EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 773. EGC, superficial spreading type]
[Gastric cancer 773. EGC, superficial spreading type]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
Early gastric cancer of superficial spreading type is relatively rare. It is included in the expanded criterial of the ESD, but most cases are usually treated by surgery.
Stomach, radical total gastrectomy: Early gastric carcinoma
1. Location : middle third, Center at body and anterior wall
2. Gross type : EGC type IIa+IIb
3. Histologic type : tubular adenocarcinoma, mixed well and poorly differentiated (WHYX type)
4. Histologic type by Lauren : mixed
5. Size : 7.5x5.5 cm
6. Depth of invasion : invades mucosa (muscularis mucosae) (pT1a)
7. Resection margin: free from carcinoma, safety margin: proximal 2.0 cm, distal 9.0 cm
8. Lymph node metastasis : no metastasis in 19 regional lymph nodes (pN0) (0/19: "2", 0/1; "3", 0/4; "4", 0/4; "5", 0/0; "6", 0/4; "7", 0/1; "9", 0/1; "8a", 0/1; "11p", 0/0; "12a", 0/3; "4sb", 0/0; "1", 0/0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. AJCC stage by 8th edition: pT1a N0
Lee KJ et al (Yonsei University) reported Investigation of Endoscopic and Pathologic Features for Safe Endoscopic Treatment of Superficial Spreading Early Gastric Cancer in 2016. In this report, they mentioned that "in mucosal cancer without ulcers, tumors >= 6 cm had a higher rate of lymph node metastasis than tumors <= 2 cm; however, this trend was not significant (7.7% vs 5.3%, P=0.455)", but I am so worrisome. You can refer to my publication in 2010 (Scand J Gastroenterol 2010). I usually recommend surgery for any lesions larger than 5cm.
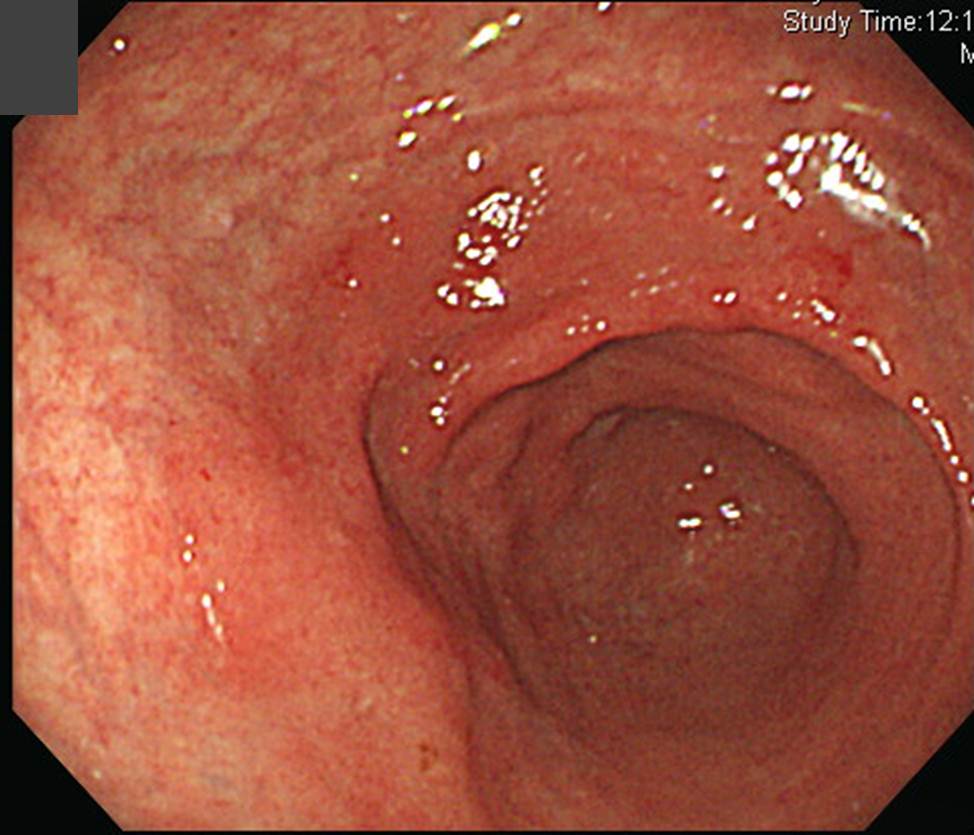
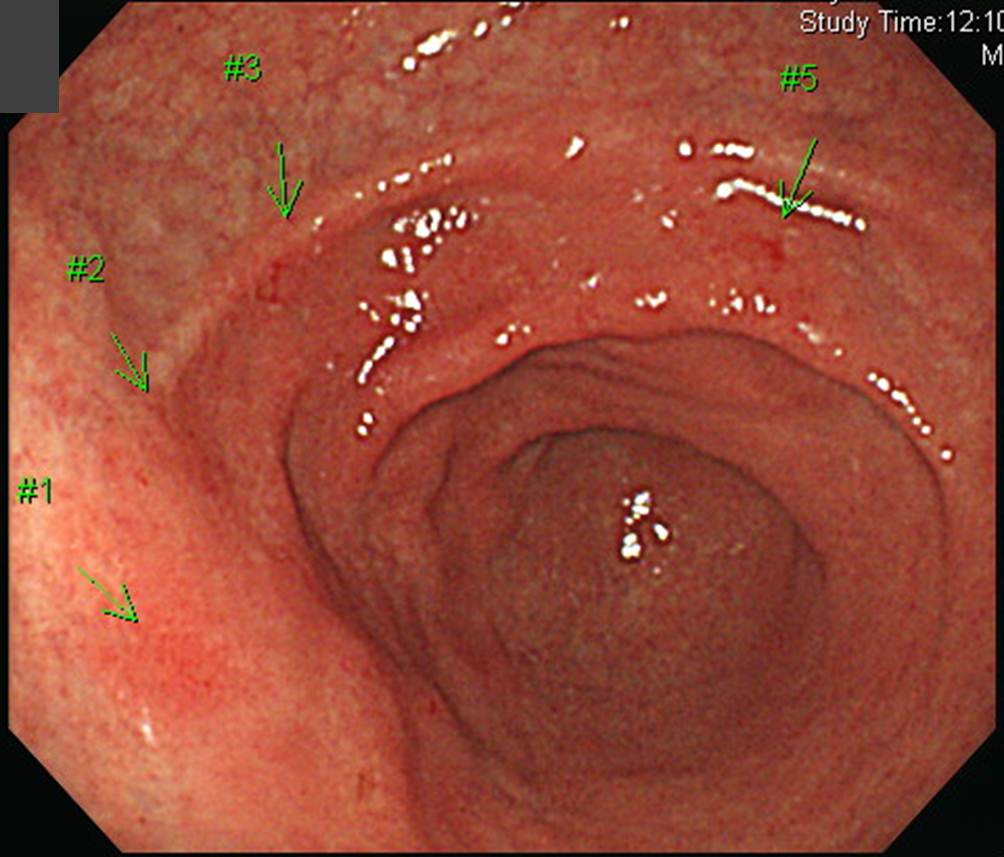
Below is another case of superficial spreading type EGC with very unclear border.
Multiple endoscopic biopsies were done and the biopsy results (#1 - #5) were all poorly differentiated adenocarcinoma.
Subtotal gastrectomy was done.
Early gastric carcinoma :
1. Location : lower third center at antrum and lesser curvature
2. Gross type : EGC type IIb
3. Histologic type : tubular adenocarcinoma, poorly differentiated
4. Histologic type by Lauren : intestinal
5. Size : 7.5x3.0 cm
6. Depth of invasion : extension to mucosa (muscularis mucosa) (pT1a)
7. Resection margin: free from carcinoma, safety margin: proximal, 8.5 cm; distal, 1.5 cm
8. Lymph node metastasis : no metastasis in 20 regional lymph nodes (pN0)
9. Lymphatic invasion : not identified
10.Venous invasion : not identified
11.Perineural invasion : not identified
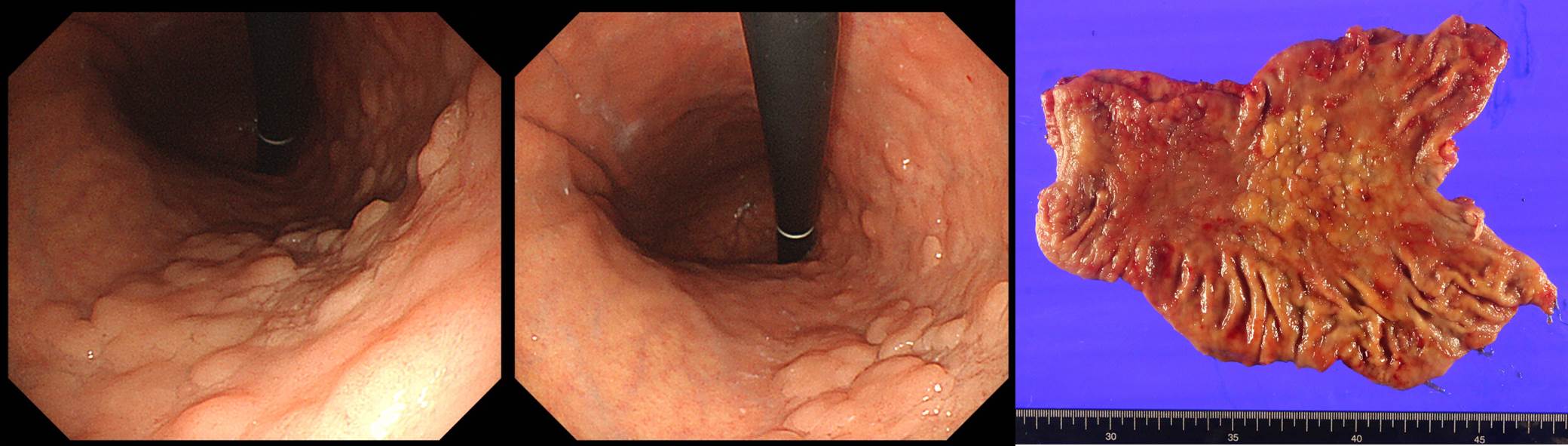
In the following case, there was an ulcer at the posterior all aspect of the angle. In addition, two small ulcerative lesions were found at the lesser curvature of the gastric body. However, intervening mucosal surface was uneven. Biopsies for three depressed lesions were all cancers. Surgery was done

Stomach, subtotal gastrectomy: Early gastric carcinoma
1. Location : middle third, Center at body and lesser curvature
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, poorly (solid) differentiated with signet ring cell component (20%)
4. Histologic type by Lauren : mixed
5. Size : 9x5 cm
6. Depth of invasion : invades submucosa (SM1) (pT1b)
7. Resection margin: free from carcinoma, safety margin: proximal 2.5 cm, distal 5.5 cm
8. Lymph node metastasis : metastasis to 8 out of 57 regional lymph nodes (pN3a) (perinodal extension: absent) (8/57: "3", 6/13; "4", 0/7; "5", 0/1; "6", 0/11; "7", 0/3; "9", 2/10; "8a", 0/5; "11p", 0/2; "12a", 0/4; "4sb", 0/0; "1", 0/1)
9. Lymphatic invasion : present
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
13. AJCC stage by 7th edition: pT1b N3a
* EB virus (-), c-erbB-2 (-)
It was a single large early gastric cancer rather than three synchronous multiple cancers. Although the depth of invasion was superficial SM, but there were multiple lymph node metastasis including #9 celiac node.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2019-8-5)