EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 810. EGC type I of the pyloric ring with duodenal herniation]
[Gastric cancer 810. EGC type I of the pyloric ring with duodenal herniation]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
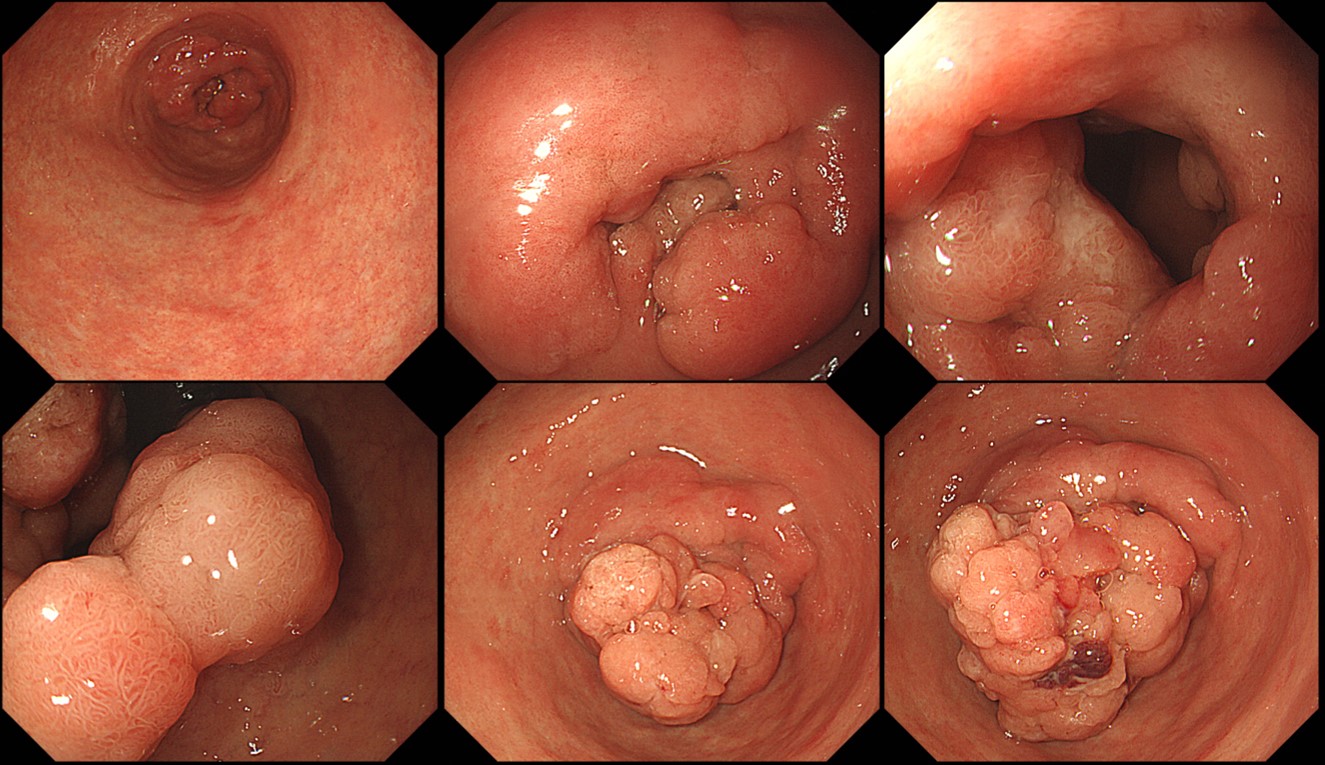
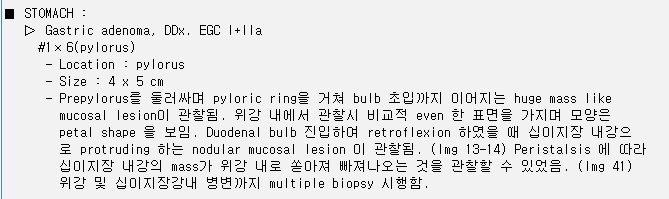
Mass lesion of the distal antrum or pylorus can partially and transiently herniate into the duodenal bulb.
At first it looked like a flat elevated lesion of the pyloric ring. But, a large protruded and herniated part of the tumor came out from the duodenum during the examination.
The forceps biopsy was well differentiated adenocarcinoma and surgery was done.
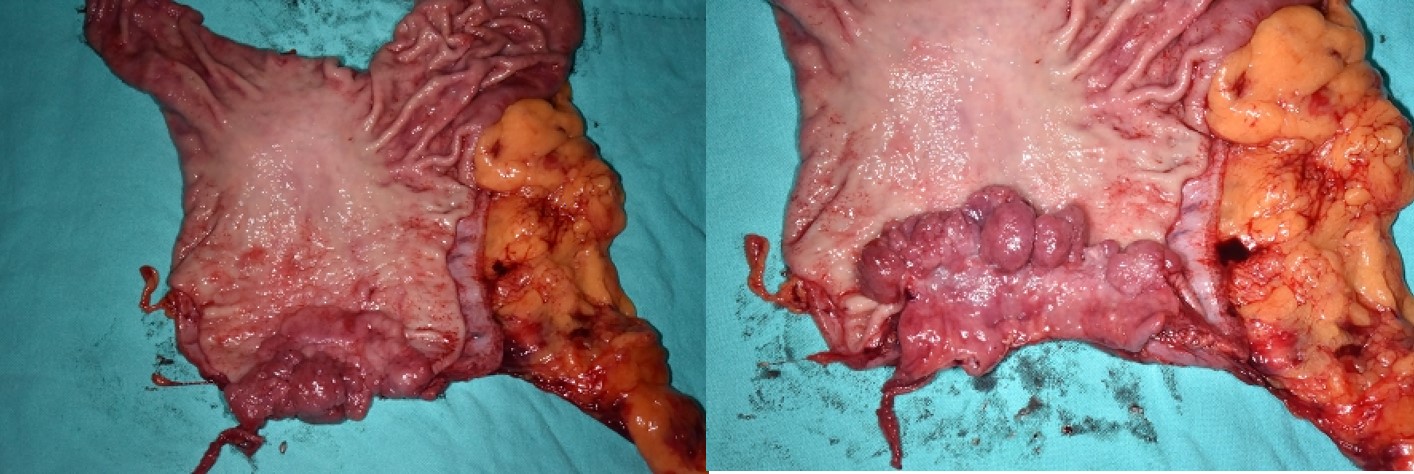
Stomach, radical subtotal gastrectomy: Early gastric carcinoma
1. Location : lower third, Center at pylorus and circle
2. Gross type : EGC type I
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size : 8.0x5.5 cm
6. Depth of invasion : invades mucosa (muscularis mucosae) (pT1a)
7. Resection margin: free from carcinoma, safety margin: proximal 9.0 cm, distal 1.5 cm
8. Lymph node metastasis : no metastasis in 40 regional lymph nodes (pN0) 9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. AJCC stage by 8th edition: pT1a N0
Differentiation between EGC type I and AGC type I is difficult. I would discuss it in the near future.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2019-11-15)