EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [내과학회 런천 강의 K-CAB : GERD 치료의 최신 지견 및 P-CAB의 역할]
[내과학회 런천 강의 K-CAB : GERD 치료의 최신 지견 및 P-CAB의 역할]
Potassium competitive acid blocker, P-CAB 계열의 국내 신약 Tegoprazan을 소개하겠습니다. CJ에서 개발하였고 K-CAB이라는 상품명으로 곧 launching될 예정입니다. (씨제이헬스케어 Kolmar, 2019년 3월?)
Tegoprazan J Pharmacol Exp Ther 2018
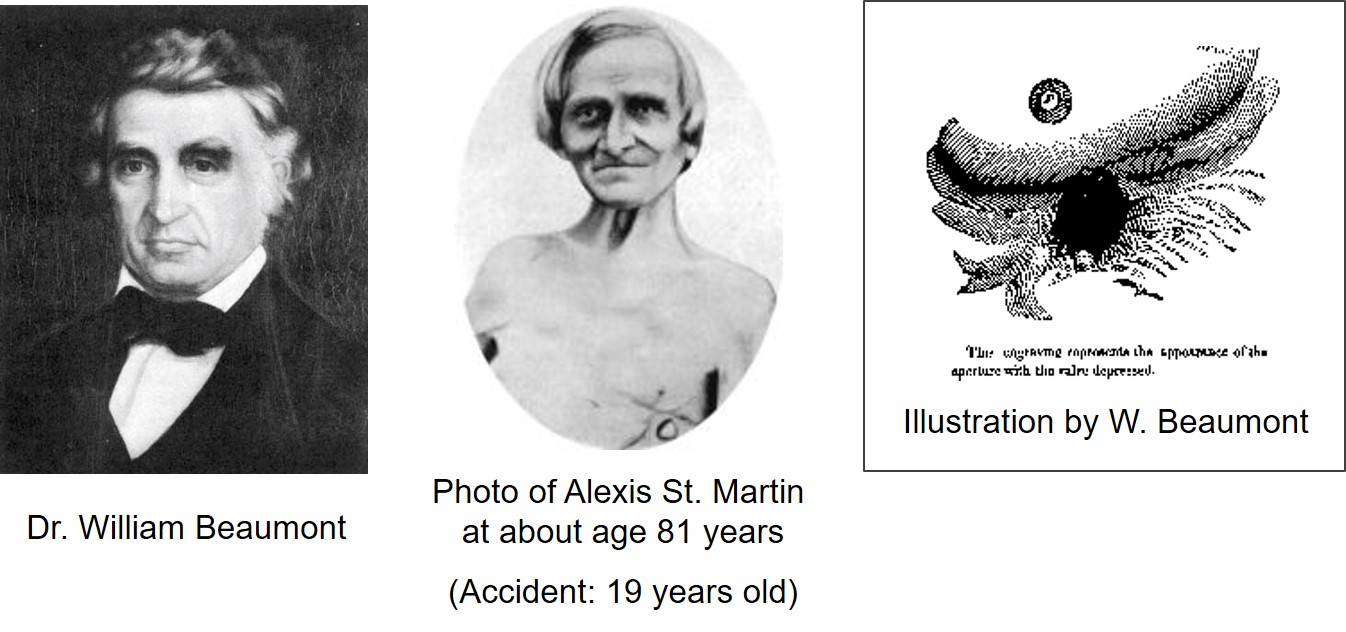
위산과 위산분비억제제의 역사에는 두 명의 유명한 이름이 나옵니다. 한명은 의사이고 한명은 환자입니다. Alexis St. Martin이라는 미국 병사는 군대에서 큰 사고를 당한 후 겨우 목숨을 건졌지만 복부에 fistula가 남았습니다. 그의 주치의 William Beaumant는 이 fistula를 통하여 위의 physiology를 연구하였고, 이 둘의 만남을 통하여 위의 내부가 acidic하다는 것이 밝혀졌습니다. 위산, gastric acid라는 개념이 세상에 처음 소개된 것입니다. 1822년 6월 사고 후 첫 만남에 대한 Beaumont 박사의 증언입니다. 내장이 다 튀어나온 끔직한 상황으로 위에 perforation이 있었는데 그 크기는 두번째 손가락이 들어갈 정도였고, 이를 통하여 음식물이 나오고 있었다는 것입니다.
사고 3년 후인 1825년부터 13년에 걸쳐 238가지 연구를 진행한 Beaumont 박사는 1833년 Experiments and observations on the gastric juice라는 280페이지 논문을 발간하였습니다. 이 논문은 현재 Google에서 e-book으로 보실 수 있습니다. Fistula를 통하여 여러 측정 기구를 넣고 빼면서 진행되었던 흥미로운 실험과정이 상세히 기술되어 있습니다.
위체부 fundic gland의 neck 부위에 위치한 parietal cell이 histamine, acetylcholine, gastrin에 자극을 받으면 그림과 같이 모양이 변하면서 위산이 분비됩니다. 그 과정에서 hydrogen-potassium pump가 중요한 역할을 합니다. 위산분비 억제제의 효시는 cimetidine과 같은 histamine antagonist이지만, 현재 많이 사용되는 종류는 1세대 및 2세대 proton pump inhibitor이며, 오늘 소개드리는 종류는 Potassium competitive acid blocker, P-CAB입니다.
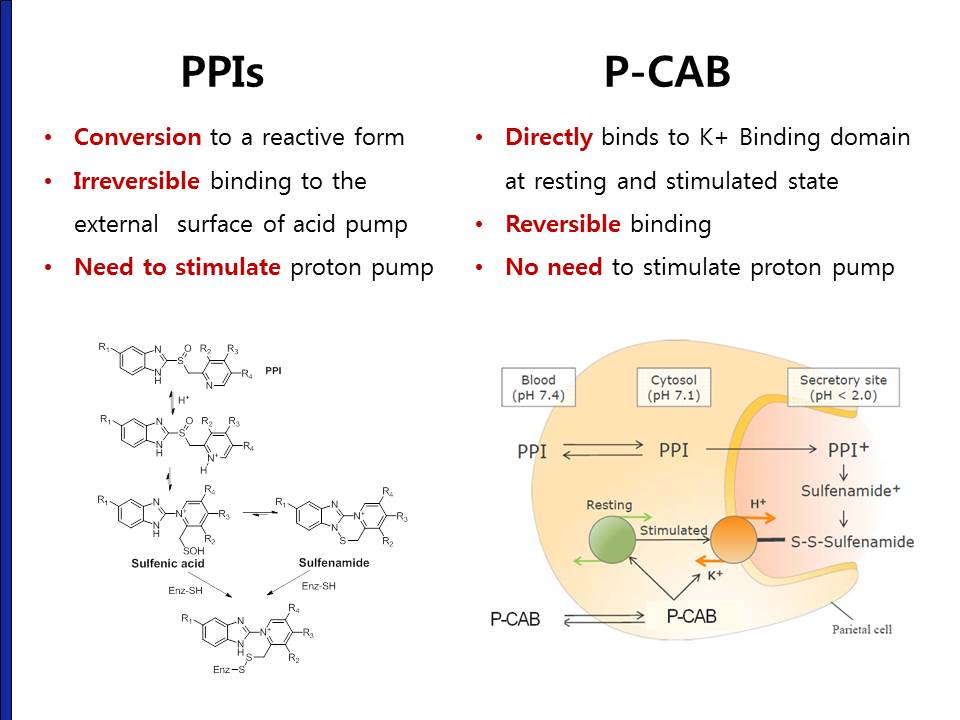
PPI와 P-CAB은 어떤 차이가 있는지 살펴보겠습니다. 당연한 이야기이겠지만 proton pump에서의 binding site가 서로 다르고 mode of action에 중요한 차이가 있습니다. PPI는 그 자체가 prodrug입니다. 따라서 reactive form으로 변형된 후 작용할 수 있으며 비가역적으로 결합합니다. 이를 위하여 proton pump 자체가 stimulation 되어야 합니다. 이 때문에 식전에 투여하는 것이지요. 반면 P-CAB은 prodrug이 아니므로 proton pump의 stimulation 없이 직접 reversible binding을 합니다. 따라서 식사와 무관하에 투여할 수 있습니다.
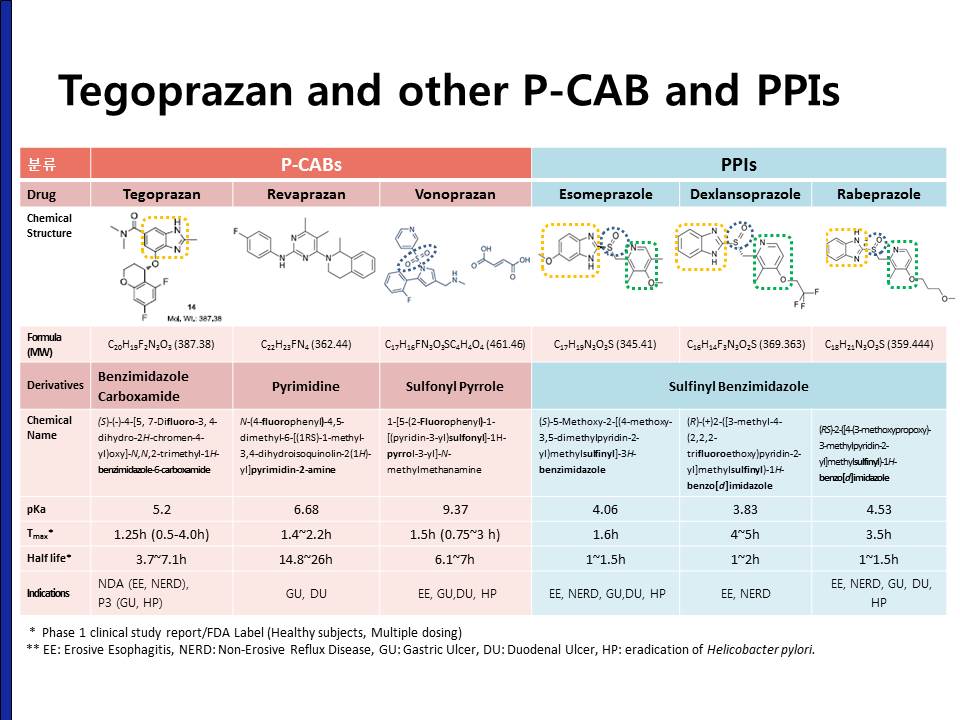
(1) 여러 종류의 PPI는 분자 구조가 서로 비슷합니다. 반면 현재까지 시판된 세 종류의 P-CAB은 분자 구조에 상당한 차이가 있습니다. 기존에 개발 혹은 시판되었던 P-CAB은 hepatotoxicity가 문제였는데 오늘 소개드리는 tegoprazan, 즉 K-CAB은 분자구조가 전혀 다르기 때문에 부작용 profile에도 차이가 있어서 hepatotoxicity 문제가 없었던 것으로 생각됩니다. (2) Tegoprazan의 half life는 3.7에서 7.1시간으로 PPI보다는 길고 다른 P-CAB보다는 짧습니다. (3) 기존에 국내에 시판되었던 rebaprazan은 위산분비억제능이 기존의 PPI보다 약하여 peptic ulcer의 적응증이 있을 뿐, GERD에서는 적응증을 받지 못하였습니다. 뒤에서 자세히 말씀드리겠지만 tegoprazan, 즉 K-CAB은 강력한 위산 분비 억제능을 가지고 있어서 주로 GERD에서 사용하도록 연구개발되고 있습니다.
P-CAB, 특히 Tegoprazan의 장점은 아래와 같습니다.
Benefits of K-CAB compared to PPI More potent acid suppression
More rapid acid inhibition
Less dependent on CYP2C19
No food effect
Optimal for H. pylori eradication
Excellent safety profile
pH 4이상으로 비교할 때보다 pH 6이상으로 비교하면 현저한 차이가 납니다.
1일, 7일 모두 1시간 이내에 pH 4이상으로 올라갑니다.
Tegoprazan 50mg으로 야간에서 pH 4이사으로 유지됩니다.
Tegoprazan이 식전과 식후 투약 시 큰 차이가 없다는 자료입니다.
Tegoprazan의 통상 용량은 50mg/day입니다. 이를 하루 두 번 투약하면 거의 하루 종일 pH가 6이상으로 유지됩니다. 이와 같은 강력한 위산억제는 헬리코박터 제균치료에 유용하에 작용할 것으로 예상하고 있습니다.
국내 임상연구 결과는 2018년 9월 19일 conference에서 원광대 최석채 교수님께서 발표한 바 있어 이 내용도 소개하였습니다.
2상 key 결과
3상 key 결과
2,3상 자료를 모은 분석인데, LA-B,C,D에서 대조약에 비하여 tegoprazan의 효과가 더 좋았다는 흥미로운 분석이 가능했습니다.
NERD에 대한 placebo controlled data에서 4주에 유의한 효과가 있었습니다.
Safety profile은 대조약과 차이가 없었다고 합니다. LFT 상승도 대조약과 차이가 없었습니다. 과거 레바넥스(rebaprazan)에서 종종 hepatotoxicity가 있었다는 것과 확연한 차이이며 tegoprazan의 특장점인 것으로 생각됩니다.
[2018-10-27. 좌장 질문]
P-CAB이 PPI를 replace할 수 있을 것으로 생각하십니까?
[2018-10-27. 이준행 답변]
P-CAB이 PPI의 unmet need에 대한 좋은 대안이 될 것은 틀림없다고 생각합니다. 지금까지의 연구 결과와 일본의 시장 현황을 살펴볼 때, Helicobacter 제균치료와 NERD에서 우선적으로 사용될 수 있을 것입니다. 그러나 위산의 과도한 억제도 나름대로 또 다른 문제를 발생시킬 수 있기 때문에 환자의 상황에 따라 두 종류의 약제가 상호 보완적으로 쓰이지 않을까 예상하고 있습니다.
위산 분비 억제 치료가 필요한 환자를 치료하는 의사로서 새롭고 안전하고 강력한 치료약제가 나왔다는 점에서 매우 반가운 일입니다. 약제 launching 후 임상 경험이 쌓이면 좀 더 세부적인 의견을 드릴 수 있을 것 같습니다.
![]() [Selected posters]
[Selected posters]
Cribriform-morular variant papillary thyroid cancer의 절반은 familial adenomatous polyposis입니다. 2017년 7월 27일 목요집담회에서 한 증례를 논한 바 있어 아래에 옮겨 소개합니다.
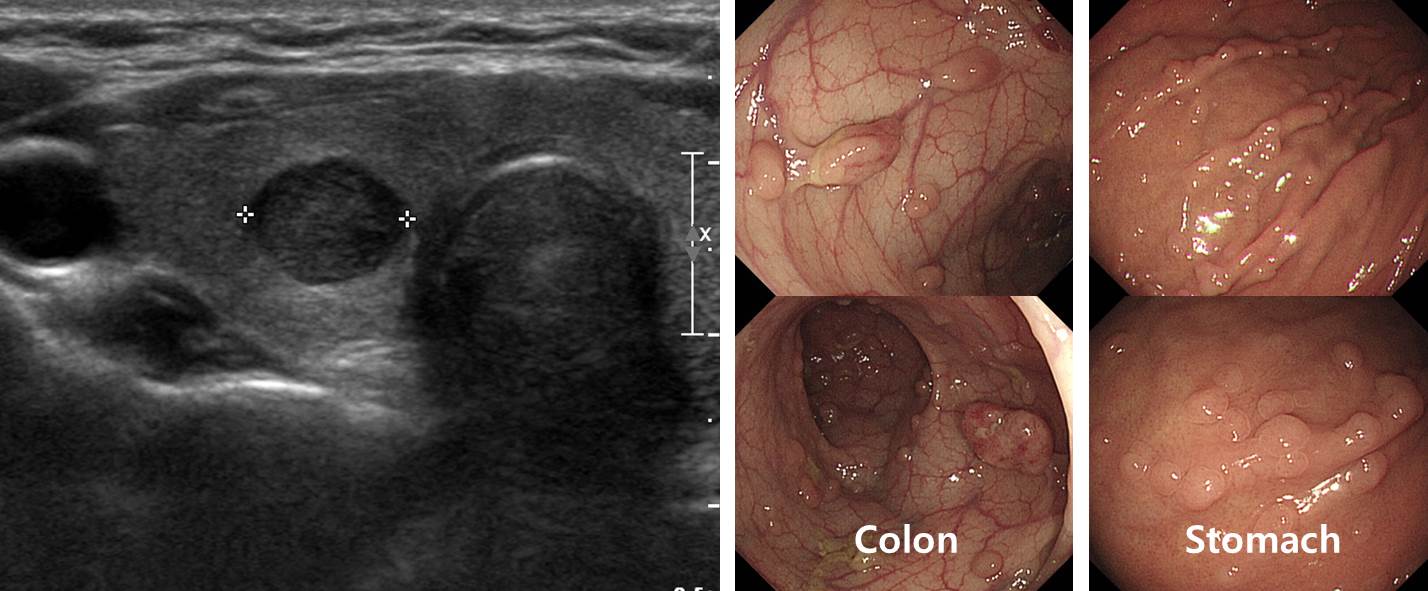
갑상선암으로 수술 후 대장 검사를 통하여 FAP로 확진된 환자입니다. 병리 결과는 아래와 같습니다.
Thyroid gland, lymph node, total thyroidectomy with central(anterior compartment) neck dissection: Papillary carcinomas (x3):
1) Subtype: Cribriform-morular variant
2) Tumor location: Both lobes
3) Tumor size: 0.8x0.8x0.8cm (lower pole, right), 0.3x0.3x0.2cm (mid pole, left), 1.5x1.2x1.1cm (lower pole, left)
4) Lymph vessel invasion: Absent
5) Blood vessel invasion: Absent
6) Extrathyroid extension: Present (minimal)
7) Surgical margins: Negative
8) Tumor multicentricity: Present
9) Lymph nodes ; No regional lymph node metastasis (0/2: "right central LN", 0/1; "left central LN", 0/1)
10) Other pathology: None
11) Parathyroid glands: No
12) pT1b N0
β-catenin: Positive in tumor cells
p27: Positive (1+, 5%)
Cyclin D1: Positive (2+, 25%)
Note: This tumor is associated with germline mutations in APC gene (e.q, familial adenomatous polyposis) although rarely associated with somatic mutations. Clinical work up is recommended.
그 많은 갑상선암 환자 중 왜 이 환자만 FAP 검사를 했을까요? 갑상선암의 병리학적 특성 때문이었습니다. Cribriform-morular variant는 FAP와 동반되는 경우가 많다고 잘 알려진 병입니다. 이 환자는 병리과에서 FAP 가능성을 언급하였고, 내과에서 이를 확인한 경우입니다. 아래 문헌을 참고하시기 바랍니다.
*참고: Cribriform-morular variant of papillary thyroid carcinoma: a distinctive type of thyroid cancer.
The aim of this systematic review is to study the features of cribriform-morular variant of papillary thyroid carcinoma (CMV-PTC) by analysing the 129 documented cases in the English literature. The disease occurred almost exclusively in women. The median age of presentation for CMV-PTC was 24 years. Slightly over half of the patients with CMV-PTC had familial adenomatous polyposis (FAP). CMV-PTC presented before the colonic manifestations in approximately half of the patients with FAP. Patients with FAP often have multifocal tumours in the thyroid. Microscopic examination of CMV-PTC revealed predominately cribriform and morular pattern of cancer cells with characteristic nuclear features of papillary thyroid carcinoma. Psammoma body is rare. On immunohistochemical studies, β-catenin is diffusely positive in CMV-PTC. The morular cells in CMV-PTC are strongly positive for CD10, bcl-2 and E-cadherin. Pre-operative diagnosis of CMV-PTC by fine-needle aspiration biopsy could be aided by cribriform architecture, epithelial morules and β-catenin immunostaining. Mutations of APC gene are found in the patients with CMV-PTC associated with FAP. In addition, mutations in CTNNB1, RET/PTC rearrangement and PI3K3CA mutations have been reported. BRAF mutation is negative in all CMV-PTC tested. Compared to conventional papillary thyroid carcinoma, CMV-PTC had a lower frequency of lymph node metastases at presentation (12%) and distant metastases (3%) as well as lower recurrence rates (8.5%) and patients' mortality rates (2%). To conclude, patients with CMV-PTC have distinctive clinical, pathological and molecular profiles when compared to conventional papillary thyroid carcinoma.
[질문] Cribriform-morular variant인 thyroid papillary cancer에서는 FAP를 의심해야 하는 것은 잘 알겠습니다. 그렇다면 FAP 환자에서 발생하는 thyroid cancer 중 cribriform-morular variant의 비중은 어느 정도입니까?
[답변] FAP 환자의 갑상선암에 대한 최근 큰 규모의 연구 결과입니다 (J Clin Endocrinol Metab 2016). 11명 중 8명이 Cribriform-morular variant였습니다.
Results: Twenty-one patients (16.3%) had solid nodules, and 24 patients (18.6%) had benign cystic nodules. In total, PTC was found in 11 patients (16% of the women and 0%of the men), 8 of which were CMV-PTC and the rest were classical PTC. In 17 female patients with thyroid nodules, CMV-PTC occurred in 8 of 9 patients who were 35 years age or younger but in none of the 8 patients who were older than 35 (P .0004 by Fisher’s exact test). The APC germline mutations in 8 patients with CMV-PTC were present at the 5 side of the profuse type of FAP region (codons 1249-1330).
Conclusions: The prevalence of CMV-PTC in FAP patients was higher than previously reported and this type of tumor was found preferentially in younger (under age 35) female patients with FAP.
* 참고: EndoTODAY 가족성 선종성 용종증 FAP
대한항공 의무실에서 발표한 흥미로운 자료입니다. 95회 비행 당 1건의 환자가 발생하고 있는데, 실신 (21%) 다음으로 소화기계 증상(18%)이 많았습니다. 기내 사망 사건은 2017년에 4건이었고 그 중 한 명은 원인 미상이었습니다. 1031건 중 항공기 회항은 5건이었습니다.
'만성 위염전'의 드문 증례입니다. EndoTODAY에서도 gastric volvulus와 diaphragmatic evantration을 소개한 바 있으니 참고하시기 바랍니다.
Foreign body에 의한 식도 actinomycosis 증례입니다. 목요내시경집담회에서 actinomycosis 증례를 논의한 바 있으니 참고하시기 바랍니다.
피부 전이로 진단되 직장의 반지세포암 1예
Pyogenic liver abscess로 인한 hepatogastric fistula
Malignant mesothelioma of peritoneum (tuberculous peironitis와 구분이 어려웠던 경우)
![]() [Pictures]
[Pictures]
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.