EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 834. EGC in an aspirin-user]
[Gastric cancer 834. EGC in an aspirin-user]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
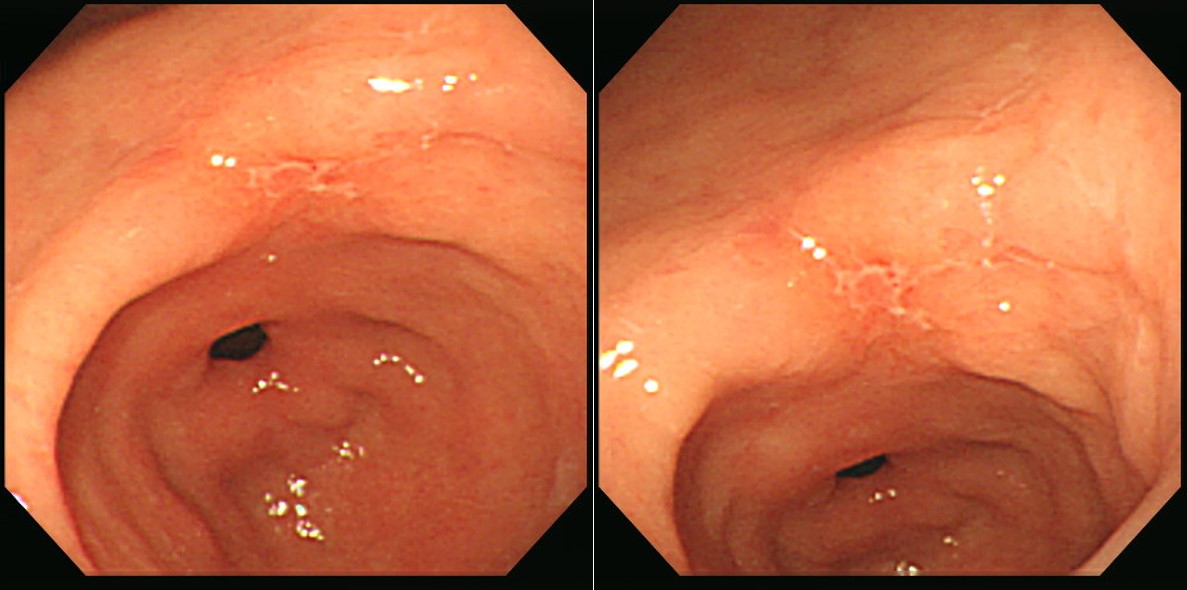
A small depressed lesion was found in a 65 years old aspirin user. The initial biopsy was "chronic gastritis, active, with intestinal metaplasia and ulcer. Hp (-)". What's your plan?
.
.
.
.
.
.
.
.
.
.
In a repeated endoscopy (after a few weeks of PPI treatment), the depresseed lesion persisted and the edge became more irregular. The biopsy was well-differentiated adenocarcinoma. ESD was done.
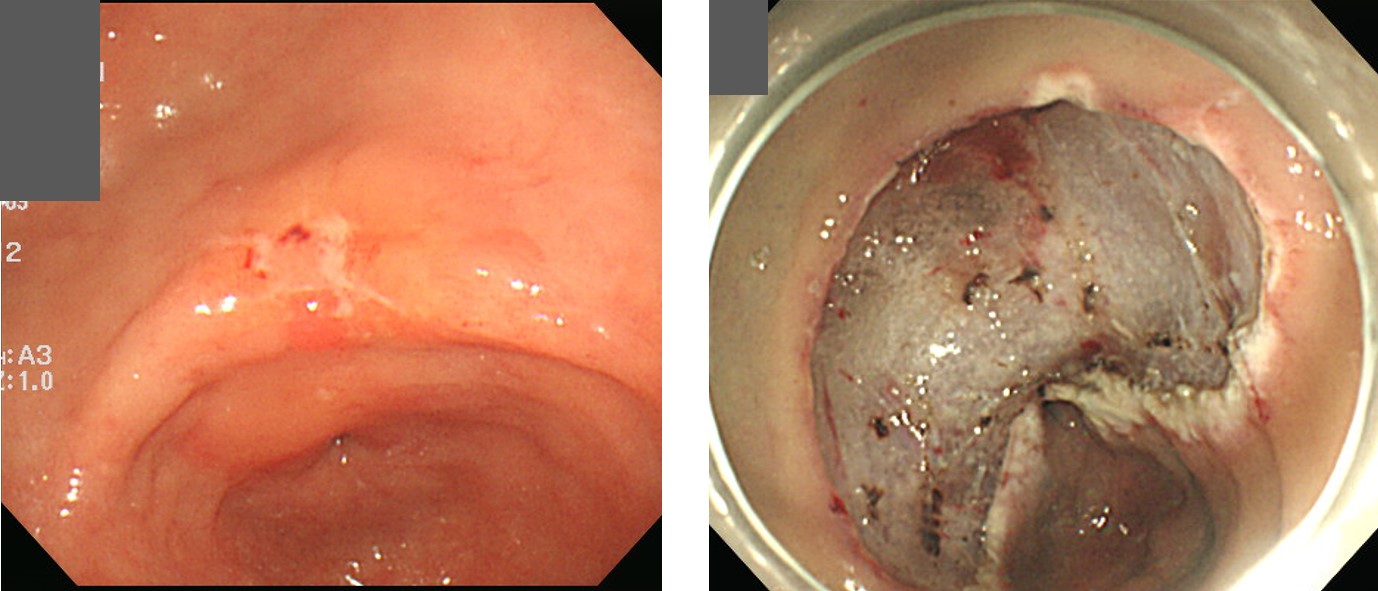
ESD: Early gastric carcinoma
1. Location : antrum, lesser curvature
2. Gross type : EGC type IIc
3. Histologic type : tubular adenocarcinoma, moderately differentiated >> tubular adenocarcinoma, poorly differentiated (about 3 %)
4. Histologic type by Lauren : intestinal
5. Size of carcinoma : (1) longest diameter, 18 mm (2) vertical diameter, 13 mm
6. Depth of invasion : invades mucosa (muscularis mucosa) (pT1a)
7. Resection margin : free from carcinoma(N) safety margin : distal 6 mm, proximal 11 mm, anterior 16 mm, posterior 10 mm
8. Lymphatic invasion : present
9. Venous invasion : not identified(N)
10. Perineural invasion : not identified(N)
11. Microscopic ulcer : absent
12. Histologic heterogeneity: present
Surgery was recommended following the guidelines, and there was no residual tumor or lymph node involvement in the surgery specimen.
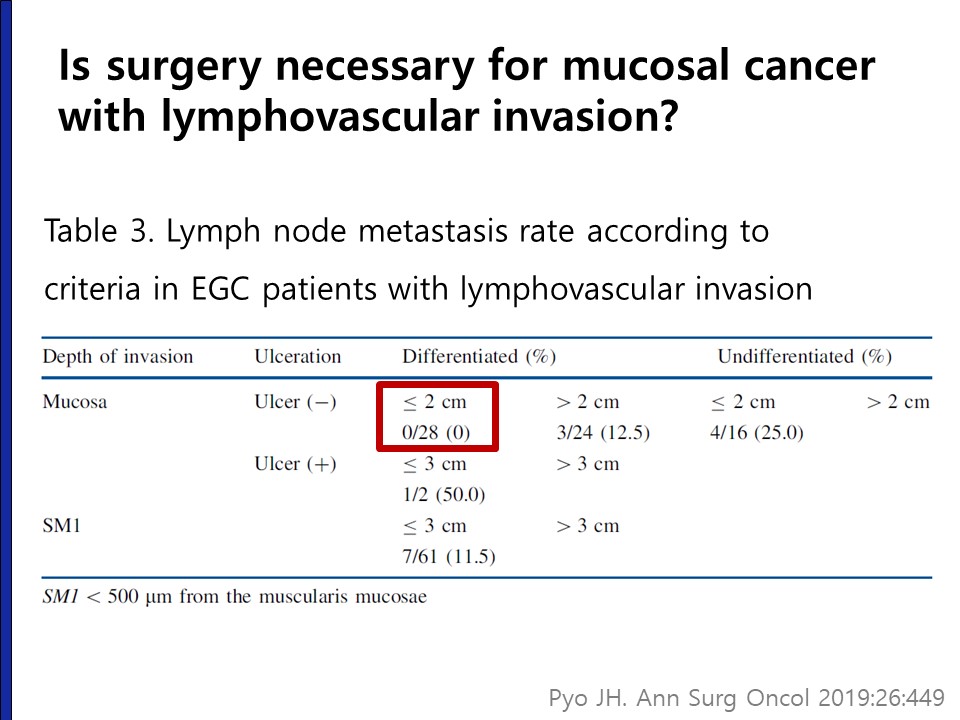
It is still unclear whether salvage surgery must be done for all patients with lymphatic invasion. Maybe we are doing too much surgery after ESD. Do you think surgery is necessary for mucosal cancer with lymphovascular invasion?
As you can see in the red box, in lymphovascular invasion positive patients within the traditional absolute indication (mucosal cancer, differentiated type, no ulcer, less than 2 cm), there was no lymph node metastasis in surgery (Ann Surg Oncol 2019). Careful observation without additional surgery can be an option for this group of patients.
In this case, the decision making is even more difficult due to the histological heterogeneity (3% poorly differentiated component). Based on our recent publication (Ann Surg Oncol 2019), I think that informed discussion about careful observation without surgey can be provided to the patient.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2020-2-27)