EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 784. Laparoscopic wedge resection for NET]
[Gastric cancer 784. Laparoscopic wedge resection for NET]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
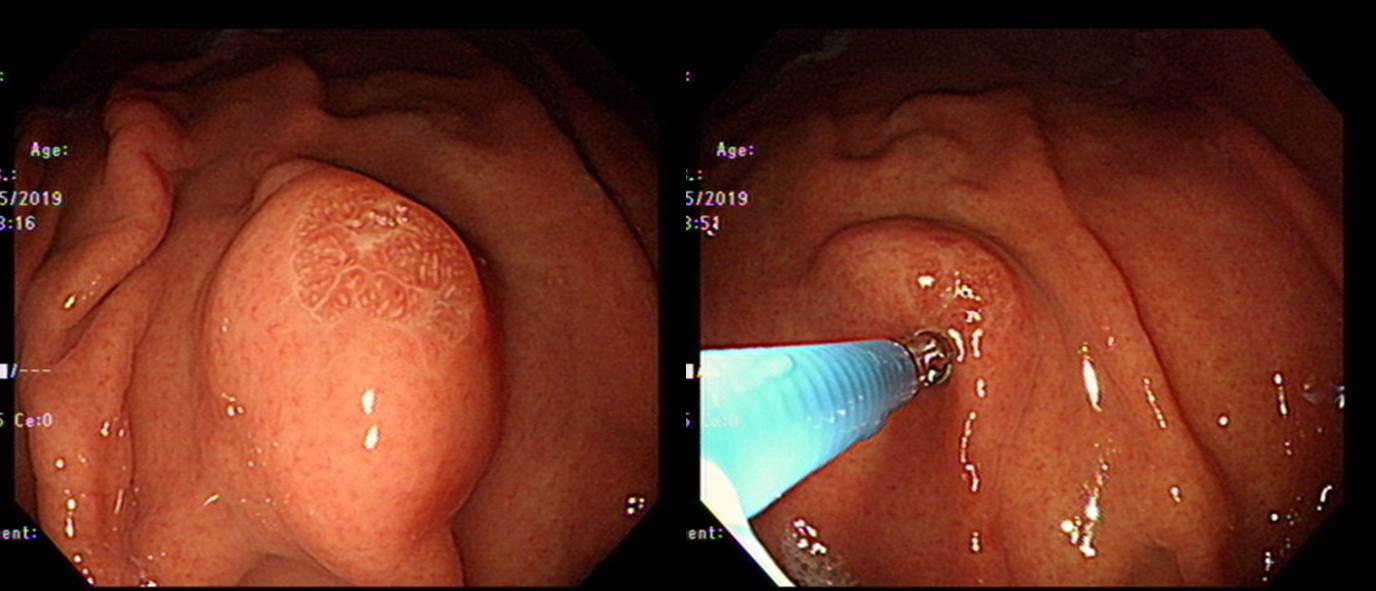
60 years old male was referred due to well differentiated neuroendocrine tumor (G1). The serum gastrin was normal (41.9). What would you recommend, surgery or endoscopic resection?
It looks like an SMT, which means a massive submucosal infiltration. I recommended laparoscopic resection.


Stomach, laparoscopic wedge resection: Well differentiated neuroendocrine tumor (CARCINOID) (G1)
1. Name of Procedure: laparoscopic wedge resection
2. Site of Tumor: Stomach (high body, greater curvature)
3. Diagnosis: Neuroendocrine tumor
4. WHO classification(2010): Well-differentiated Neuroendocrine tumor (G1)
5. Multiplicity: Single
6. Size: 1.7x1.5 cm
7. Extent: Mucosa and submucosa
8. Grading: Mitotic Count(/10HPF): 0-1, Ki-67 labeling index: G1: <3%
9. Immunohistochemical Stains:
1) Synaptophysin : Positive
2) Chromogranin A: Positive
10. Lymphovascular invasion: Not identified
11. Perineural invasion: Not identified
12. Lymph node metastasis: not evaluated
13. Resection Margins: Negative, Safety margin : 1.5 cm
Gastric carcinoids usually have submucosal invasion in resected specimen. When a NET looks like a small mucosal lesion (especially when serum gastrin is high), endoscopic resection can be tried. However, a big lesion (more than 1 cm) or an SMT-like lesion is usually treated by wedge resection. I am not sure whether lymph node dissection is required for a small NET.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2019-8-26)