EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 812. EGC (inter-observer variation in the pathology)]
[Gastric cancer 812. EGC (inter-observer variation in the pathology)]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
A patient with EGC was referred (pathology report: P/D adenocarcinoma). Based on the pathology report and unclear border of the lesion, initial plan was surgery. However, outside slide review and repeated biopsy at my hospital was all M/D adenocarcinoma.
55 year old male
After a long and careful discussion, the patient and I decided to do ESD.
ESD was done as usualy and the final pathology was excellent.
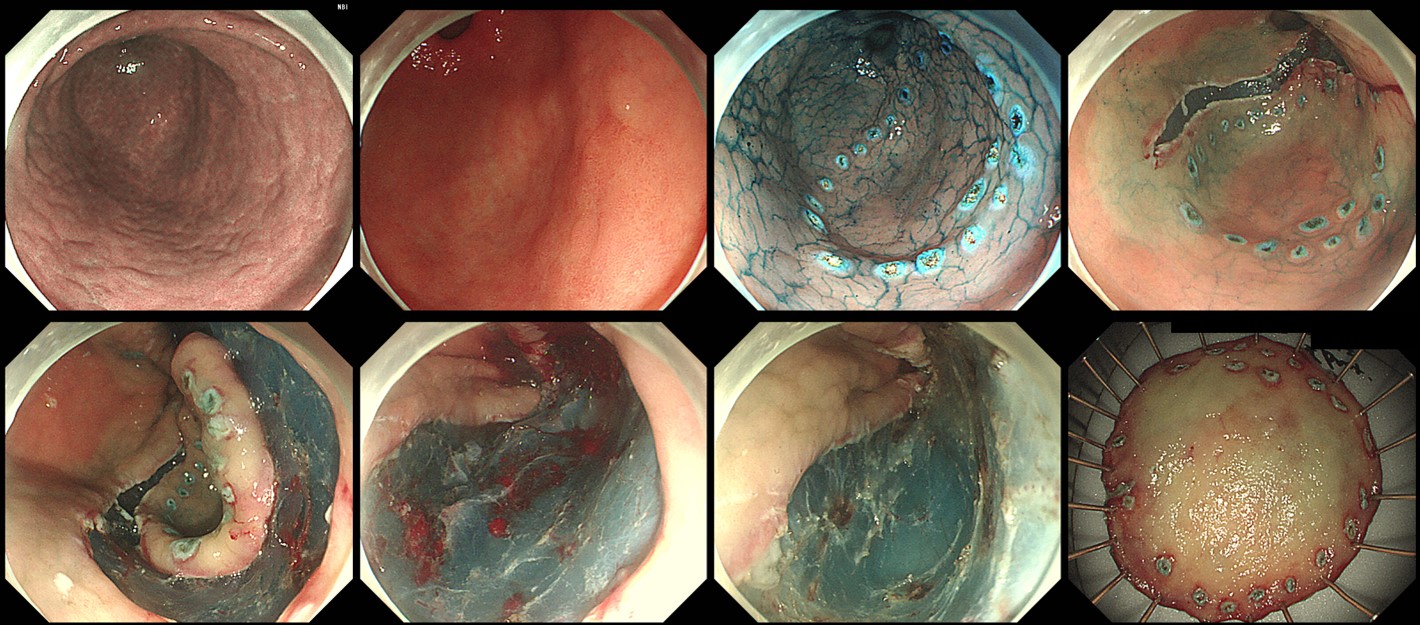
ESD; early gastric carcinoma
1. Location : distal antrum, postero-greater curvature
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated (WHYX type)
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 22 mm (2) vertical diameter, 21 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 7 mm, proximal 10 mm, anterior 12 mm, posterior 10 mm, deep 300
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
In addition to the standard PPI for 8 weeks, I added a short course of steroid for the prevention of stricture.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2019-11-25)