EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Metachronous gastric cancer after ESD for EGC. 이시성 위암, 이시성 재발] - 終
[Metachronous gastric cancer after ESD for EGC. 이시성 위암, 이시성 재발] - 終

Clin Endosc 2018:51:253
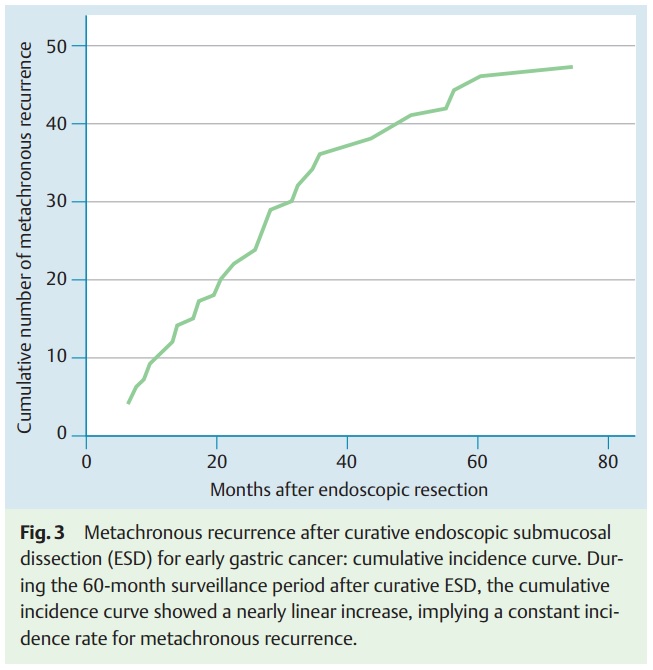
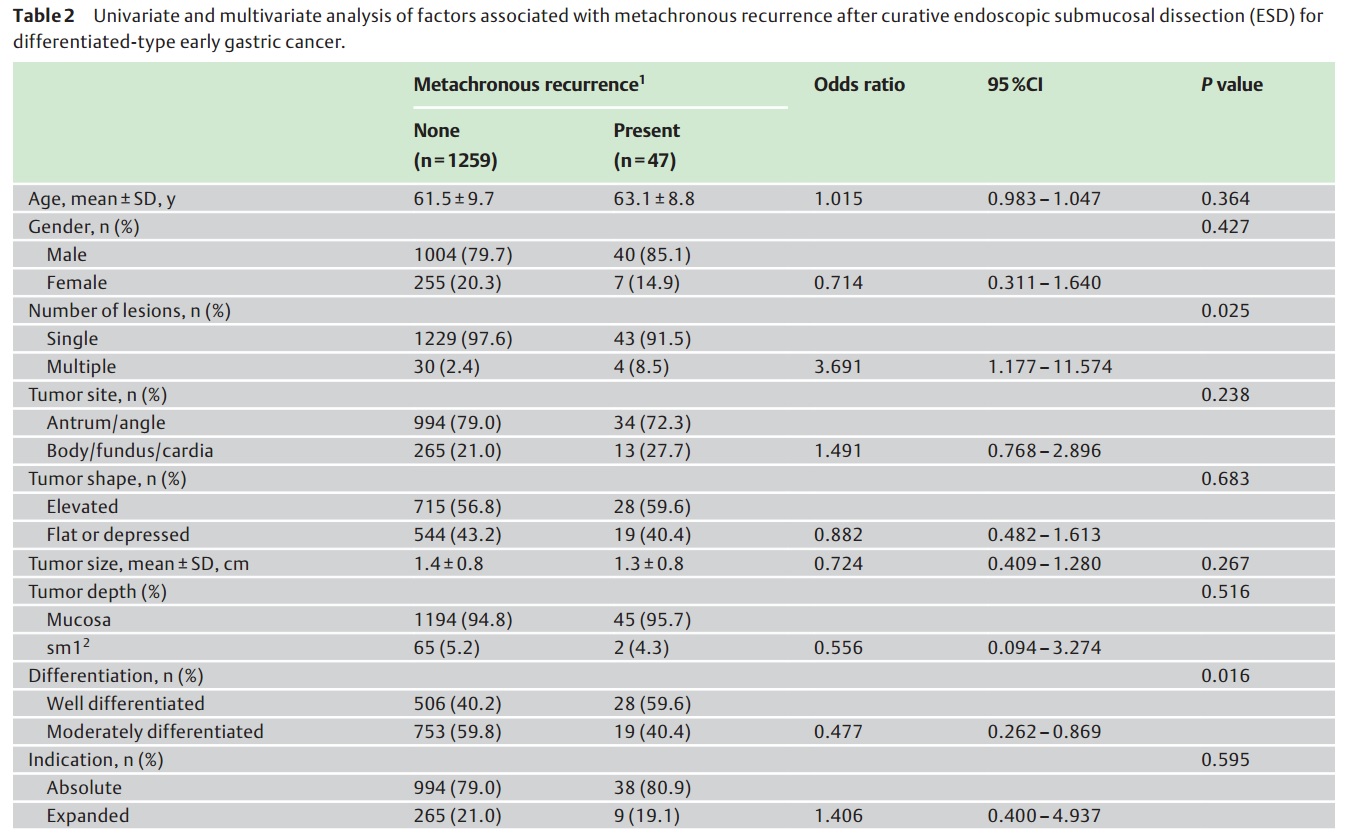
![]() 2015년 삼성서울병원. 내시경으로 치료한 differentiate-type EGC 환자 2,036명 중 curative resection으로 나왔던 1,692명 (83.2%) 중 ESD로 치료하였고 1년 이상 추적관찰이 가능하였던 1,306명에 대한 long-term follow-up data가 발표되었습니다 (민병훈. Endoscopy 2015).
2015년 삼성서울병원. 내시경으로 치료한 differentiate-type EGC 환자 2,036명 중 curative resection으로 나왔던 1,692명 (83.2%) 중 ESD로 치료하였고 1년 이상 추적관찰이 가능하였던 1,306명에 대한 long-term follow-up data가 발표되었습니다 (민병훈. Endoscopy 2015).
Metachronous recurrence는 47명 (3.6%, 47/1306)에서 발견되었습니다. 조기위암이 44예 (93.6%), 진행성위암이 3예였으며, 28예(60.0%)는 ESD로 19예(40.0%)는 수술로 치료하였습니다.
Metachronous recurrence는 처음에 다발성 병소였던 환자와 분화형이 well differentiated에서 많았습니다.
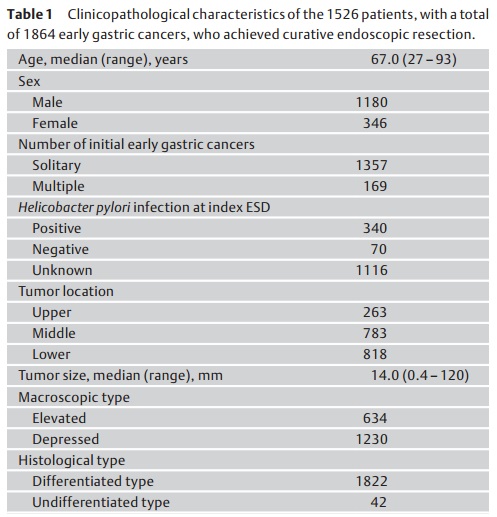
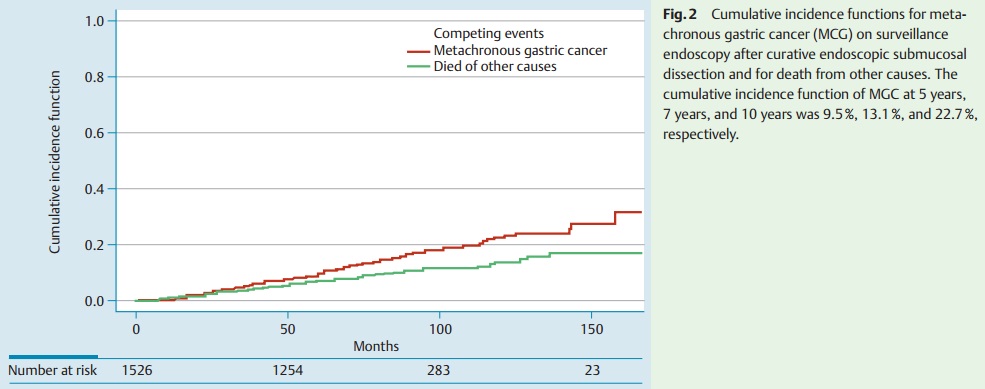
![]() 2015년 동경암센터. 이소성 위암에 대한 가장 대규모 연구가 발표되었습니다 (Abe S. Endoscopy 2015 Dec).
2015년 동경암센터. 이소성 위암에 대한 가장 대규모 연구가 발표되었습니다 (Abe S. Endoscopy 2015 Dec).
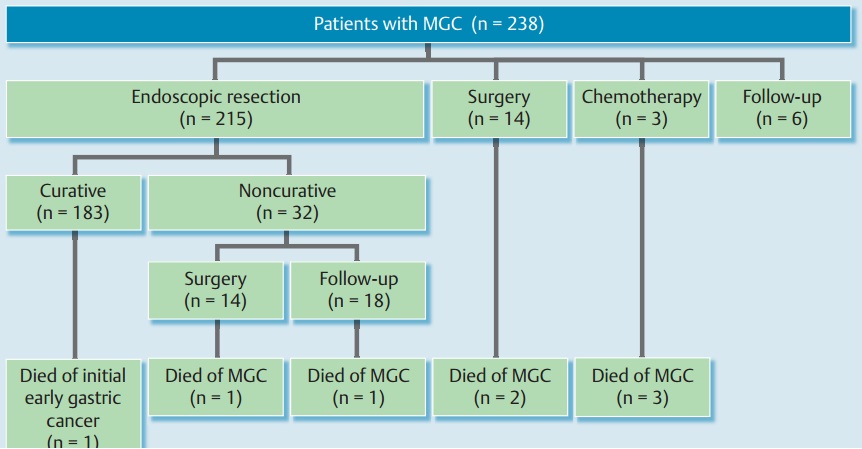
During a median follow-up period of 82.2 months, 238 patients developed MGC post-ESD resection of EGC. The 5-year, 7-year, and 10-year cumulative incidence functions of MGC were 9.5%, 13.1% and 22.7%, respectively. Male sex and multiple initial EGCs were independent risk factors for MGC in the Cox proportional hazard model. Of the 238 patients with MGC, 215 were treated with endoscopic resection, of which 183 achieved curative resection, although one patient later died of his initial EGC. A further 14 patients were treated surgically, three had metastatic disease and received palliative chemotherapy, and the remaining six were observed without any intervention. A total of seven patients died of MGC, five at least 5 years after their index ESD. The 5-year, 7-year, and 10-year DSSs were 99.2%, 98.6%, and 92.5%, respectively.
1999년부터 2006년까지 동경암센터에서 ESD로 치료한 EGC 환자를 분석한 자료입니다. 평균 연령이 67세로 우리나라 환자보다 다소 고령이었습니다. 이소성 위암의 빈도가 5년에 9.5%로 우리나라보다 월등히 높았는데, 그 이유 중 일부는 adenoma가 cancer로 조직진단되었기 때문일 것 같습니다.
이소성 위암 238예 중 28예(11.8%)에서 수술이 이루어졌습니다. 3명이 초치료로 항암치료를 받았다는 점이 특이했습니다 (저희 기관에서는 metastatic disease로 발견된 이소성 위암은 없었습니다). 7명(2.9%)이 이소성 위암으로 사망하였습니다.
Abe 등의 동경암센터 이소성위암 연구에 Imperiale 등이 editorial을 붙였는데 온통 overdiagnosis issue입니다 (Imperiale. Endoscopy 2015 Dec). 관점이 참 많이 다르다고 생각됩니다.
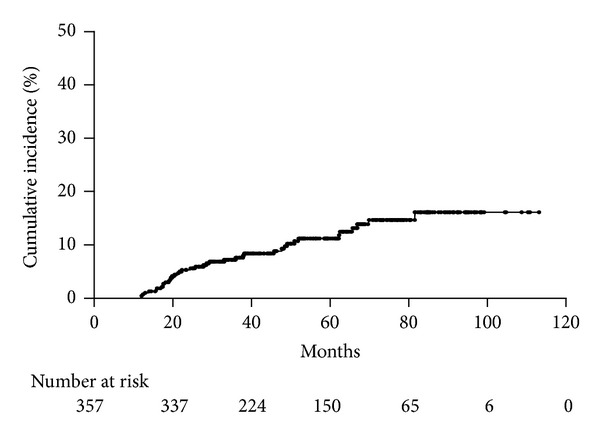
![]() 일본 장소? Sugimoto T. Can J Gastroenterol Hepatol 2015 - Epub
일본 장소? Sugimoto T. Can J Gastroenterol Hepatol 2015 - Epub
The median follow-up period was 4.2 years. Metachronous gastric cancers were found in 23 of 155 patients (3.5% per year). No local recurrences were observed. The cumulative incidence of metachronous gastric cancer was significantly high in IM and NI in the corpus (P=0.0093 and P=0.0025, respectively [log-rank test]). The ORs for IM and NI in the corpus were 2.65 and 3.06, respectively, according to the Cox proportional hazards model (P=0.024 and P=0.0091, respectively).
![]() Boda T. Gastroenterol Res Pract 2014
Boda T. Gastroenterol Res Pract 2014
The annual incidence of metachronous tumors after ESD was 2.4%.
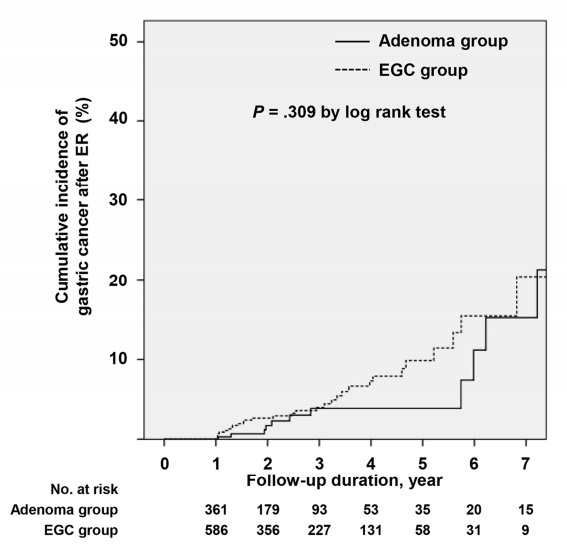
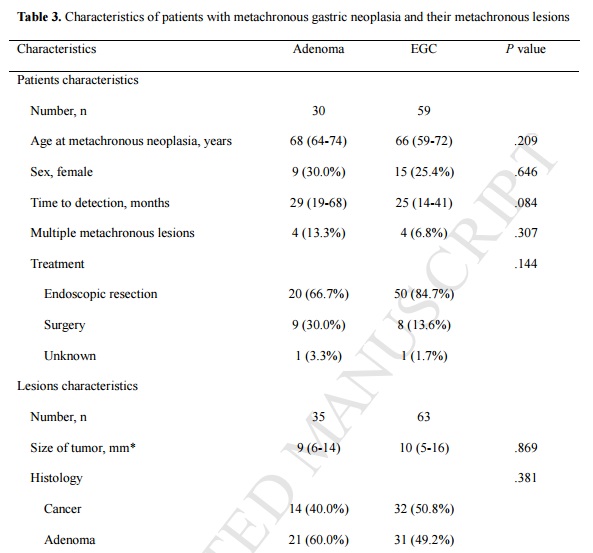
![]() 2015년 8월 강남성모병원에서 선종이나 위암 내시경 치료 후 이소성 병소에 대한 결과를 발표하였습니다 (Yoon SB. GIE). 저도선종을 adenoma 군으로, 고도선종과 암을 EGC 군으로 나누었기 때문에 약간 혼동되는 면은 있습니다만... 저도 선종 내시경 치료 후에도 상당부분 이소성 선종과 이소성 암이 발견되다는 점을 잘 보여주고 있습니다.
2015년 8월 강남성모병원에서 선종이나 위암 내시경 치료 후 이소성 병소에 대한 결과를 발표하였습니다 (Yoon SB. GIE). 저도선종을 adenoma 군으로, 고도선종과 암을 EGC 군으로 나누었기 때문에 약간 혼동되는 면은 있습니다만... 저도 선종 내시경 치료 후에도 상당부분 이소성 선종과 이소성 암이 발견되다는 점을 잘 보여주고 있습니다.
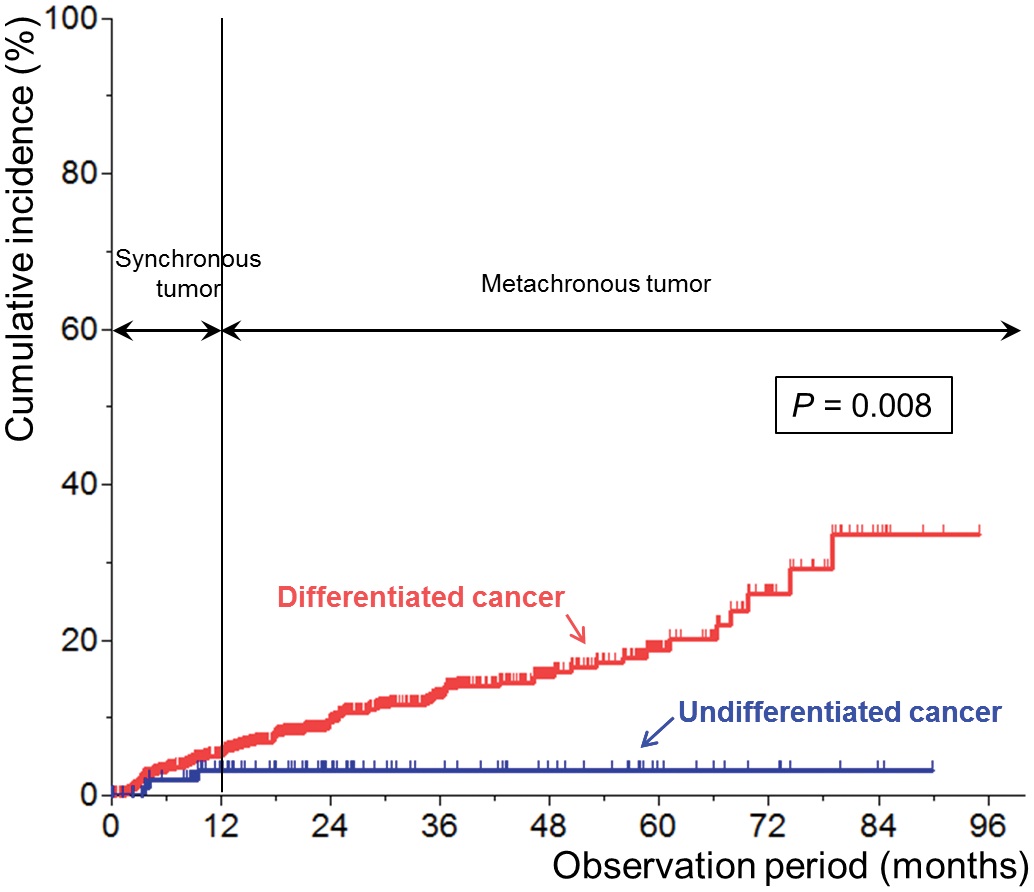
![]() 2016년 연세대학교 (Park CH. PLoS One 2016). Undifferentiated type EGC에 대한 내시경 치료 후 이소성 재발이 적었습니다. 심지어는 동시성 재발도 적었다고 합니다. 결론("These findings suggest that ESD should be actively considered as a possible treatment for undifferentiated type EGCs")은 조금 이상했습니다. 이소성 재발이 적다는 것이 어떻게 내시경 치료의 적응증 확대로 연결되는지 이해할 수 없습니다.
2016년 연세대학교 (Park CH. PLoS One 2016). Undifferentiated type EGC에 대한 내시경 치료 후 이소성 재발이 적었습니다. 심지어는 동시성 재발도 적었다고 합니다. 결론("These findings suggest that ESD should be actively considered as a possible treatment for undifferentiated type EGCs")은 조금 이상했습니다. 이소성 재발이 적다는 것이 어떻게 내시경 치료의 적응증 확대로 연결되는지 이해할 수 없습니다.
그런데 2010년 같은 기관에서 발표한 논문(Seo JH. Digestion 2010)과 결론이 반대인 것 같습니다. 2010년에는 "undifferentiated histology and upper location of the primary lesion were correlated with the occurrence of metachronous gastric cancer"였기 때문입니다.
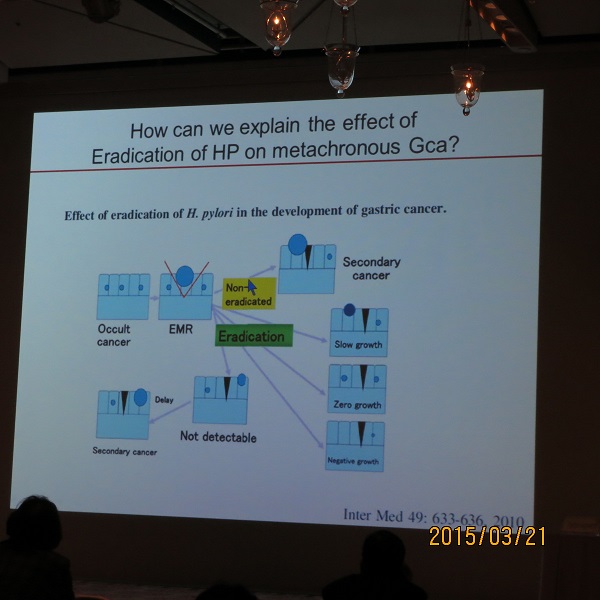
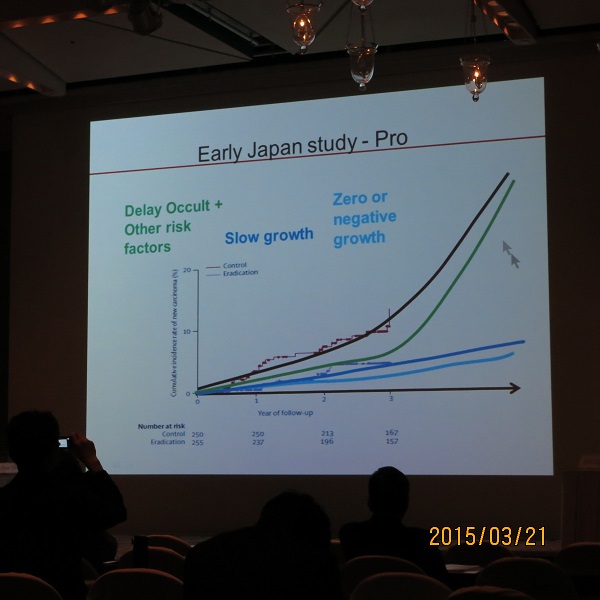
![]() 2015년 3월 20일 한일헬리코박터학회 경북대학교 전성우 교수님 강의. Metachronous recurrence after ESD
2015년 3월 20일 한일헬리코박터학회 경북대학교 전성우 교수님 강의. Metachronous recurrence after ESD
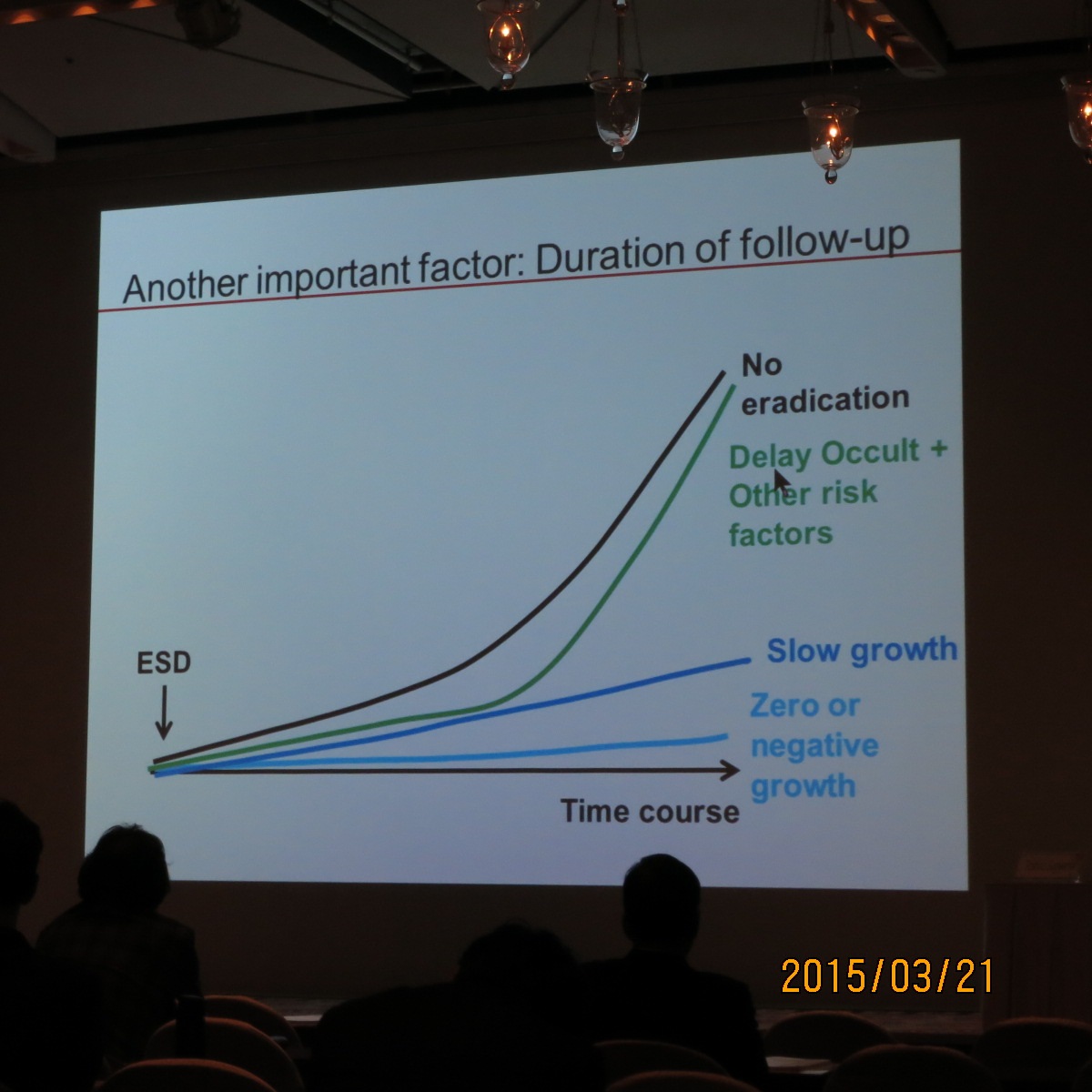
전성우 교수님께서 경북대의 ESD 후 metachronous recurrence에 대한 자신의 데이타를 보여주신 후 비슷한 다른 연구 결과들을 보여주면서 매우 중요한 가설을 제시하셨습니다. ESD 후 Hp 제균이 metachronous cancer 발생에 미치는 영향은 follow-up 기간에 따라 달라진다고 설명하셨습니다.
Hp 제균 초기에는 암의 진행을 억제합니다. 따라서 Hp 제균이 metachronous cancer 발생을 줄이는 것으로 나옵니다. 그러나 위암은 Hp이외의 다른 많은 요인에 의해 발생합니다. 따라서 장기간 추적관찰을 하면 Hp 이외의 다른 인자(diet, atrophic anc metaplastic gastritis, epigenetic change)의 영향이 상대적으로 중요해지므로 Hp 제균에 의한 효과가 상대적으로 작아지고 결국 차이가 없는 것으로 나옵니다. 이 분야에 대한 설명 중 이처럼 간결하고 명료한 가설은 처음이었습니다. 전성우 선생님. 멋집니다.
관련논문: Failure of Helicobacter pylori eradication and age are independent risk factors for recurrent neoplasia after endoscopic resection of early gastric cancer in 283 patients. Kwon YH. Aliment Pharmacol Ther 2014;39:609-18
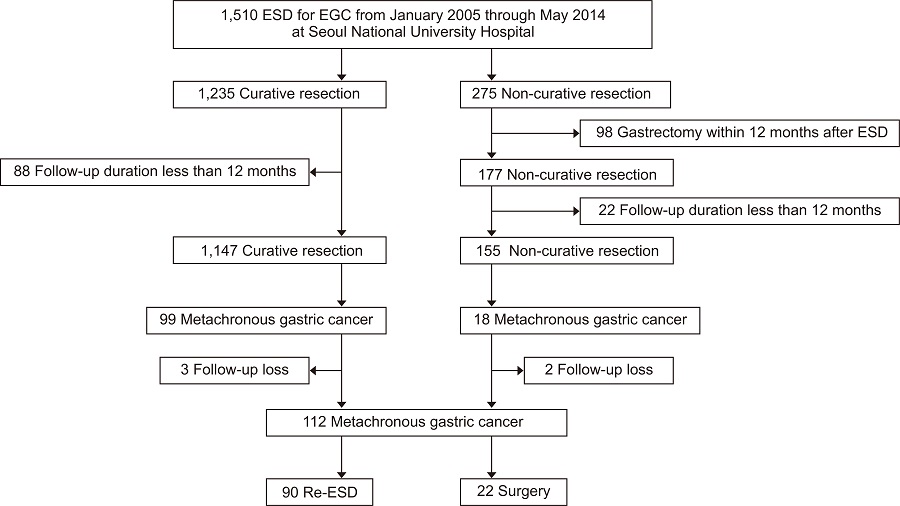
![]() 2020년 서울대 (Gut and Liver 2020)
2020년 서울대 (Gut and Liver 2020)
서울대 팀에서는 112명 중 90명 (80.3%)을 ESD로 치료했다는 놀라운 성적을 보고하였습니다.
이 논문에 대한 editorial에는 그간 발표된 논문들의 내용이 잘 정리되어 있었습니다.
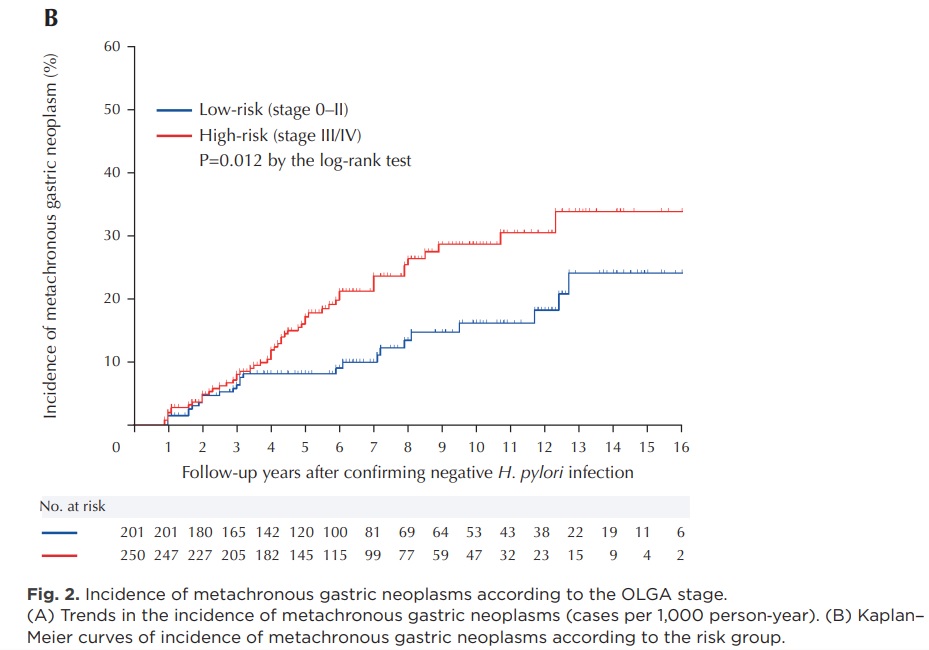
![]() 2026년 JGC. 국립암센터에서 Hp 음성 EGC에서 ESD 후 OLGA/OLGIM staging이 이시성 위암 예측에 도움이 된다고 보고했습니다.
2026년 JGC. 국립암센터에서 Hp 음성 EGC에서 ESD 후 OLGA/OLGIM staging이 이시성 위암 예측에 도움이 된다고 보고했습니다.
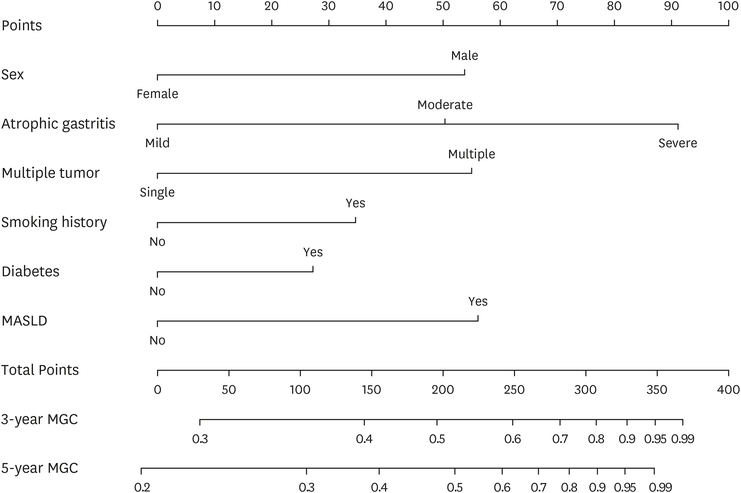
![]() 2026년 JGC. 중국에서 ESD와 Hp 제균치료 후 metachronous cancer 발생에 대한 nomogram을 제안하였습니다.
2026년 JGC. 중국에서 ESD와 Hp 제균치료 후 metachronous cancer 발생에 대한 nomogram을 제안하였습니다.
![]() [Cases]
[Cases]
날문 위암 ESD 하였는데 또 다른 방향에서 날문 위암이 나옴
이소성 위암 중 수술이 필요한 경우가 종종 발견됩니다.
이소성 위암 중 ESD 후 수술이 필요한 경우도 있습니다.
Stomach, endoscopic submucosal dissection:
Early gastric carcinoma
1. Location : mid antrum
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 13 mm (2) vertical diameter, 12 mm
6. Depth of invasion : invades submucosa, (depth of sm invasion : 1000 ㎛) (pT1b)
7. Resection margin : involved deep resection margin by carcinoma with cauterized artifacts safety margin : distal 15 mm, proximal 13 mm, anterior 16 mm, posterior 14 mm, deep 0 mm (sm only)
8. Lymphatic invasion : present (+++)
9. Venous invasion : suspicious
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
2008년 synchronous EGCs로 ESD (x2) 후 첫 이소성 위암(2011)은 ESD로 해결할 수 있었으나 두번째 이소성 위암(2015)은 ESD 후 아래와 같이 수술이 필요한 결과가 나왔습니다.
Stomach: LC of mid body, ESD:
Early gastric carcinoma
1. Location : body, lesser curvature
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 11 mm (2) vertical diameter, 8 mm
6. Depth of invasion : invades submucosa, (depth of sm invasion : 400 ㎛) (pT1b)
7. Resection margin : involved deep resection margin by carcinoma with cauterized artifacts safety margin : distal 6 mm, proximal 9 mm, anterior 8 mm, posterior 10 mm, deep 0 ㎛
8. Lymphatic invasion : present
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
고도선종 내시경치료 후 이소성으로 위암이 발견되는 경우도 있습니다.
Stomach, ESD : Early gastric carcinoma
1. Location : antrum, anterior wall
2. Gross type : EGC type IIb
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 12 mm (2) vertical diameter, 8 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 7 mm, proximal 4 mm, anterior 4 mm, posterior 8 mm, deep 600 ㎛
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
Metachronous cancer develops in 1-2%/year after ESD for EGC. Six years after ESD for EGC, a metachronous cancer was found in the lesser curvature aspect of the high body. ESD was done again.

[1st ESD (left)]
ESD: Early gastric carcinoma
1. Location : proximal antrum, greater curvature
2. Gross type : EGC type IIb+IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 14 mm (2) vertical diameter, 13 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 11 mm, proximal 12 mm, anterior 18 mm, posterior 12 mm
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent[2nd ESD (right)]
ESD: Early gastric carcinoma
1. Location : high body, lesser curvature
2. Gross type : EGC type IIa+IIc
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 18 mm (2) vertical diameter, 14 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N) safety margin : distal 7 mm, proximal 6 mm, anterior 12 mm, posterior 10 mm, deep 200 ㎛
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
Borrmann type 4 gastric cancer may develop after ESD.
2021년 (F/64)
Biopsy at peritoneal seeding nodule
![]() [FAQ]
[FAQ]
[2021-3-31. 학생 질문]
반복적으로 재발하는 EGC에 대해서 앞으로 어떻게 해야할지 궁금합니다. 원래 그냥 ESD한 환자라면 경과관찰을 하겠지만, 이렇게 재발하는 환자의 경우에는 다음 번에 또 재발할 경우 위절제수술을 고려해야 하나요?
[2021-4-1. 이준행 답변]
좋은 질문 감사합니다. 한 마디로 답하면 재발의 종류에 따라 다릅니다.
조기위암 내시경치료 후 병리학적으로 완전절제로 판단된 환자의 동일 병소(index cancer)의 국소, 림프절 전이 혹은 원격 재발은 상당히 적습니다 (EndoTODAY Longterm outcome of endoscopic curative resection of EGC). 국소 재발은 상황에 따라서 소작술, second ESD, 혹은 수술을 적용합니다. 림프절 전이는 당연히 수술을 합니다. 원격 재발은 안타까운 경우이지만 항암치료를 합니다 (EndoTODAY Extragastric recurrence after ESD for EGC).
Index cancer의 재발보다는 이소성 (異所性) 재발이 흔합니다 (EndoTODAY 이소성 재발). 위 내의 다른 속에서 위암이 새로 발생하는 경우인데 그 빈도는 1년에 1-2%입니다. 5년이면 5-10%라는 의미이니 상당히 흔합니다.
이소성 재발의 치료원칙은 위암이 처음 진단되었을 때와 비슷합니다. 내시경 절제술 적응증이면 내시경 절제술을 하고 수술 적응증이면 수술을 합니다. 2번째, 3번째, 4번째.... 암이었다는 이유로 내시경 절제술을 고려하지 않고 수술하는 경우는 거의 없습니다. 위는 소중한 장기이고 가능하면 끝까지 가지고 사는 것이 유리하기 때문입니다. Subtotal gastrectomy나 total gastrectomy 후 삶의 질은 상당히 떨어집니다.
[2021-3-31. 학생 질문]
시술을 하기 전 조직검사에서는 well differentiated였는데, ESD 후 조직검사 결과가 moderately differentiated로 나왔다면, 이 경우에는 수술을 고려해야하나요?
[2021-4-1. 이준행 답변]
ESD 전후 세포형의 차이는 상당합니다 (EndoTODAY Pathologic discrepancy). 조직검사는 부분 검사이고 ESD 검체에 대한 검사는 전체 검사이기 때문입니다. 부분을 보고 전체를 예측하는 것은 항상 정확하지 않습니다.
ESD 전후 세포형이 다르게 나올 때의 원칙은 간단합니다. ESD 검체에 대한 병리결과에 따라 additional surgery 여부를 결정합니다.
![]() [References]
[References]
1) 胃 ESD 후 내시경 소견 (이준행). 삼성서울병원 Winter school 2018

© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.