 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 425]
[Gastric cancer 425]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
조직검사에서 M/D adenocarcinoma가 나와 ESD를 위하여 의뢰된 분입니다. 그런데 시술 결과 28밀리 미분화 혼재암이고 절제변연이 4 방향 중 3 방향에서 양성이었습니다.
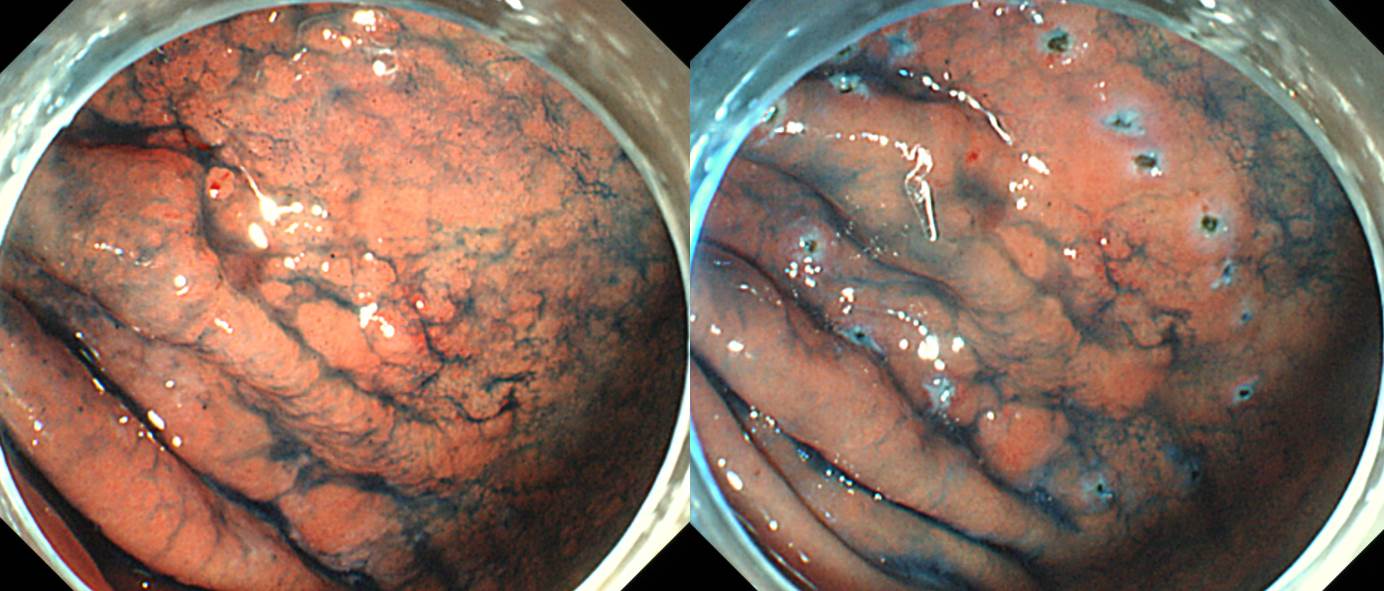
Early gastric carcinoma
1. Location : body, anterior wall
2. Gross type : EGC type IIb+IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated > signet ring cell carcinoma(30%)
4. Histologic type by Lauren : mixed
5. Size of carcinoma : (1) longest diameter, 28 mm (2) vertical diameter, 24 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : proximal, distal and posterior resection margins involved by carcinoma, safety margin : anterior 10 mm
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: present
환자에게는 아래와 같이 설명드렸습니다.
비교적 작은 조기위암으로 판단되어 85% 정도의 초기성공률 (내시경치료만으로 일차 치료가 끝나는 비율)을 예측하는 상황에서 내시경치료를 하였는데, 아쉽게도 그 85%에 들지 못하고 수술이 필요한 15%에 해당하는 결과가 나왔습니다. 내시경으로 절제한 표본에 대한 최종 병리결과에서 세포형, 깊이, 범위, 림프관/혈관에 모두 문제가 없어야 하는데 아쉽게도 문제가 있는 것으로 나왔습니다. 즉 수술이 필요한 것으로 나왔습니다. 이런 분들이 약 15%정도 됩니다.
환자분에서 문제가 되는 것은 두 가지 입니다. (1) 세포형이 적절하지 않았습니다. 분화형으로 나와야 하는데 분화형과 미분화형이 섞여 있는 혼재암으로 나왔습니다. (2) 혼재암인 경우에 자주 발생하는 문제인데요... 절제 변연에 암이 닿아 있었습니다. 즉 일정 부분 여분을 두고 절제가 되어야 하는데 혼재암인 경우 병소의 경계가 모호하여 최대한 절제하여도 절제 변연이 부족하게 나오는 경우가 많습니다.
병리결과에 문제가 없을 때 재발률이 5% 정도인데 반하여, 현재의 재발 위험은 10-20% 이상입니다. 만약 재발하면 절반 이상은 완치의 기회가 없습니다 .따라서 수술이 경과관찰보다 유리한 상황입니다. 물론 수술은 수술입니다. 전신마취에 따른 위험, 통증, 수술의 합병증, 수술 후 삶의 질 저하 등의 어려운 점이 있지만 그래도 재발위험을 더 많이 고려해야 한다고 판단됩니다. 수술을 해보면 눈에 보일 정도의 암이 남아있는 경우도 있고 그렇지 않는 경우도 있습니다. 이러한 내용을 모두 종합하여 판단할 때 수술을 권하고 싶습니다.
외과 선생님을 뵙고 일정과 수술에 대하여 상의하시기 바랍니다. 제가 미리 설명해 두었습니다.
수술을 하였고 residual tumor가 있었습니다.
Stomach, subtotal gastrectomy:
Status post endoscopic submucosal dissection
Early gastric carcinoma, residual
1. Location : middle third, Center at body, anterior wall
2. Gross type : EGC type IIb
3. Histologic type : signet-ring cell carcinoma, residual
4. Histologic type by Lauren : diffuse
5. Size : 1.1x1 cm, residual
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin: free from carcinoma, safety margin: proximal 2.1 cm, distal 9 cm
8. Lymph node metastasis : no metastasis in 34 regional lymph nodes (pN0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
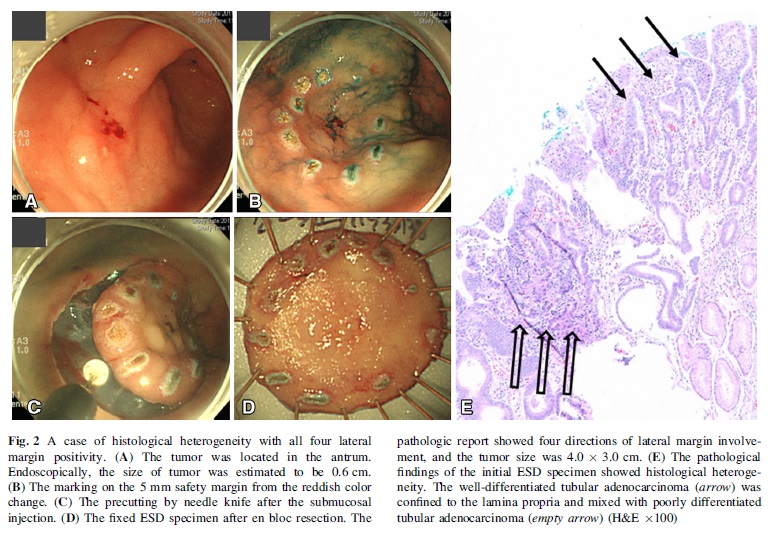
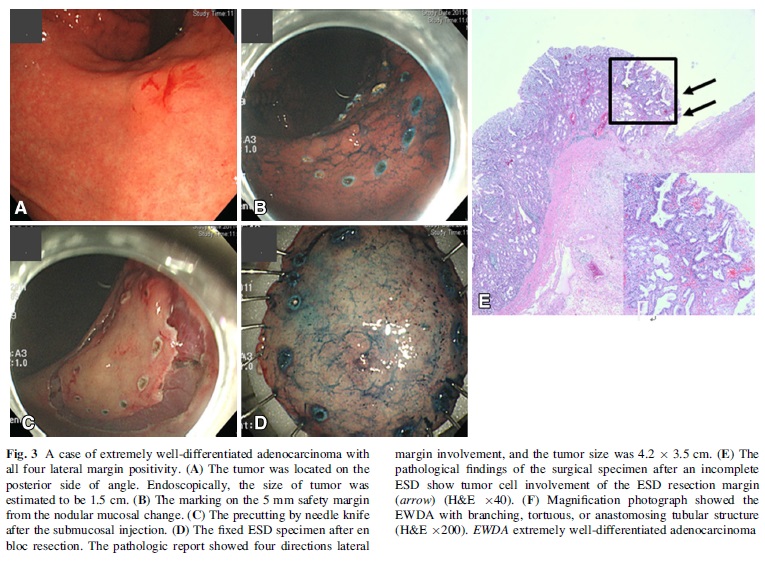
조기위암 ESD 후 절제변연 양성은 5.5% 정도입니다. 이 중 다발성 양성인 경우는 대부분 뭔가의 이유가 있습니다. 저희의 분석(Lee JH. Surg Endosc 2015)에 의하면 histologic heterogeneity (EndoTODAY 20121122) 혹은 EWDA (extremely well differentiated adenocarcinoma) (EndoTODAY 20121123)에서 multiple lateral margin involvement가 많았습니다. 과거에 한번 소개한 바 있지만 다시 옮깁니다.
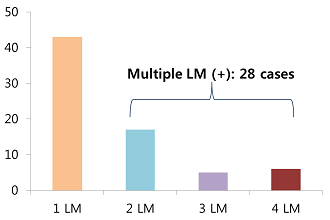
In our institution, lateral margin involvement is evaluated and reported in 4 directions. In about 14 hundred early gastric cancers treated by ESD, lateral margin involvement was documented in 5.5%. Among them, 60% were single lateral margin positive. 40% were multiple lateral margin positive.
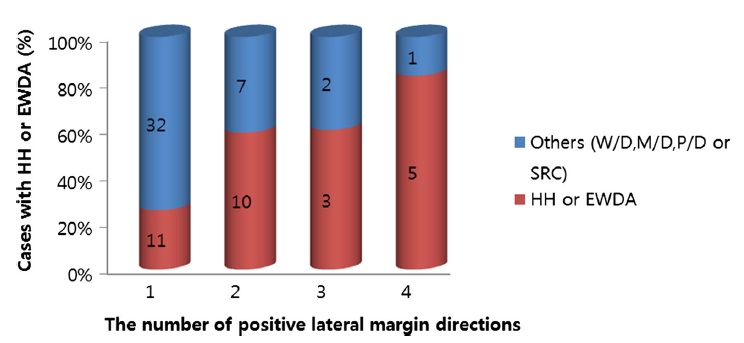
Histologic heterogeneity was seen in 25% and 46%, respectively. Extremely well differentiated adenocarcinoma was 7% and 25% in the two groups. This difference was statistically significant. Cases of technical difficulty was the same in the two groups. Surprisingly, the procedure time was shorter in the multiple lateral margin positive group. We thought that the technical aspect was not related to the number of positive lateral margin.

In this figure, yellow bar is the proportion of the cases with HH or EWDA. It showed that the ratio of HH or EWDA is increasing according to the number of lateral margin positive direction. And the difference was statistically significant.
결국 histologic heterogeneity (EndoTODAY 20121122) 혹은 EWDA (extremely well differentiated adenocarcinoma) (EndoTODAY 20121123)에서 multiple lateral margin involvement가 많았다는 것입니다. 가벼운 마음으로 아주 쉽게 ESD를 한 후 multiple lateral margin이 나오는 것인데 임상가로서는 상당히 당황스러운 일입니다.
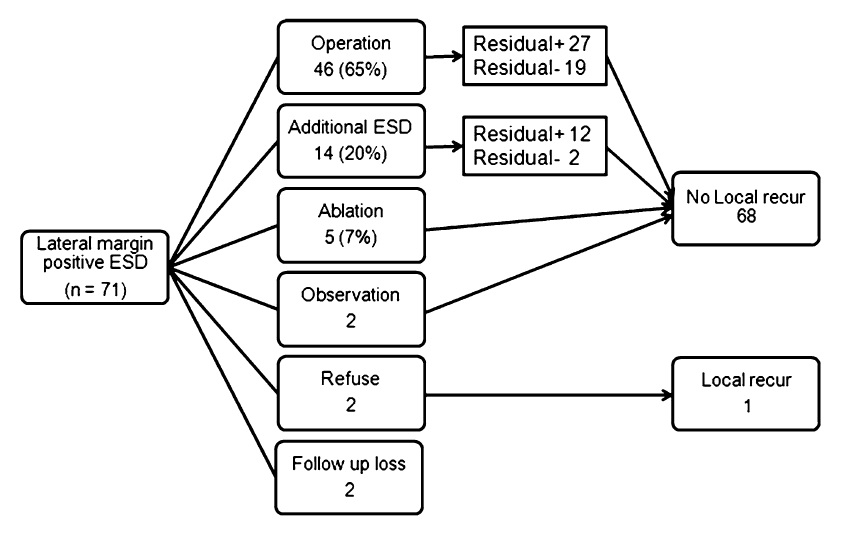
치료 성적입니다. 치료를 받지 않은 환자 1명만 국소재발을 보였고 다른 환자들은 다양한 방법으로 잘 치료되었습니다.
* 참고: EndoTODAY 절제 변연 양성
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.