 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [위암 134]
[위암 134]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
위식도접합부암의 수술 원칙은 명확하지 않습니다. 외과쪽에서는 total gastrectomy를, 흉부외과쪽에서는 total gastrectomy 혹은 Ivor-Lewis 수술을 선호하는 것 같습니다.
제 생각은 병소가 식도를 거의 침윤하지 않았으면 total gastrectomy를 하고, 식도를 많이 침윤하고 있으면 Ivor-Lewis 수술을 하면서 위를 상당부분 절제하거나, total gastrectomy를 하면서 distal esophagectomy를 더하는 것이 좋을 것 같습니다. 광범위한 림프절 절제는 말할 필요도 없습니다.
Ivor-Lewis 수술일 시행되었던 위식도접합부암 증례입니다.
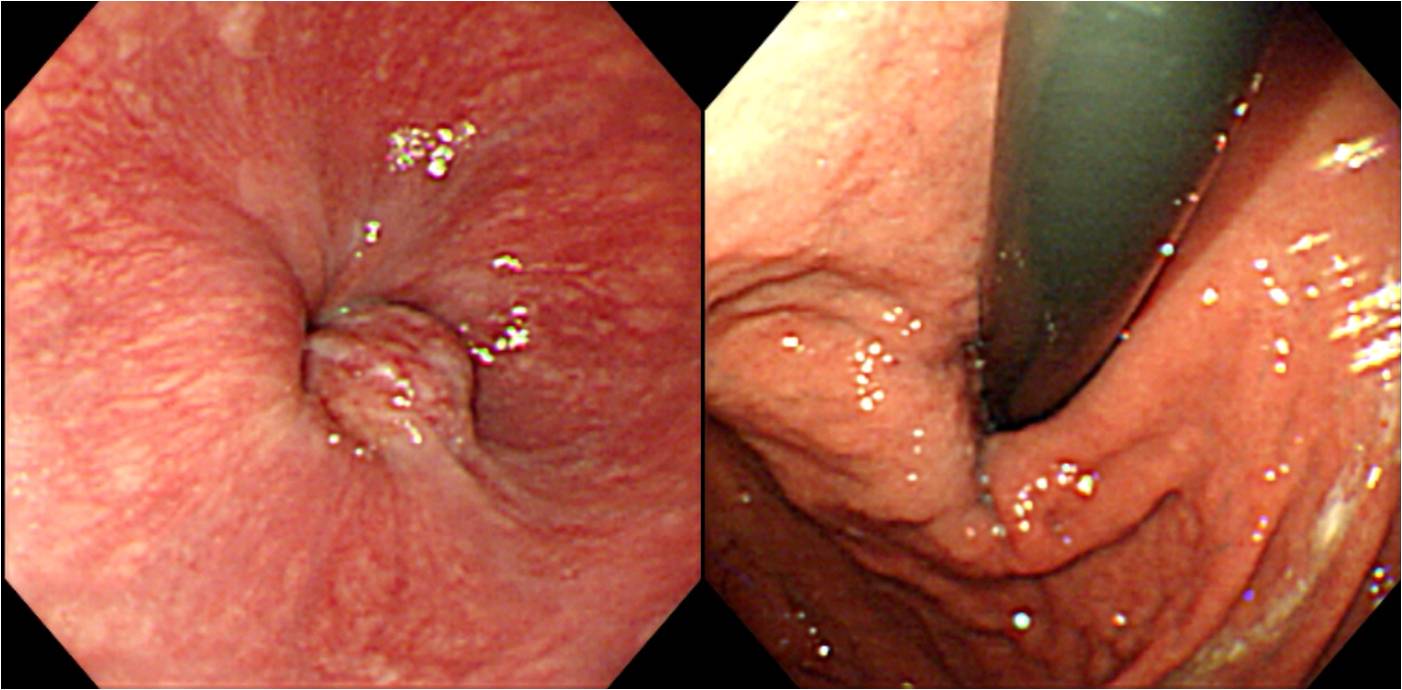

Advanced gastric carcinoma, Borrmann type II,
Adenocarcinoma, moderately differentiated, cardia and gastroesophageal junction;
1) tumor size: 4x4 cm
2) extension to adventitia and subserosa
3) endolymphatic tumor emboli: present
4) negative resection margins (proximal: 10 cm; distal: 8 cm)
5) metastasis to 5 out of 49 regional lymph nodes
![]() © 2014-11-25. 이준행
© 2014-11-25. 이준행