EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 778. Borrmann type IV]
[Gastric cancer 778. Borrmann type IV]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
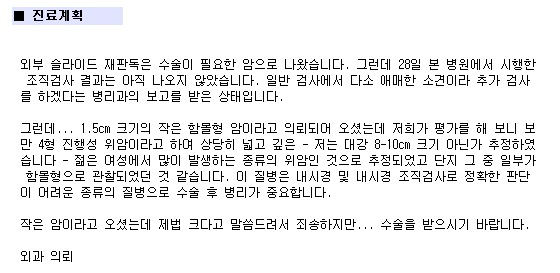
A young lady was referred due to a small depressed type cancer (1.5cm) detected in the screening endoscopy. The pathology was poorly cohesive carcinoma
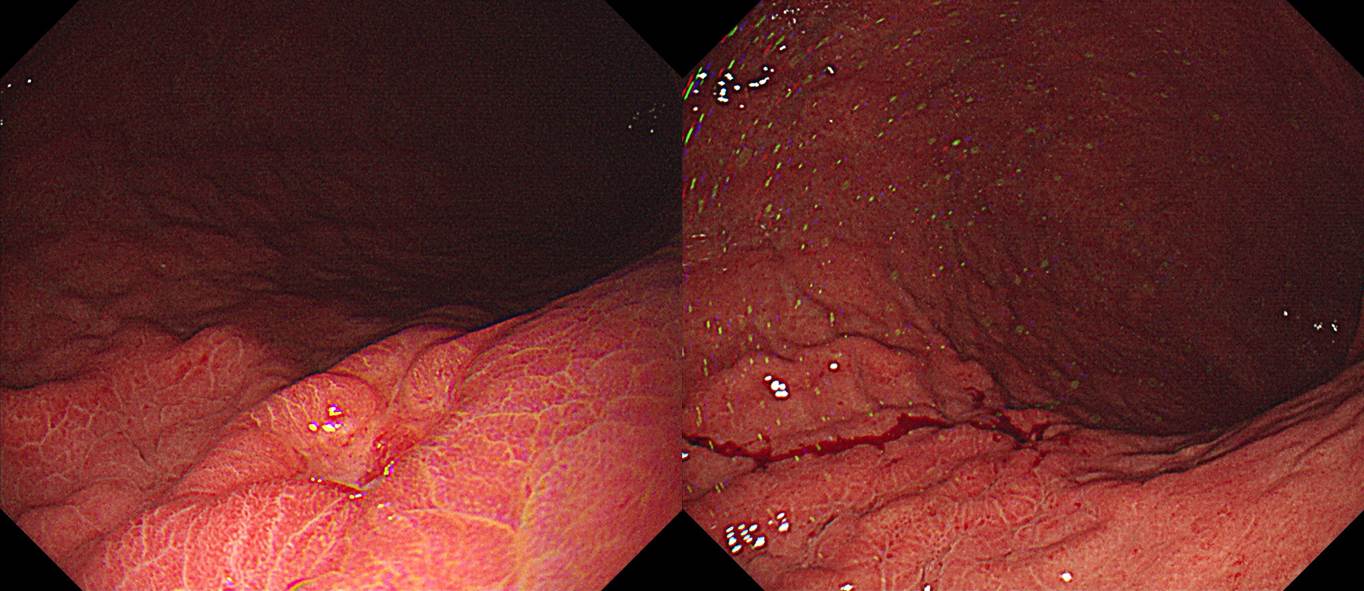
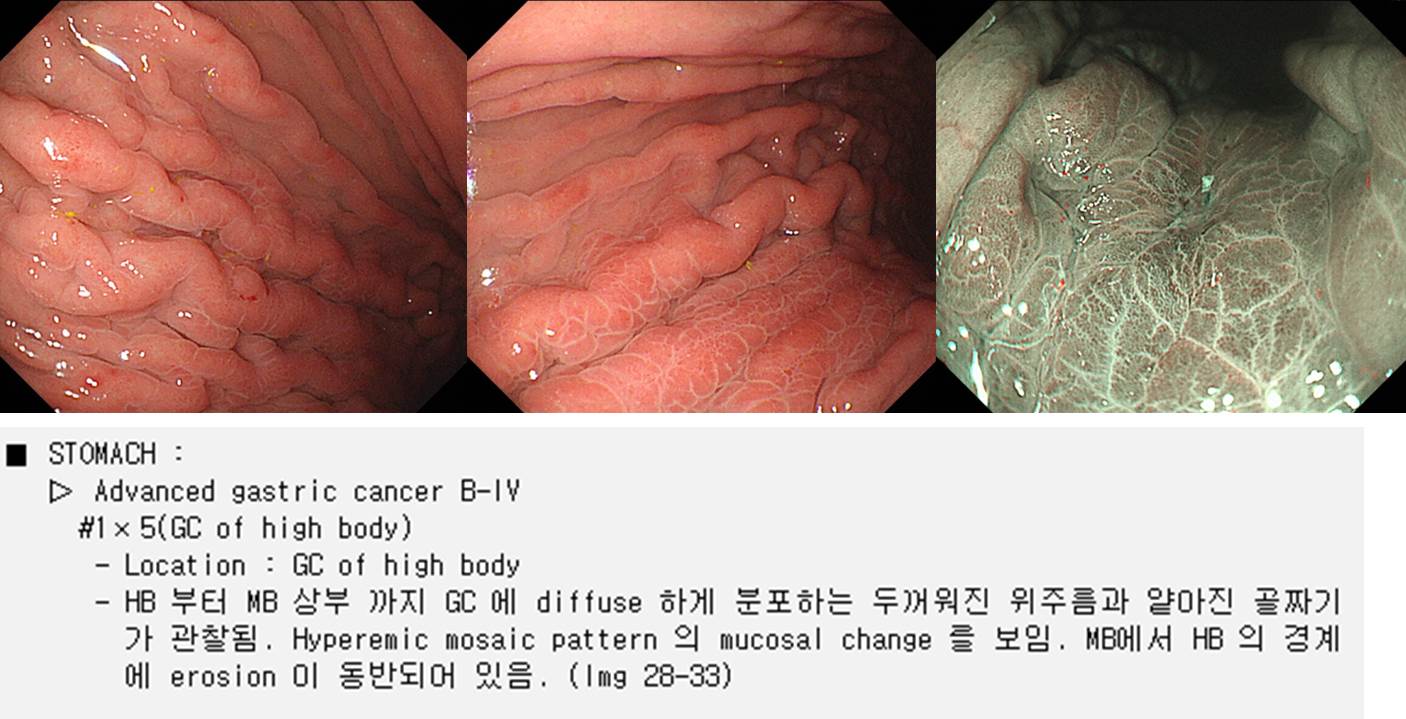
However, in the repeat endoscopy, the lesion was a large Borrmann type IV cancer with a small depressed lesion. The surface showed typical Mozaic pattern.
Total gastrectomy was done.
Stomach, radical total gastrectomy: Advanced gastric carcinoma
1. Location : upper third, Center at body and posterior wall
2. Gross type : Borrmann type 4 (scirrhous)
3. Histologic type : tubular adenocarcinoma, poorly (poorly cohesive) differentiated
4. Histologic type by Lauren : diffuse
5. Size : 9.0x5.0 cm
6. Depth of invasion : penetrates subserosal connective tissue (pT3)
7. Resection margin: free from carcinoma; safety margin: proximal 2.5 cm, distal 8.5 cm
8. Lymph node metastasis : no metastasis in 29 regional lymph nodes (pN0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
13. AJCC stage by 8th edition: pT3 N0
The endoscopy description was perfect except that it has no size measurement. In Borrmann type IV, exact size measurement is difficult. It is usually 10cm when the antrum was saved. As you can see the outpatient medical record, I explained to the patient that the tumor is about 8-10cm.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2019-8-10)