EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 815. ESD for EGC near the pyloric ring]
[Gastric cancer 815. ESD for EGC near the pyloric ring]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
EGC of the distal antrum abutting the pyloric ring is difficult to do ESD. If the retroflection is possible at the duodenal bulb, the retrograde approach can be tried. In many cases, however, duodenal retroflection is impossible. So, the antegrade approach should be done.
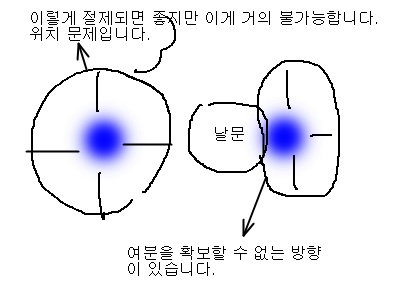
In the antegrade approach to the pyloring ring cancer, distal resection margin is alway worrisome. In the outpatient interview, I usually explain this point very carefully using the following cartoon.
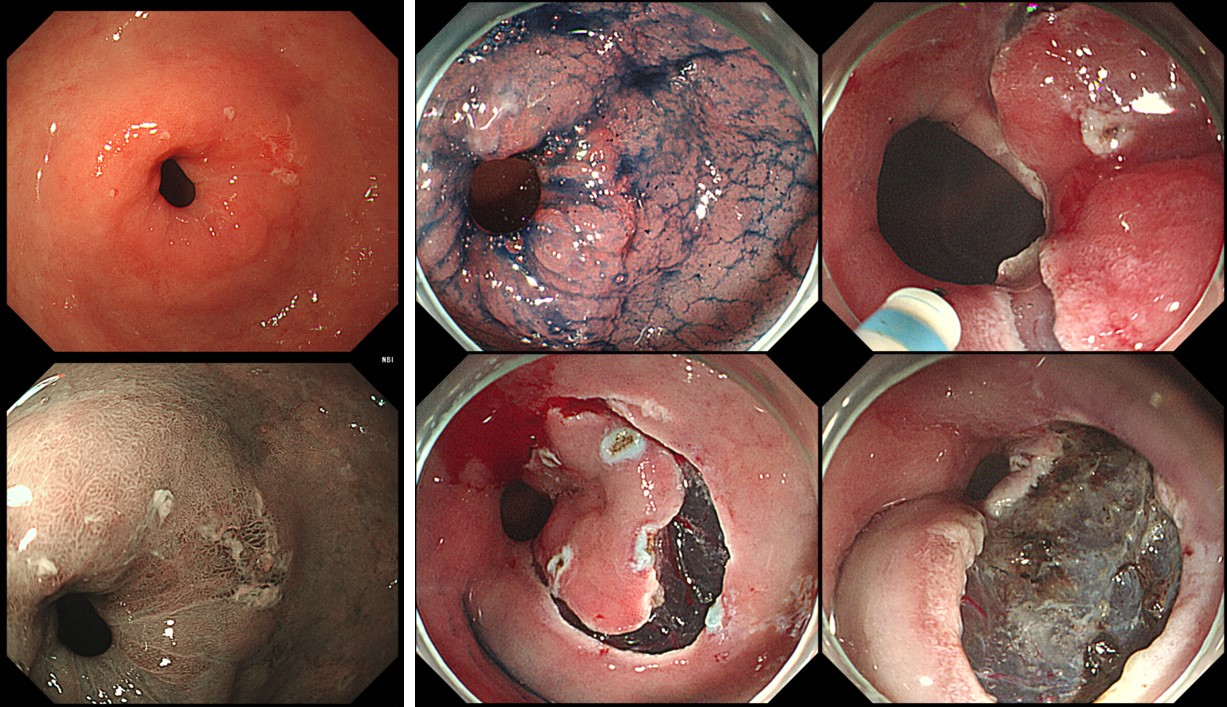
In the following case, retroflection in the duodenal bulb was impossible. After marking, distal precutting was done very carefully using the Dual knife. After finishing the circumferential precutting, submucosal dissection was done as usual.
The final pathology was acceptible. However, the distal resection margin was just 2 mm as expected.
ESD: Early gastric carcinoma
1. Location : pylorus
2. Gross type : EGC type IIa+IIc
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 10 mm (2) vertical diameter, 4 mm
6. Depth of invasion : invades mucosa (lamina propria) (pT1a)
7. Resection margin : free from carcinoma(N), safety margin : distal 2 mm, proximal 4 mm, anterior 4 mm, posterior 10 mm, deep 350
8. Lymphatic invasion : not identified(N)
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: absent
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2019-12-26)