EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
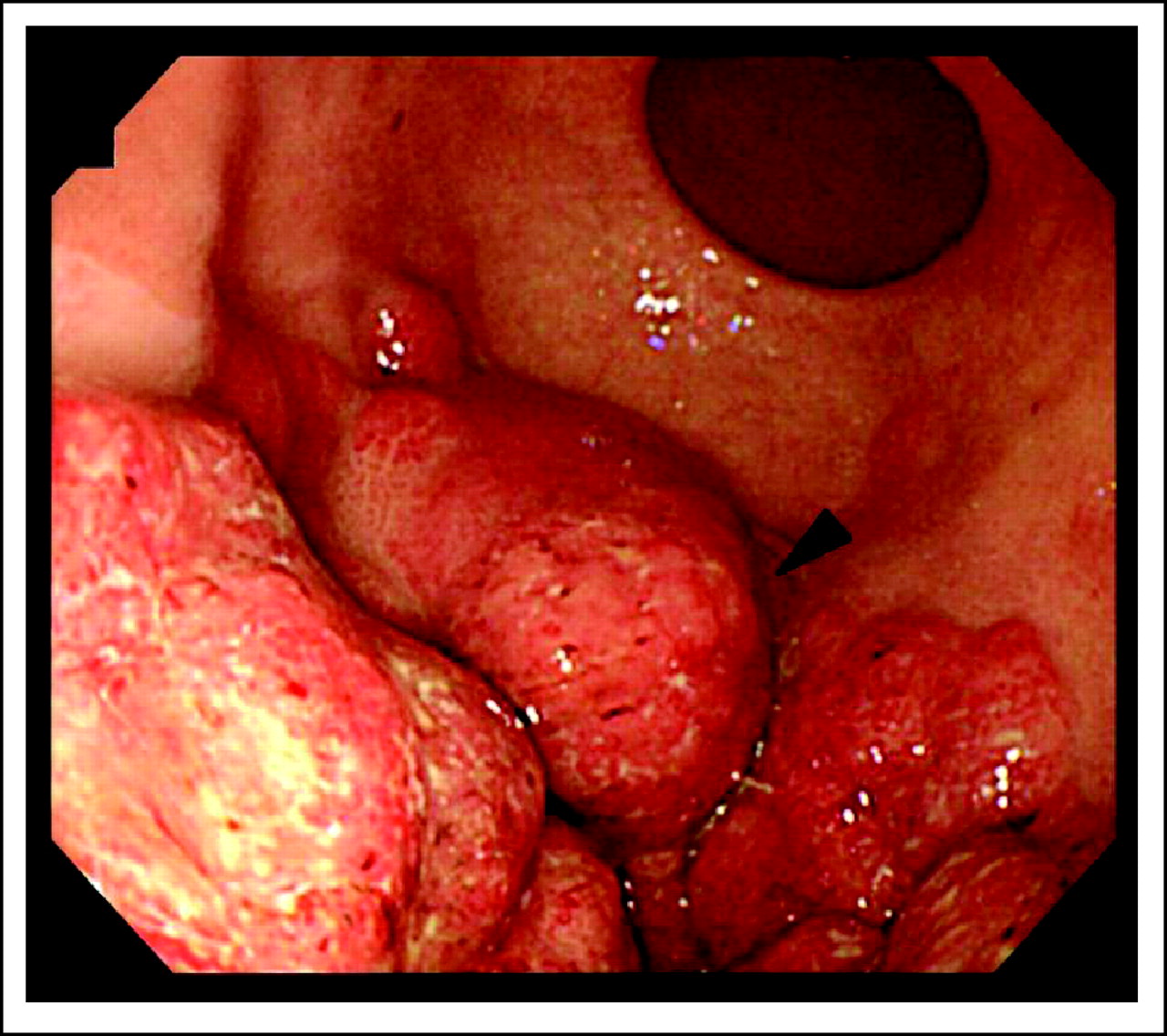
![]() [Gastric cancer 862. Gastric recurrence of extramedullary granulocytic sarcoma]
[Gastric cancer 862. Gastric recurrence of extramedullary granulocytic sarcoma]
001 | 101 | 201 | 301 | 401 | 501 | 601 | 701 | 801 | 901 | 1000
This is a somewhat old case report from my institution (Journal of Clinical Oncology 2009). Rare and lots of learning points. I summarized the case report.
A 38-year-old woman was diagnosed with acute myeloid leukemia (AML). She received chemotherapies, an allogeneic HSCT, and total-body irradiation. There was no evidence of extramedullary involvement of AML on pretransplant evaluation, including evaluation of the upper GI tract. Her post-transplant course was complicated by extensive chronic graft-versus-host disease (GVHD) involving the skin, oral cavity, and lung, which was treated with tacrolimus and corticosteroids.
Fifteen months after allogeneic hematopoietic stem-cell transplantation (HSCT), she suddenly developed left sided flank pain with evidence of left costovertebral angle tenderness. Computed tomography (CT) scan revealed diffuse wall thickening in the middle portion of the left ureter and hydronephrosis together with extensive submucosal wall thickening in the body and fundus of the stomach.
Pathologic findings were consistent with myeloid sarcoma based on myeloperoxidase and CD13 antigen?positive myeloblastic cells in the stomach tissue. Immunohistochemical evaluation demonstrated the presence of blasts positive for leukocyte common antigen, lysozyme, CD13, and CD56 and negative for CD15 and CD117. Marrow examination demonstrated no evidence of marrow involvement with AML blasts. The patient received salvage chemotherapy which consisted of high-dose cytarabine and amsacrine with withdrawal of the immunosuppressive agent.
EMR (extramedullary recurrence) of acute myeloid leukemia (AML) is not uncommon after allogeneic HSCT. Isolated EMRs without evidence of leukemia in the marrow, however, rarely occur. EMR involves the skin or CNS relatively frequently, but involves the stomach or genitourinary tract very rarely.
The potential mechanism of the development of EMR without coexisting leukemic marrow involvement is that the graft-versus-leukemia (GVL) effect is particularly more potent in the marrow, but is weaker in the extramedullary sites. Thus, relapsing leukemia in the extramedullary sites frequently escapes the GVL effect. Thus, previous experience with extensive chronic GVHD has been more frequently observed in patients developing EMR compared to those developing only marrow relapse of leukemia after allogeneic HSCT in whom chronic GVHD usually does not develop.
You can read the full discussion at https://ascopubs.org/doi/10.1200/JCO.2009.23.7560. The relationship between GVHD and extramedullary recurrence without BM involvement is interesting.
* 참고: EndoTODAY 혈액질환 위전이 혹은 위침윤
최이령 선생님. 이런 훌륭한 증례 보고가 있었던 것을 미처 알지 못했습니다. 10년이나 지났지만... 축하합니다. 정말 멋진 일을 하셨습니다!!!
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng. (2020-5-31)