EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [Gastric cancer 860. Cardia cancer]
[Gastric cancer 860. Cardia cancer]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
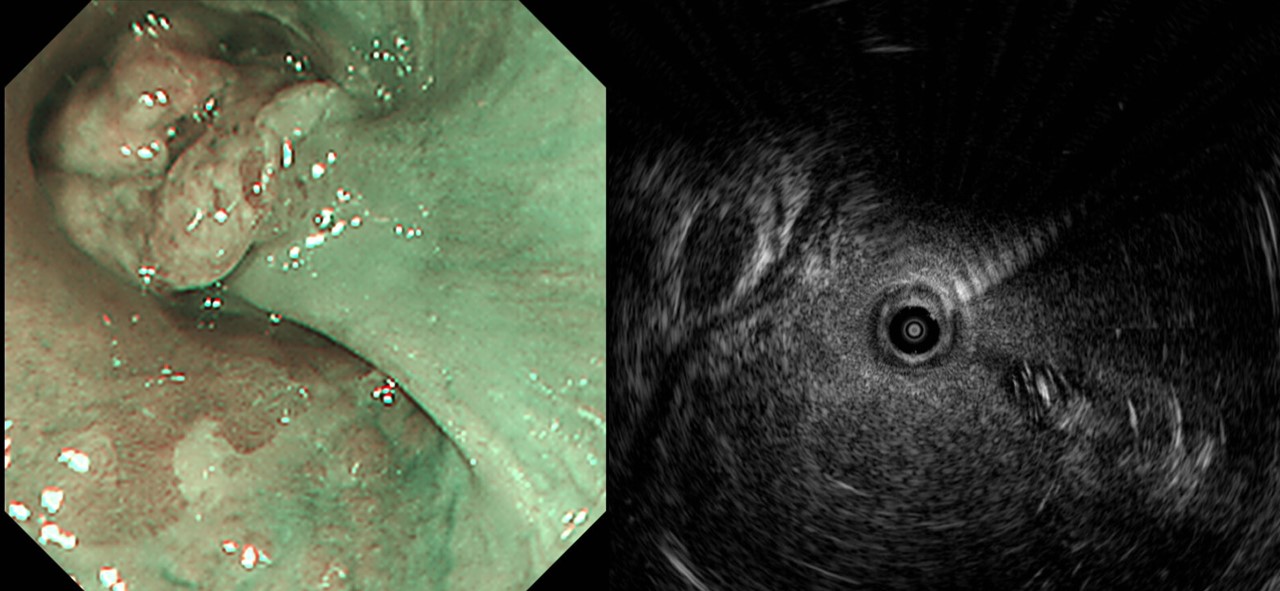
62 years old male was referred for the managment of EGC at cardia (pathology: M/D adenocarcinoma). In the previous hospital, it was staged as T1b (submucosal cancer) based on the EUS finding. Total gastrectomy was recommended but the endoscopist told that the chance of endoscopic treatment is around 10-20%. What would you do?
Endoscopic examination was repeated. It was not a pure polypoid tumor. It was a flat elevated type tumor with polypoid portion and depressed portion in it. I recommended surgery.
Total gastrectomy was done and this is the final pathology.
Stomach, radical total gastrectomy: Early gastric carcinoma
1. Location : upper third, Center at cardia (Siewert I)
2. Gross type : EGC type I
3. Histologic type : tubular adenocarcinoma, well differentiated
4. Histologic type by Lauren : intestinal
5. Size : 2.1x2.0 cm
6. Depth of invasion : invades mucosa (muscularis mucosae) (pT1a)
7. Resection margin: free from carcinoma, safety margin: proximal 0.5 cm, distal 15.3 cm
8. Lymph node metastasis : no metastasis in 55 regional lymph nodes (pN0)
9. Lymphatic invasion : not identified
10. Venous invasion : not identified
11. Perineural invasion : not identified
12. Peritoneal cytology : negative
13. AJCC stage by 8th edition: pT1a N0
I hate EUS in the initial evaluation of gastric cancer. I never do it.
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2020-5-21)