EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 791. Multiple gastric cancers in the surgically resected specimen]
[Gastric cancer 791. Multiple gastric cancers in the surgically resected specimen]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
When a gastric cancer patient is referred for surgery, endoscopy is repeated for (1) detailed examination of the index cancer lesion, and (2) possible synchronous lesions. We carefully examine the proximal stomach, because this area is remained after the standard subtotal gastrectomy.
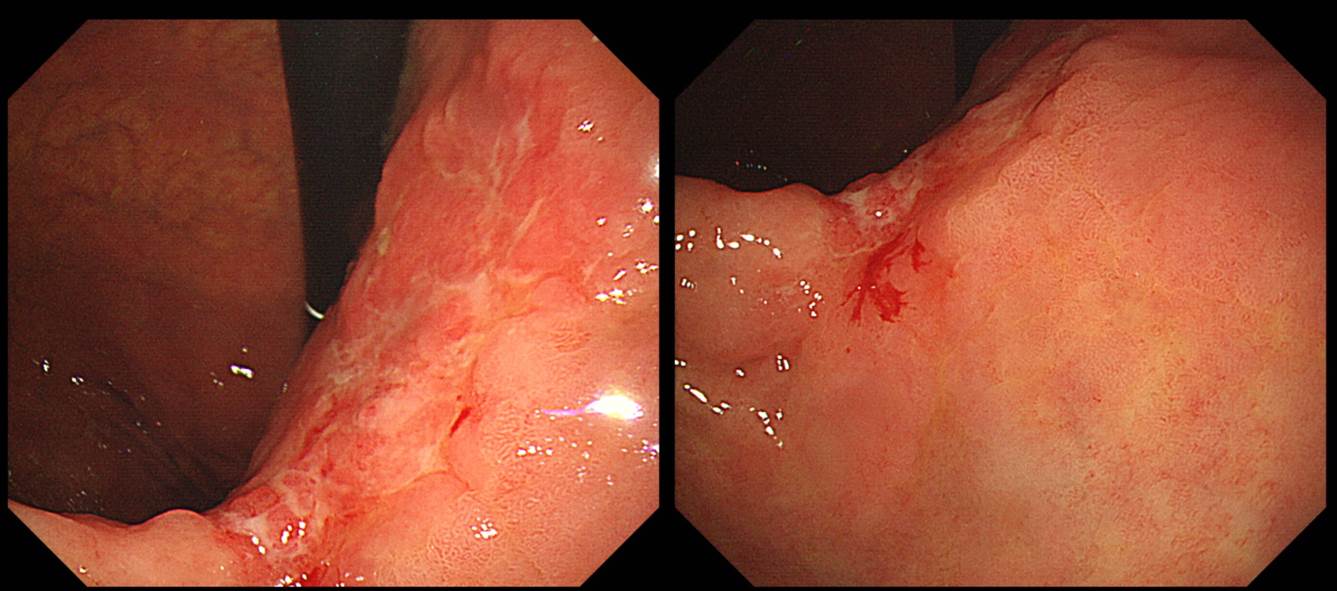
There was a cancer lesion at the posterior wall of the gastric angle. After repeating endoscopy, subtotal gastrectomy was done
The surgical pathology was surprising, because (1) there were two cancers in the resected specimen, (2) it was all EGCs, (3) there was a lymph node metastasis in the station #4.
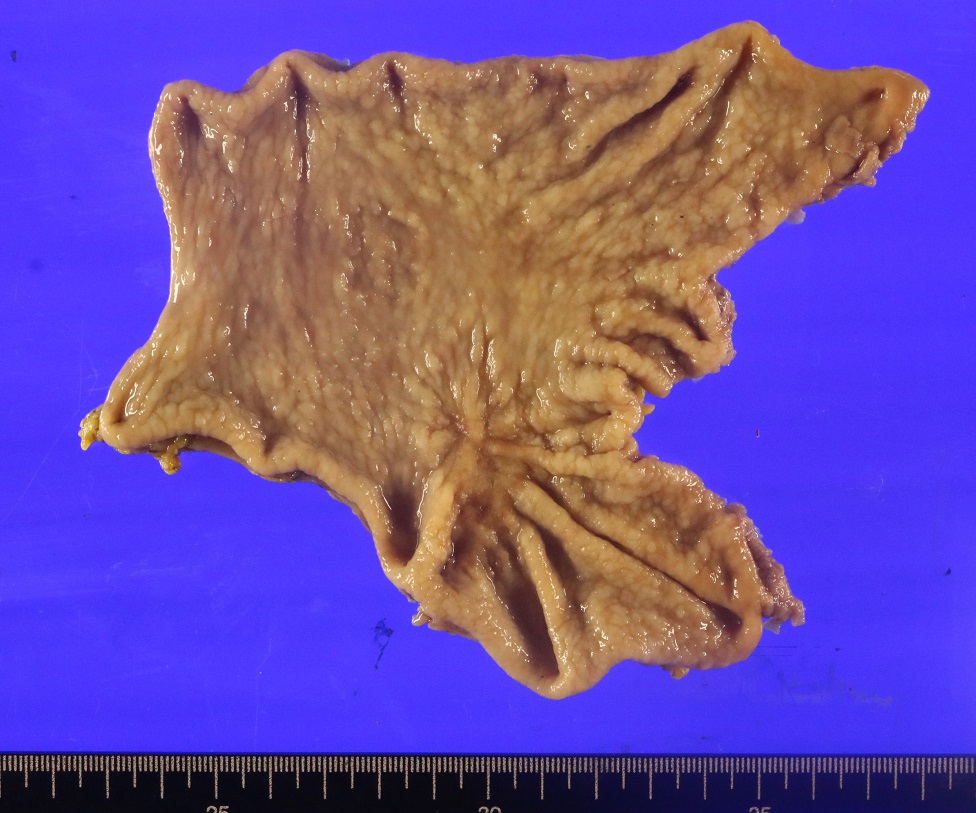
EGC, middle third, P/D (solid), 4.5x2.8 cm, SM3
EGC, lower third, W/D, 1.8x1.5 cm, MM
LN : metastasis to 1 out of 34 regional nodes
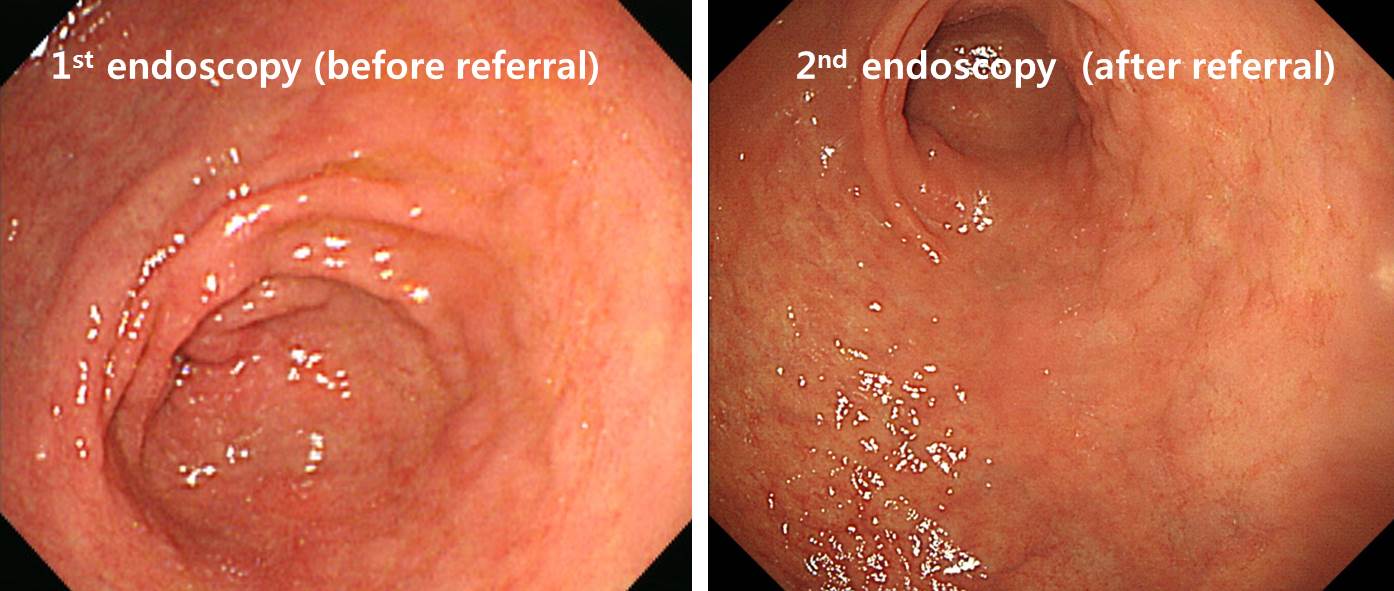
So, the 1.8cm sized mucosal cancer in the antrum was missed twice in the screening endoscopy and in the repeated endoscopy after referral. In the review of endoscopic images, cancer lesion was not clear in the antrum.
We should think about the possibility of synchronous cancer, especially before surgery.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2019-9-3)