EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric Cancer 002. P/D로 ESD 했는데 M/D, SM invasion으로 나온 위암] - 終
[Gastric Cancer 002. P/D로 ESD 했는데 M/D, SM invasion으로 나온 위암] - 終
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
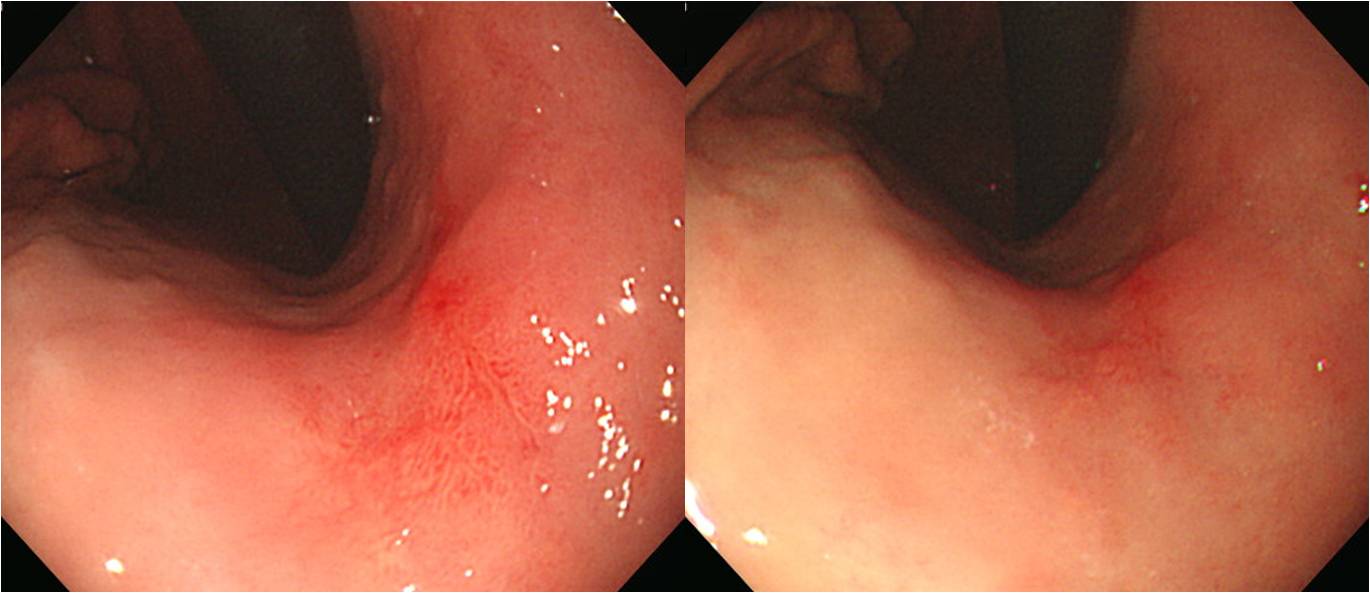
조직검사는 P/D adenocarcinoma였습니다. ESD를 하시겠습니까? 수술을 권하시겠습니까?
![]() [2014-4-16]
[2014-4-16]
수술을 권했습니다. P/D 형은 보통 수술을 보내고 있습니다. P/D나 signet ring cell carcinoma를 포함한 expanded indication이 그다지 미덥지 않습니다. 적어도 제게는...
1. Location : middle third, center at body and lesser curvature
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated
4. Histologic type by Lauren : intestinal
5. Size : 2.7x1.4 cm
6. Depth of invasion : invades submucosa (sm1) (pT1b)
7. Resection margin: free from carcinoma, safety margin: proximal 3.8 cm, distal 11.2 cm
8. Lymph node metastasis : no metastasis in 29 regional lymph nodes (pN0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
![]() [2026-7-15. update]
[2026-7-15. update]
2022년 발표되었고 2024년 개정되어 2025년 1월 Journal of Gastric Cancer에 발표된 Korean Gastric Cancer Guideline 2024에서 미분화조직형 위암의 ESD에 대한 추천은 아래와 같습니다. Cautiously consider할 수 있고 근거수준은 낮고 추천강도는 conditional for라는 것입니다. 매우 중요한 내용이므로 가이드라인의 해당 부분 전문을 읽어보실 것을 권합니다. 옮깁니다.
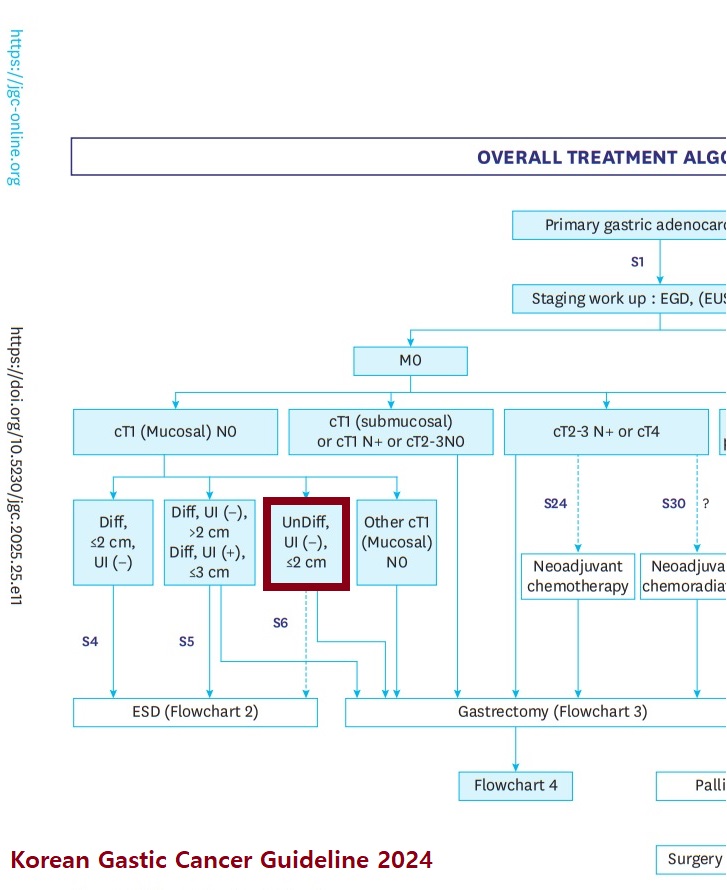
Statement 6: Endoscopic resection could be cautiously considered for poorly differentiated tubular or poorly cohesive (including signet-ring cell) EGCs meeting the following endoscopic findings after sufficient discussion: endoscopically estimated tumor size ≤2 cm, endoscopically mucosal cancer, and no ulcer in the tumor (evidence:low, recommendation: conditional for).
EGCs with poorly differentiated tubular and PCC (including SRCC) are associated with a higher risk of LN metastasis than well and moderately differentiated tubular EGCs, making endoscopic resection very cautious consideration.
In previous Japanese Gastric Cancer Guidelines
, a literature review of the literature that endoscopic resection could be considered for poorly differentiated tubular adenocarcinoma or PCC (including SRCC) in cases with histologic confirmation from forceps biopsy specimens, endoscopically estimated tumor size ≤2 cm, endoscopically mucosal cancer, and no ulcer in the tumor. When these criteria were met, the risk of LN metastasis was reported to range from 0% to 2.3%. Under the mentioned endoscopic findings, endoscopic resection could be considered for initial treatment. However, when risk factors for LN metastasis (tumor size >2 cm, submucosal invasion, ulcer in the tumor, and lymphovascular invasion) are revealed in pathologic reports, additional gastrectomy may be necessary.
In this guideline, we reviewed recent literature published since the previous edition. Currently, no prospective RCTs have compared the long-term OS of endoscopic resection with that of gastrectomy with LN dissection, which is the standard treatment for these indications. Retrospective studies have shown no difference in OS between gastrectomy and endoscopic resection, though endoscopic resection had a higher local recurrence rate in terms of recurrence-free survival (RFS), which is consistent with the findings of previous studies. In a prospective, single-arm, phase III observational study in Japan (JCOG1009/1010), the curative resection rate of the endoscopic resection group in undifferentiated EGC was 71% (195/275). Over a median follow-up period of 69.9 months, the 5-year OS rate was 99.3% (95% CI, 97.1% to 99.8%) and 5-year RFS rate was 98.9% (95% CI, 96.5% to 99.6%). In Korea, a study on the Comparison of Endoscopic Resection And Surgery for Early Gastric Cancer with undifferentiated histological type: a multicenter RCT (ERASE-GC trial, NCT04890171), is currently ongoing, and its results should be followed-up.
To date, the standard treatment for these criteria has been gastrectomy with LN dissection. Only retrospective cohort studies support these criteria for endoscopic resection, and the data from prospective trials are still lacking. Additionally, a significant portion of cases estimated to meet these criteria in the pre-endoscopic resection workup are found to be out these criteria upon pathologic examination of endoscopic resection specimens. Therefore, standard surgery (gastrectomy with LN dissection) can also be considered for cases meeting these criteria. It is advisable to choose a treatment method after sufficient discussion with the patient about the possibility of LN metastasis, and complications associated with endoscopic procedure and surgery.
2018년 일본가이드라인에서는 미분화조직형 위암의 ESD는 expanded indication이라고 표현하였습니다. 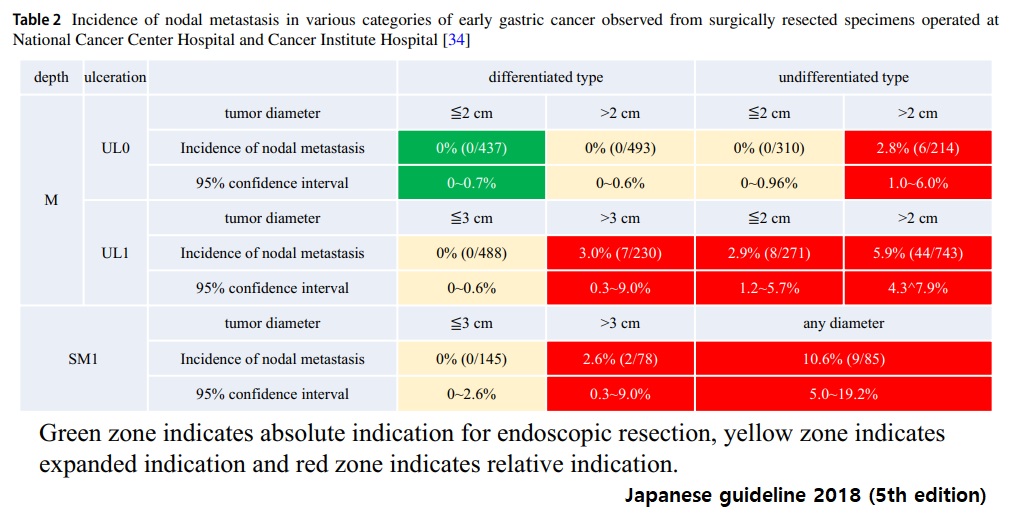 그런데 2025년 일본가이드라인에서는 2018년의 absolute indication for endoscopic resection을 absolute indication for EMR or ESD으로 바꾸고, 2018년의 expanded indication을 absolute indication for ESD로 바꾸고 대신 eCura A-1의 국소재발을 expanded indication으로 새롭게 정의하는 엄청난 변화를 일으켰습니다.
그런데 2025년 일본가이드라인에서는 2018년의 absolute indication for endoscopic resection을 absolute indication for EMR or ESD으로 바꾸고, 2018년의 expanded indication을 absolute indication for ESD로 바꾸고 대신 eCura A-1의 국소재발을 expanded indication으로 새롭게 정의하는 엄청난 변화를 일으켰습니다. 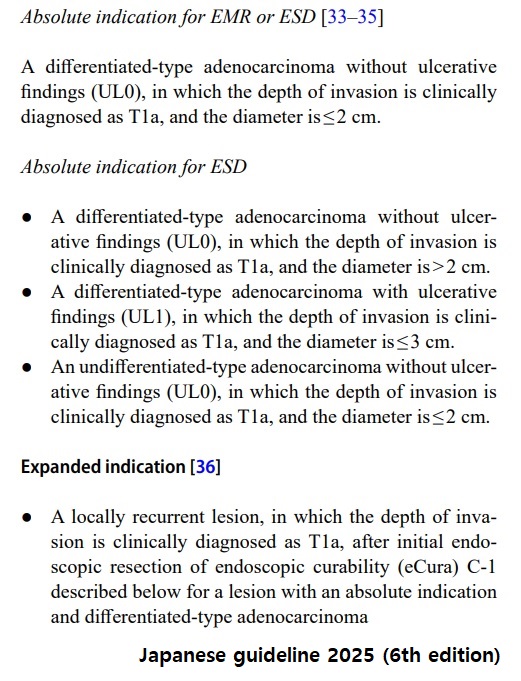 두 가이드라인 사이에 새롭게 나온 근거는 거의 없는 상황에서 왜 2018년의 expanded indication이 2025년의 absolute indication으로 바뀌었는지 설명은 없습니다. 그저 놀라울 뿐입니다. 지나친 도약이었다고 생각합니다.
두 가이드라인 사이에 새롭게 나온 근거는 거의 없는 상황에서 왜 2018년의 expanded indication이 2025년의 absolute indication으로 바뀌었는지 설명은 없습니다. 그저 놀라울 뿐입니다. 지나친 도약이었다고 생각합니다.
일본의 작은 single arm 관찰연구(JCOG1009/1010)의 결과가 좋았고, 우리나라의 다기관 전향연구(ERASE-GC trial, NCT04890171)에서 긍정적 결과가 나오더라도 저는 미분화조직형 위암을 ESD의 absolute indication으로 바꾸는 것에 대하여 매우 조심스러워야 한다고 생각해야 합니다. 사실 반대하는 입장입니다. Bias가 너무 많기 때문입니다. 저의 경험과 일치하지 않기 때문입니다.
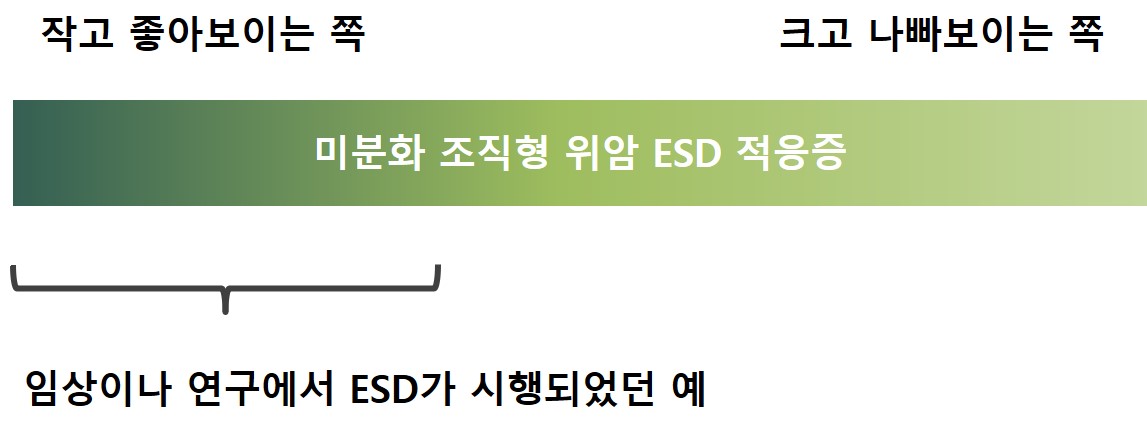
JCOG1009/1010은 '2cm 이하의 궤양이 없는 점막암으로 추정되는 미분화조직형 위암'을 모두 ESD로 치료하여 장기 성적을 분석한 연구가 아닙니다. '2cm 이하의 궤양이 없는 점막암으로 추정되는 미분화조직형 위암' 중 경계가 명확하고, 1cm 이하이고, flat하고 경계가 좋은 것, 즉 치료하기 쉽고 예후가 좋을 것으로 추정되는 것들을 주로 선정하여 ESD를 한 결과를 분석한 것에 지나지 않습니다.
임상 연구의 결과와 여러분이 환자를 치료한 결과가 다른 이유 중 하나가 '적응증 중 좋아보이는 예들만 골라서 randomization에 들어갔기 때문'일 수 있습니다. 만약 그러하였다면 다음과 같은 결론이 나옵니다. '좋다. 나쁜 것만 빼면' 나쁜 것 한두개를 빼면 결과가 좋아집니다. 그게 연구의 한계입니다. Randomization이 모든 bias를 해결해 주지 않습니다. 가이드라인이나 임상연구의 결론만 보지 마시고 그 맥락, 배경, 숨은 이야기 등을 이해하려고 노력하십시오. 이게 전문가와 솔직한 대화를 해야 하는 이유입니다. 학회 발표보다 질문이나 comment가 더 중요한 이유입니다. 직접 찾아가서 옆에서 봐야 하는 이유입니다. 술 한잔 마시고 나누는 대화가 중요한 이유입니다.
이러한 아이디어는 논문이나 리뷰로 실리는 예가 거의 없습니다. 2025년 Hatta의 JGC review에서도 이러한 측면은 고려되지 않은 것 같습니다. 과거 저는 아래 두 논문을 보고 감탄한 적이 있습니다. 연구의 변방인 그리스의 한 시니컬한 연구자의 글입니다. 균형잡힌 시각을 위하여 일독을 권합니다.
![]() © 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Jun Haeng Lee (2014-4-16)
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Jun Haeng Lee (2014-4-16)