 EndoTODAY ГЛНУАц БГНЧ
EndoTODAY ГЛНУАц БГНЧ
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [РЇОЯ 132]
[РЇОЯ 132]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
РЇНФЕЕСЂЧеКЮОЯ СѕЗЪИІ НФЕЕОЯРЮСі РЇОЯРЮСі БИКаЧЯБтДТ НБСі ОЪНРДЯДй. ОЦЗЁ СѕЗЪДТ НФЕЕОЯРЯБюПф, РЇОЯРЯБюПф?
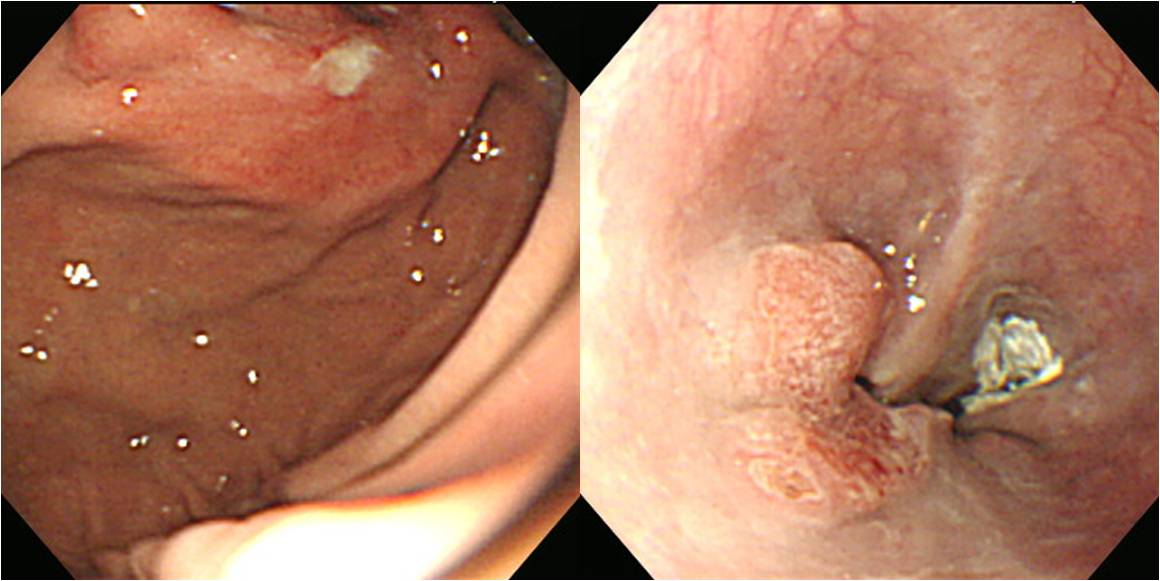
Advanced gastric carcinoma
1. Location : [2] esophagus, [1] upper third, distal esophagus and gastroesophageal junction
2. Gross type : Borrmann type 3
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size : 3.5x3.2x1.6 cm
6. Depth of invasion : extension to adventina of esophagus and subserosa of stomach
7. Resection margin: free from carcinoma
8. Lymph node metastasis : metastasis to 4 out of 23 regional lymph nodes
9. Lymphatic invasion : present
10.Venous invasion : not identified
11.Perineural invasion : present
РњДТ РЇОЯРИЗЮ КаЗљЧЯПДНРДЯДй. СООчРЧ СпНЩРЬ НФЕЕКИДйДТ РЇТЪРЬОњАэ, Barrett НФЕЕ КЮКаЕЕ АќТћЕЧСі ОЪОвНРДЯДй.
![]() 2009Гт 6Пљ 16РЯ EndoTODAYИІ ПХБщДЯДй.
2009Гт 6Пљ 16РЯ EndoTODAYИІ ПХБщДЯДй.

Esophagogastric junction cancerРЧ АцПь РЇОЯРЮСі НФЕЕОЯРЮСіИІ ЦЧДмЧЯДТ АЭРК БзДйСі АЃДмЧб РЯРЬ ОЦДеДЯДй. КДМвАЁ РлРИИщ КДМв СпНЩРЧ РЇФЁИІ КИАэ ДыА ЦЧДмЧв Мі РжСіИИ, КДРЬ ФПСіИщ ЕЕДыУМ ОюЕ№М НУРлЧб АЭРЮСіИІ ОЫБт ОюЗЦНРДЯДй. Barrett esophagusАЁ ОјДј НУР§ПЁДТ squamous cell carcinomaИщ НФЕЕОЯРЬАэ adenocarcinomaИщ РЇОЯРЬЖѓАэ ДмМјШї Л§АЂЧв Мі РжОњНРДЯДй. БзЗЏГЊ УжБйПЁДТ Barrett esophagusАЁ СѕАЁЧЯАэ РжБт ЖЇЙЎПЁ adenocarcinomaАЁ ГЊПТДйАэ ЧЯДѕЖѓЕЕ РЇОЯРЬЖѓАэ РхДуЧЯБт ОюЗСПю СіАцРЬ ЕЧОњНРДЯДй.
ЙнДыЗЮ squamous cell carcinomaАЁ ГЊПРИщ НФЕЕОЯРИЗЮ ЦЧДмЧв Мі ЙлПЁ ОјНРДЯДй. ОЦСї stomach mucosaРЧ squamous metaplasiaДТ ОЫЗССЎ РжСі ОЪБт ЖЇЙЎРдДЯДй. ПРДУРЧ СѕЗЪДТ squamous cell carcinomaЗЮ ГЊПдБт ЖЇЙЎПЁ НФЕЕОЯРК ЦВИВОјДйАэ Л§АЂЧв Мі РжОњНРДЯДй (Invasive squamous cell carcinoma, well differentiated; 1) tumor size: 6.5x5x2.5cm, 2) extension to perimuscular adventitia, 3) no metastasis in 56 regional lymph nodes ). БзЗЏГЊ КДМвРЧ СпНЩРК esophagogastric junction КИДй ЧЯЙцПЁ РЇФЁЧЯАэ РжОњНРДЯДй.
КДМвРЧ СпНЩРИЗЮ НФЕЕОЯАњ РЇОЯРЛ ГЊДЉДТ АЭРЬ ОѓИЖГЊ ЧуИСЧб АЭРгРЛ КИПЉСжДТ СѕЗЪАЁ ОЦДв Мі ОјНРДЯДй.
![]() © 2014-11-25. РЬСиЧр
© 2014-11-25. РЬСиЧр