EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 847. Melena. Initial biopsy false negative.]
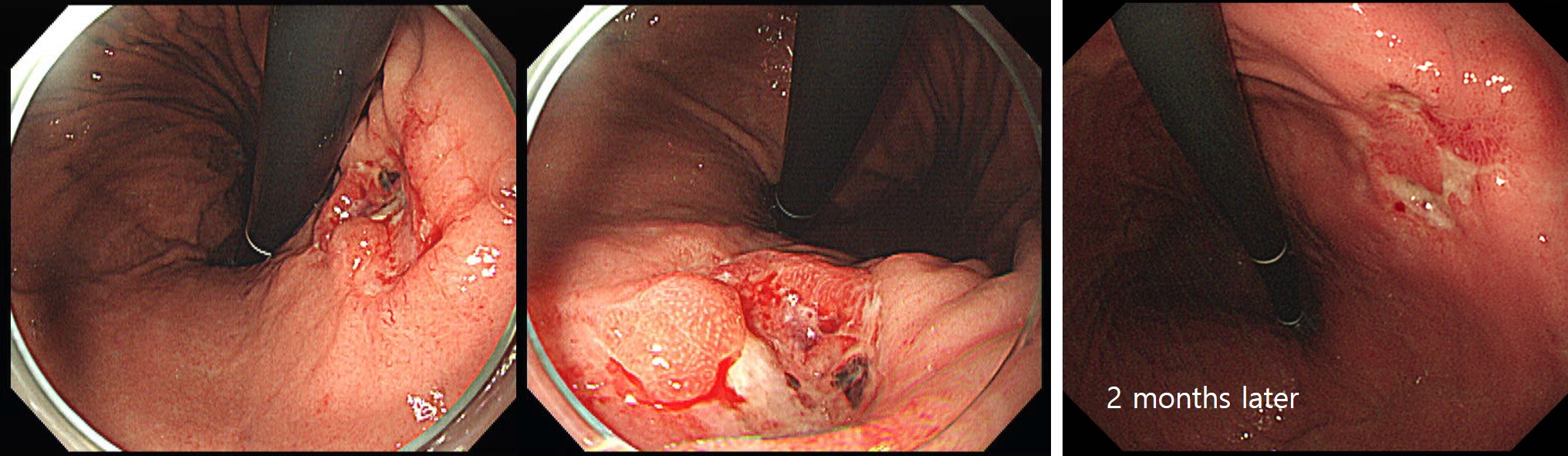
[Gastric cancer 847. Melena. Initial biopsy false negative.]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
A 45 years old lady was referred due to gastric cancer.
A few months ago, she developed melena and the endoscopic biopsy was negastive for malignancy. PPI treatment was done. In the follow up endoscopy 2 months later, the biopsy was poorly differentiated adenocarcinoma.
Biopsy is not 100% sensitive. It is especially true in the setting of bleeding. Careful interpretation of the endoscopic finding is very important to determine the timing of follow-up endoscopy. If cancer is suspected, 2nd endoscopy can be recommended as soon as possible.
Radical surgery was done.
Stomach, subtotal gastrectomy: Advanced gastric carcinoma
1. Location : middle third, Center at low body and posterior wall
2. Gross type : Borrmann type 3
3. Histologic type : tubular adenocarcinoma, poorly (poorly cohesive) differentiated
4. Histologic type by Lauren : diffuse
5. Size : 3.2x3 cm
6. Depth of invasion : penetrates subserosal connective tissue (pT3)
7. Resection margin: free from carcinoma, safety margin: proximal 1.5 cm, distal 9 cm
8. Lymph node metastasis : no metastasis in 35 regional lymph nodes (pN0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : present
12. AJCC stage by 8th edition: pT3 N0
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2020-3-30)