЙЋНУЧЯБтЕЕ ЧеДЯДй. ЧЧКЮАњ РЧЛчАЁ И№Еч СЁПЁ ДыЧЯПЉ comment ЧЯСі ОЪДТ АЭУГЗГ...
* ТќАэ: EndoTODAY НФЕЕФЕ№ДйСѕ
![]() 2. Inflammatory fibrinoid polyp
2. Inflammatory fibrinoid polyp
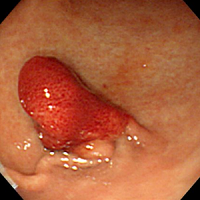
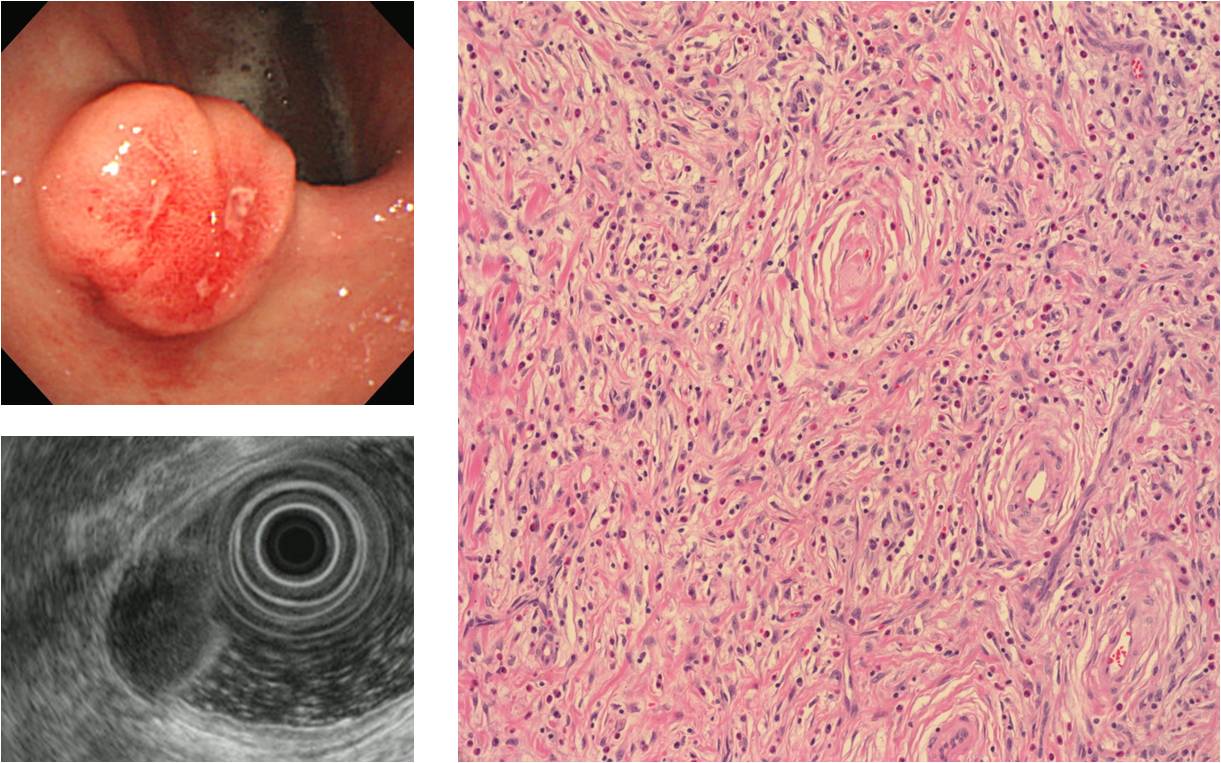
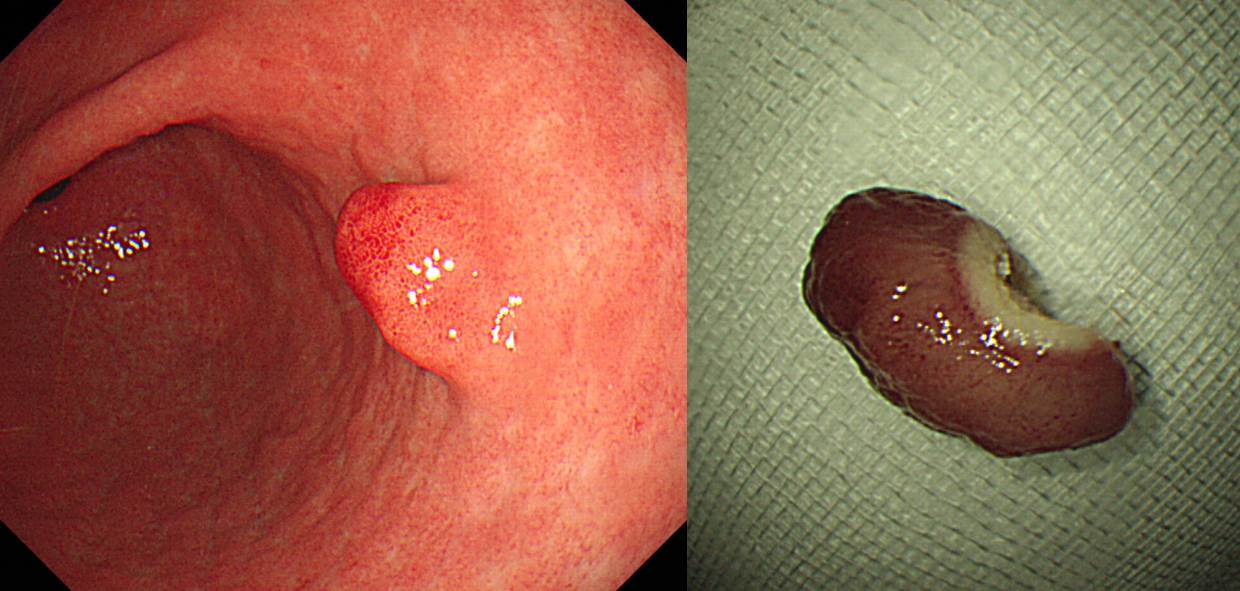
Inflammatory fibrinoid polypРК gastric submucosal granuloma with eosinophilic infiltration, eosinophilic granuloma, hemangiopericytoma, fibroma, inflammatory pseudotumor Ею ДйОчЧб РЬИЇРИЗЮ КвЗШДј СООчРдДЯДй. СЖСїЧаРћРИЗЮ МЖРЏСЖСї, ЧїАќ, ШЃЛъБИИІ ЦїЧдЧб ИЙРК ПАСѕММЦїЕщЗЮ БИМКЕЧОю РжАэ БЙМвРћРЮ КёНХЛ§МК МКРхРЛ ЧЯДТ СњШЏРдДЯДй. СжЗЮ РЇПЁ ЙпЛ§ЧЯСіИИ ЕхЙААд МвРх, ДыРх, НФЕЕПЁМЕЕ ЙпЛ§Чв Мі РжНРДЯДй. ОЧМККЏШДТ КИАэЕШ Йй ОјНРДЯДй. РЇГЛНУАцПЁМДТ СжЗЮ pedunculated polypРЧ ЧќХТАЁ ИЙРКЕЅ SMTПЭ КёНСЧЯАд КИРЬДТ АцПьЕЕ РжНРДЯДй.
IFP arises from submucosa of the GI tract. It consists of loose connective tissue with a rich vasculature and abundant fibrous component. Usually the lesion was sessile or polypoid with ulceration of the overlying mucosa.
 SMTУГЗГ КИПДДј АцПьРЬАэ wedge resectionРИЗЮ ШЎСјЧв Мі РжОњНРДЯДй. МіМњРќ impressionРК GISTПДНРДЯДй.
SMTУГЗГ КИПДДј АцПьРЬАэ wedge resectionРИЗЮ ШЎСјЧв Мі РжОњНРДЯДй. МіМњРќ impressionРК GISTПДНРДЯДй.
 Inflammatory fibrinoid polyp
Inflammatory fibrinoid polyp
![]() 3. ГЛНУАц РАОШМвАп Лѓ МБСОРЛ РЧНЩЧЯПДДј СЖБтРЇОЯ
3. ГЛНУАц РАОШМвАп Лѓ МБСОРЛ РЧНЩЧЯПДДј СЖБтРЇОЯ
 УЙ ГЛНУАц
УЙ ГЛНУАц
 РЧЗк ШФ РчАЫ
РЧЗк ШФ РчАЫ
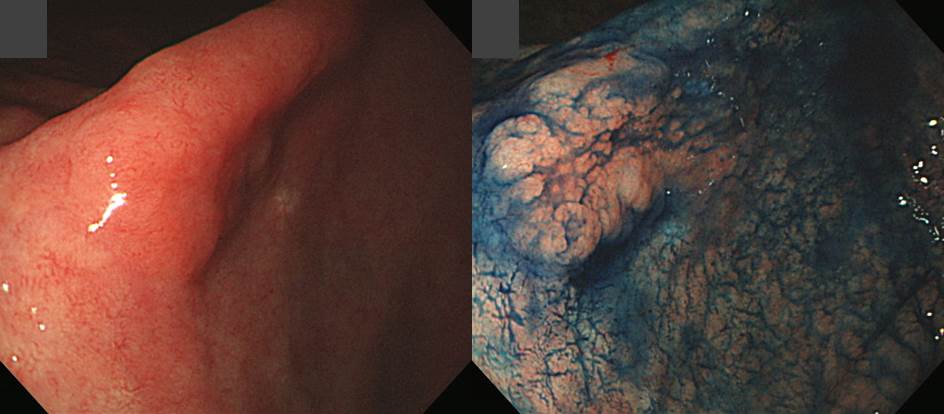
Stomach, subtotal gastrectomy:
Early gastric carcinoma
1. Location : lower third, Center at angle and anterior wall
2. Gross type : EGC type IIa
3. Histologic type : tubular adenocarcinoma, poorly differentiated
4. Histologic type by Lauren : diffuse
5. Size : 2.1x1.2 cm
6. Depth of invasion : invades mucosa (muscularis mucosae) (pT1a)
7. Resection margin: free from carcinoma, safety margin: proximal 3 cm, distal 5 cm
8. Lymph node metastasis : no metastasis in 32 regional lymph nodes (pN0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
![]() 4. Recurrent ulcer with outlet obstruction
4. Recurrent ulcer with outlet obstruction
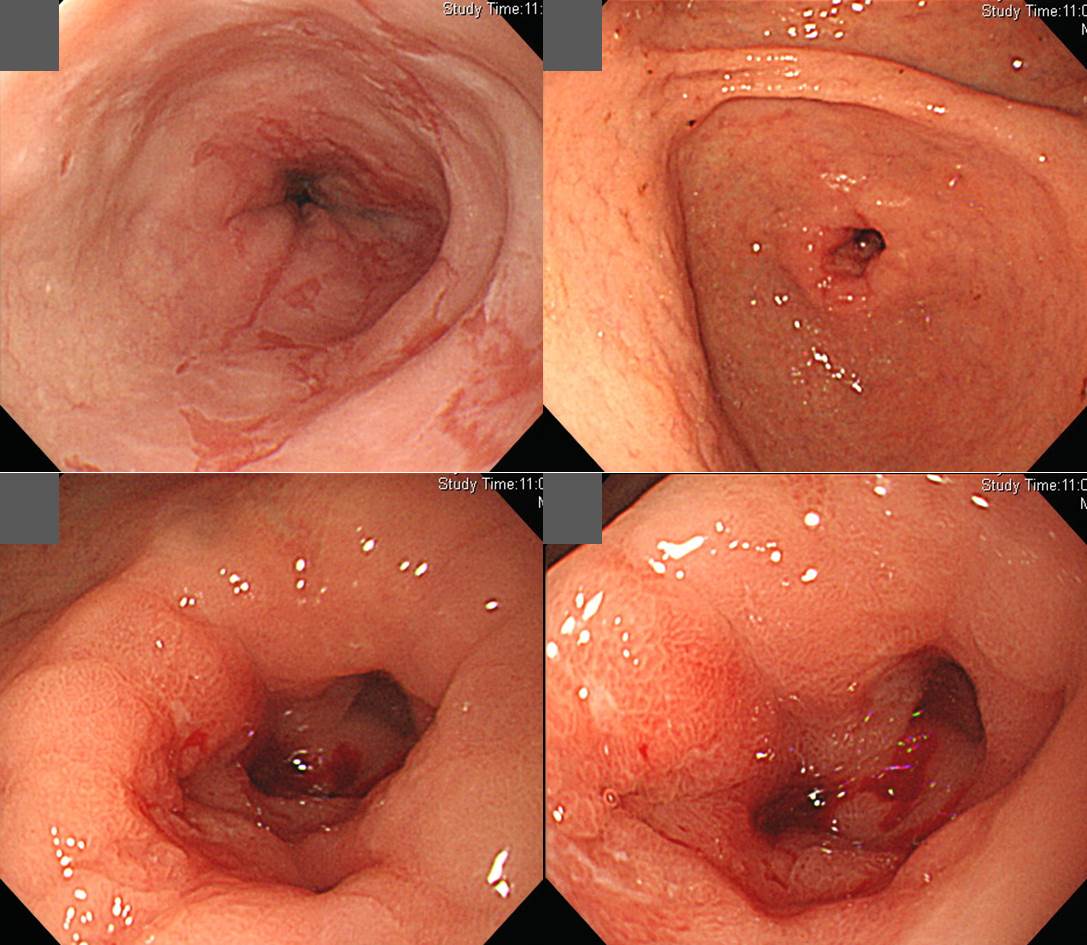
КѓЧїАњ ОюСіЗЏПђРИЗЮ ГЛПјЧЯМЬНРДЯДй. ЧїЛіМвДТ 7РЬОњАэ УЖРК 5ПДНРДЯДй. СЖСїАЫЛчПЁМДТ Hp (+) gastritisЗЮИИ ГЊПЭ СІБеФЁЗсПЭ РЇЛъКаКёОяСІСІИІ ХѕПЉЧЯПДНРДЯДй. ШЏРкАЁ РсНУ follow up lossЕШ ШФ ДйНУ ПРМЬДТЕЅ ОЦЗЁ ЛчСјАњ ААОвНРДЯДй. ЧяИЎФкЙкХЭАЁ СІБеЕЧСі ОЪРК ЛѓХТПДАэ УпАЁФЁЗс ШФ ШЃРќЕЧОњНРДЯДй.
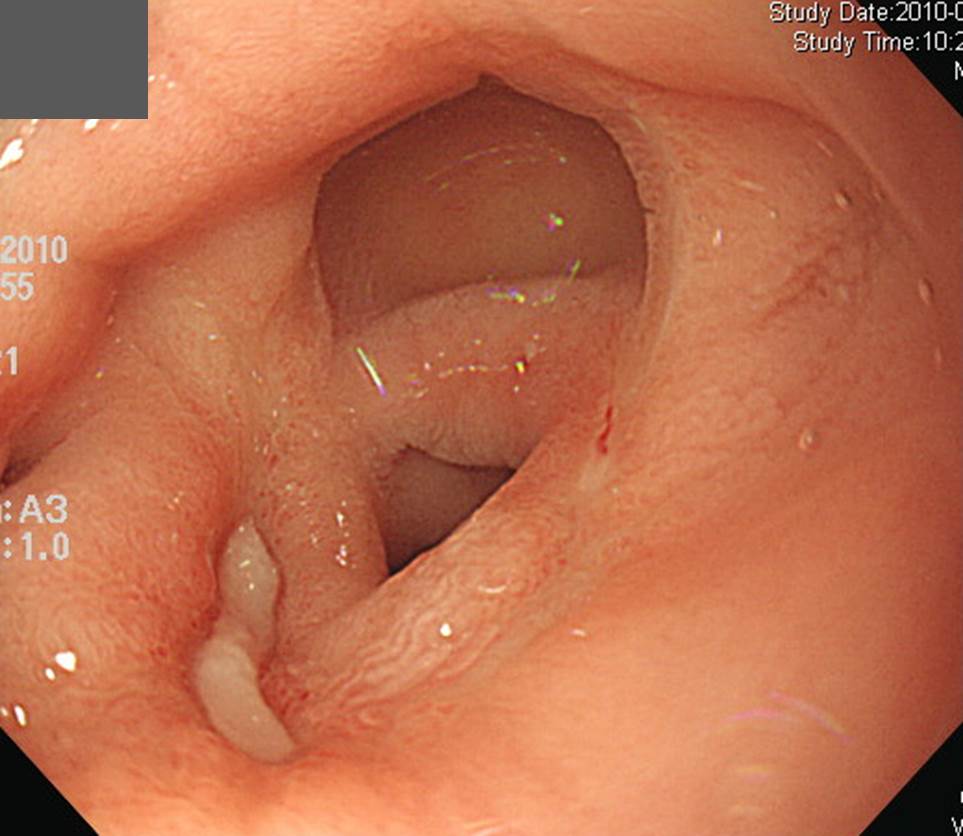
РњДТ ОЯРИЗЮ ЦЧДмЧЯПДДТЕЅ УжСО АсАњАЁ recurrent ulcerЗЮ ГЊПЭ СЖБн УЂЧЧЧпНРДЯДй. РЇОЯАњ РЇБЫОчРЧ БИКаРК ДУ ОюЗЦНРДЯДй. ГЛНУАцРЛ 25ГтТА ЧЯАэ РжДТЕЅ ПЉРќШї ОюЗЦНРДЯДй.
![]() 5. A colon LST
5. A colon LST
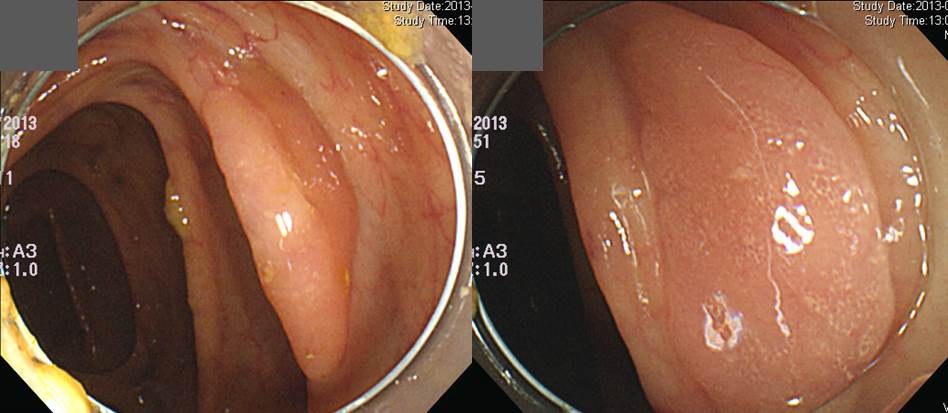
A colonРЧ LSTРдДЯДй. СЖСїАЫЛчАЁ hyperplastic polypРИЗЮ ГЊПдРИГЊ EMRРЛ ЧЯПДАэ УжСО АсАњДТ serrated adenomaЗЮ ГЊПдНРДЯДй.
* ТќАэ: EndoTODAY Serrated adenoma
![]() [References]
[References]
1) SMC Endoscopy Unit ЛяМКМПяКДПј ГЛНУАцНЧ
2) SMC Monday GI conference ЛяМКМПяКДПј РЯПјГЛНУАцБГНЧ ПљПфСЁНЩМвШБтС§ДуШИ
3) SMC Thursday endoscopy conference ЛяМКМПяКДПј РЯПјГЛНУАцБГНЧ ИёПфСЁНЩГЛНУАцС§ДуШИ
© EndoTODAY Endoscopy Learning Center. Jun Haeng Lee.