EndoTODAY ГЛНУАц БГНЧ
EndoTODAY ГЛНУАц БГНЧ
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [KINGCA 2018]
[KINGCA 2018]
РЯНУ: 2018Гт 4Пљ 26РЯ (Иё) - 4Пљ 28РЯ (Хф)
РхМв: БзЗЃЕх ПіФПШњ МПя
![]() 1. [10:00-11:30] GEJ Cancer - General principle
1. [10:00-11:30] GEJ Cancer - General principle
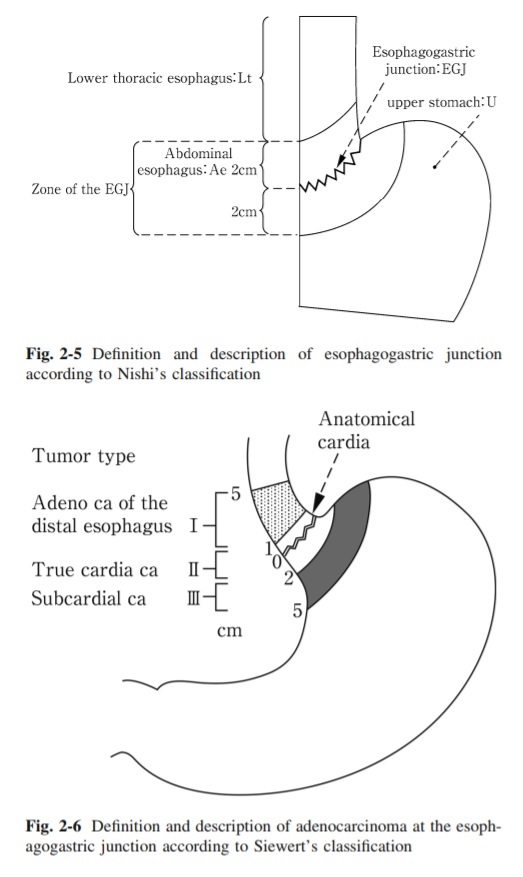
1) History of GEJ cancer treatment strategy (Arnulf H. Holscher)
РЏЗДПЁМДТ Siewert КаЗљ(Chirurg 1987;58:25-32)АЁ, РЯКЛПЁМДТ Nishi КаЗљ(1973)АЁ ЛчПыЕЫДЯДй.
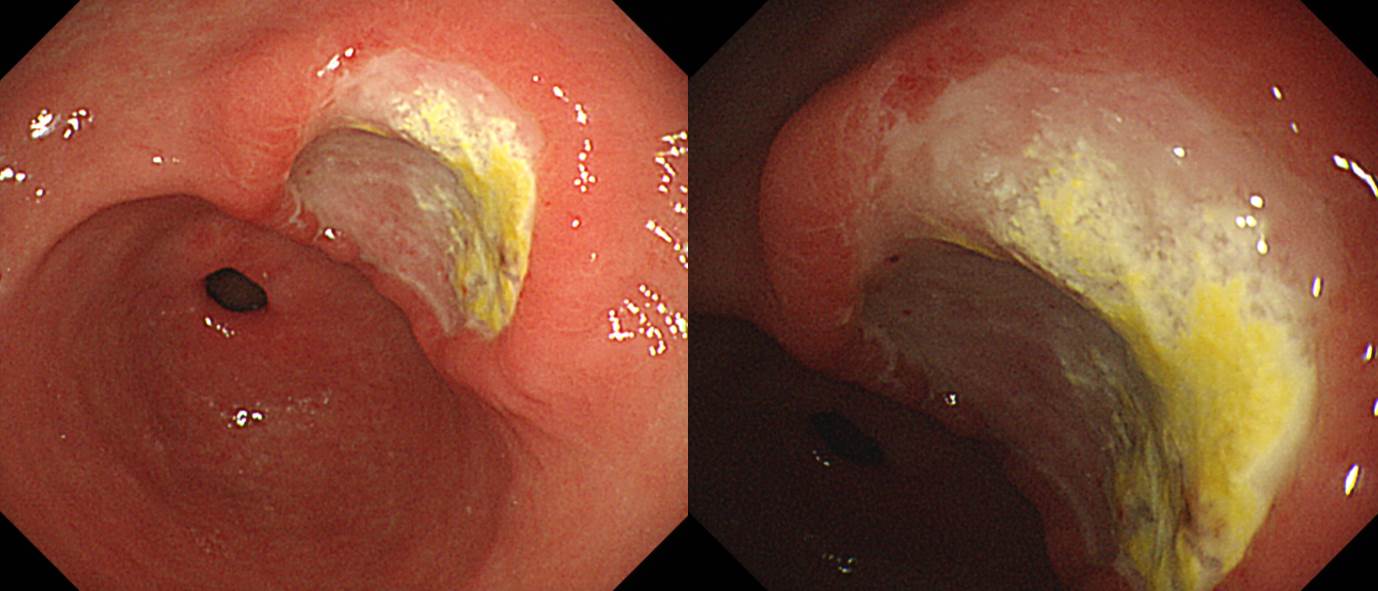
2) Endoscopic finding and results of ESD (Ichiro Oda)
Clinicopatholgical characteristics of early GEJ cancer Male
Differentiated type
HP -
Gastric atrophy -
0~6 o'clock location
IIc or IIa
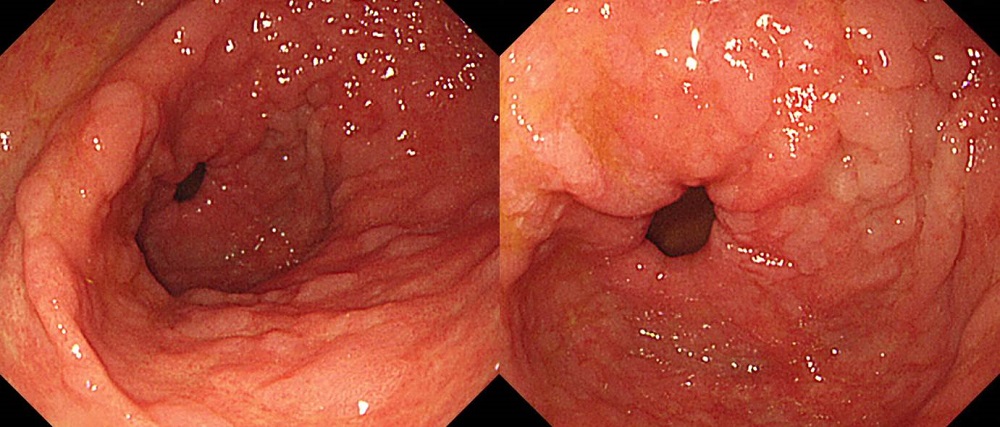
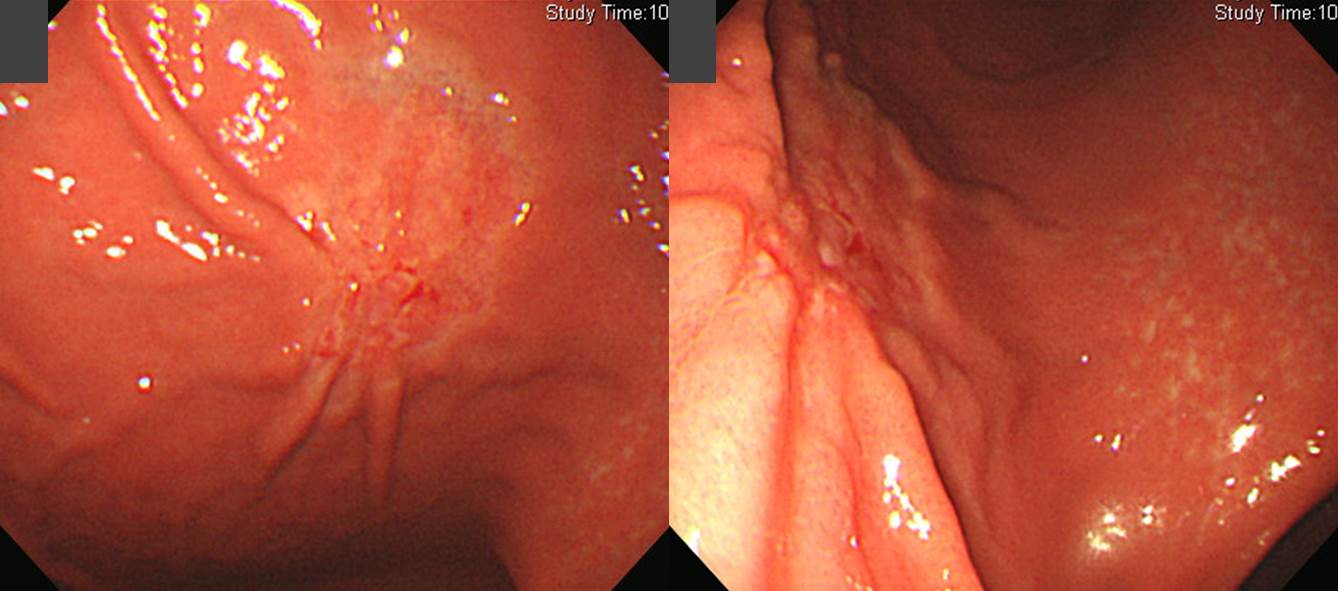
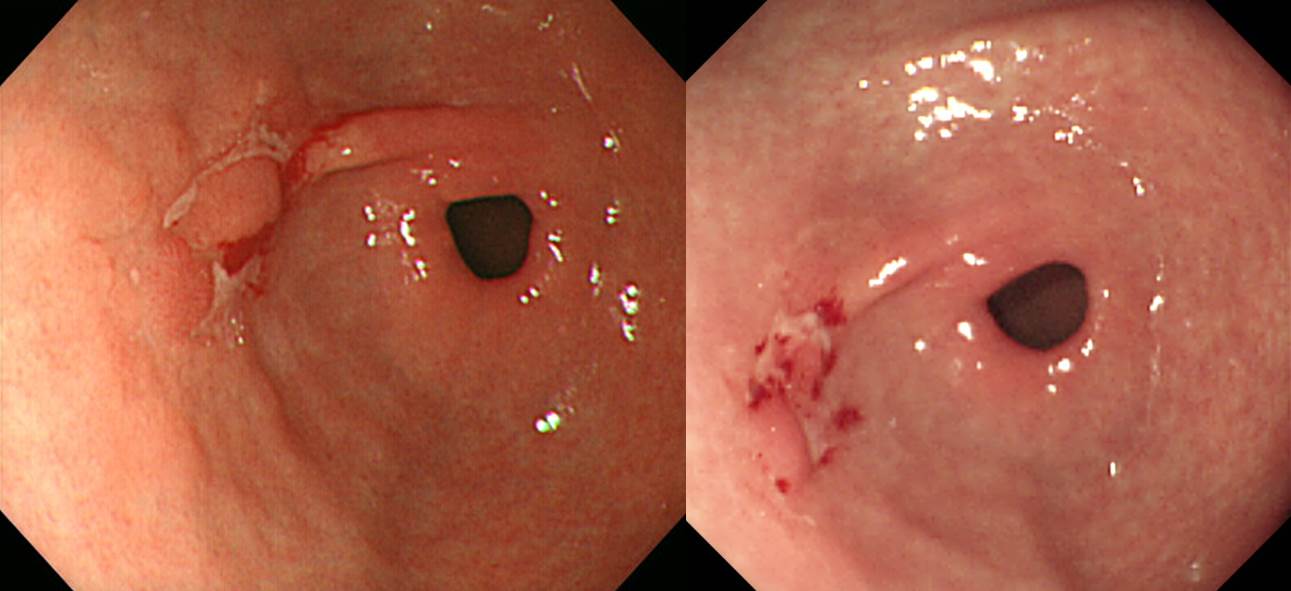
Reddish in colorHis angleПЁ РЇФЁЧб GEJ cancerРЧ ГЛНУАц ФЁЗс РќЗЋ: НФЕЕ ТЪРЛ ИеРњ ЧѲЧб ШФ РЇ КЮКаРЛ Р§СІЧбДй. Oda МБЛ§ДдРК Dual knifeЗЮ precuttingРЛ ЧЯАэ IT-2 knifeЗЮ submucosal dissectionРЛ ЧЯДТ КёЕ№ПР ХЌИГРЛ КИПЉСжОњНРДЯДй.
ЕПАцОЯМОХЭПЁМДТ ИХГт gastric ESD 500ПЙ, НФЕЕ ESD 200ПЙ СЄЕЕ НУЧрЕЧСіИИ GEJ ОЯПЁ ДыЧб ESDДТ 5-10ПЙ СЄЕЕ НУЧрЕШДйАэ ЧеДЯДй.
3) LN metastasis & recurrence patten (ПяЛъДы РЬРЮМЗ)
ЕЖРЯ РкЗс: Feith M. Surg Oncol Clin N Am 2006, Gertler R. Ann Surg 2014
РЯКЛ РкЗс: Yamashita. Gastric Cancer 2017
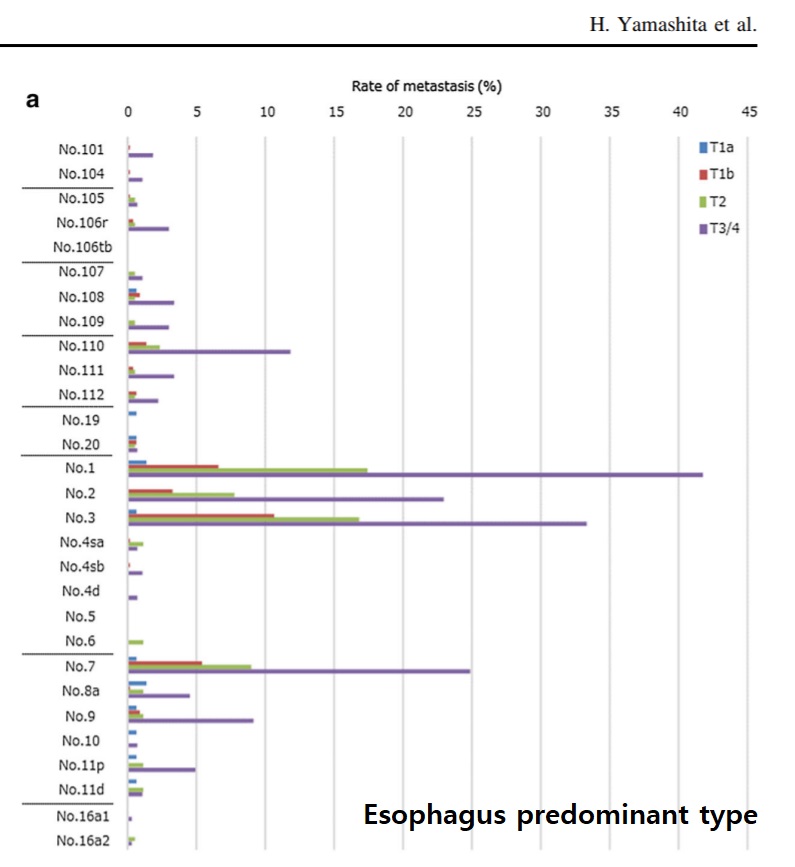
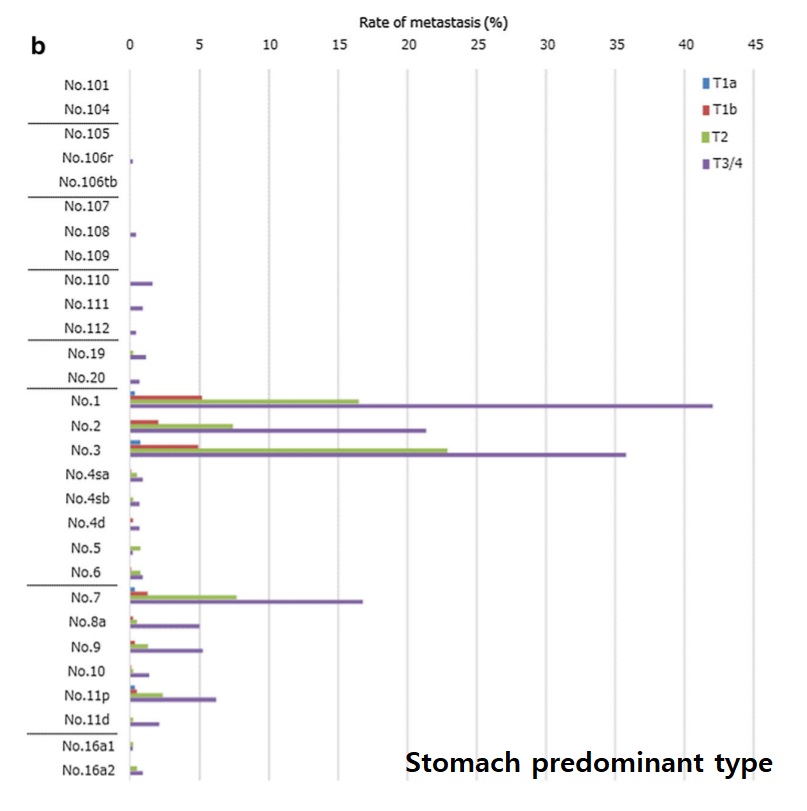
ЧбБЙ РкЗс: Suh. Ann Surg Oncol 2017
4) Upfront surgery vs. CCRTx: from the view of oncologist compared to esophageal cancer (УцКЯДы ЧїОзСООчГЛАњ ЧбЧ§Мї)
GEJ adenocarcinoma is a 'Zone Disease' rather than an 'Oragn disease'
Type I GEJ adenocarcinoma should be regarded as similar to esophageal cancers, and treated like esophageal cancer with preoperative CCRT followed by esophagectomy and mediastinal lymphadenectomy.
Type II and III GEJ adenocarcinoma should be regarded as similar to gastric cancers, and treated like gastric cancer with total gastrectomy and D2 lymphadenectomy.
* ТќАэ: EndoTODAY GEJ cancer
* ТќАэ: Japanese classification of esophageal cancer, 2017
![]() 2. [11:40-12:10] JS Min memorial lecture. ЙцПЕСж
2. [11:40-12:10] JS Min memorial lecture. ЙцПЕСж
![]() [13:10-14:40] Basics for gastric cancer treatment
[13:10-14:40] Basics for gastric cancer treatment
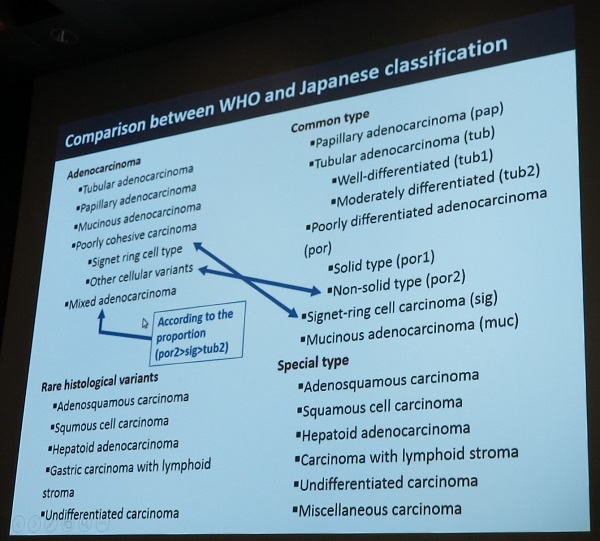
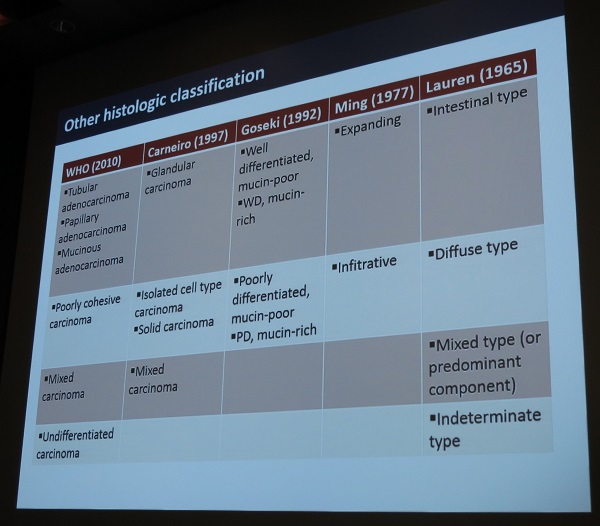
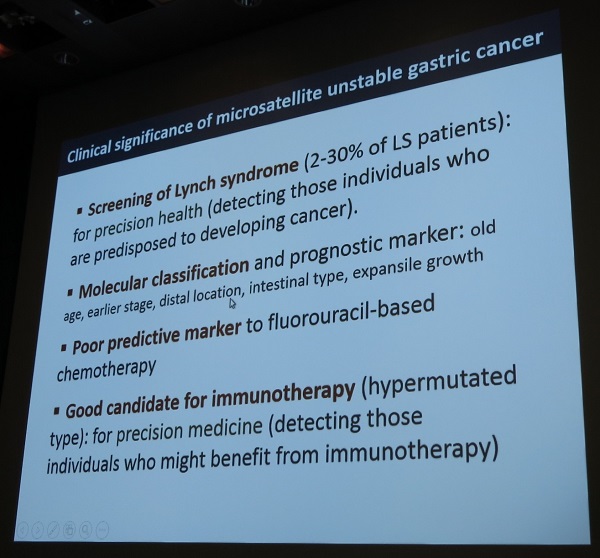
1) Pathological classification of gastric cancer
2) Endoscopy and EUS findings of gastric cancer (МКБеАќДыЧаБГ РЬСиЧр)
PPT PDF 5.0M
Traditionally learning endoscopy means learning endoscopy insertion techniques. After observing a few cases, I just started inserting the endoscope into the patientЁЏs stomach. When I found an ulcer or polyp, I had no idea whether it is benign or malignant. But everything changed. Or everything must be changed. You should not insert the endoscope without sufficient training. Our endoscopy learning program at Samsung Medical Center starts with BOXIM, which means box simulator training and DEX, description exercise.
There are many kinds of simulators. Pictures on the top are full electronic endoscopy simulator, GI Mentor and GI Mentor II. Although expensive, we donЁЏt use it anymore. I think box simulators are much useful than GI Mentor II.
The left-hand side is the old style, and the right-hand side is the new model. We start with old style simulator because it is easier to teach and learn.
We started box simulator training in the year 2005. However, our training session was always in the evening. Why? Because we didnЁЏt have a training room.
So, I changed a small warehouse into the box simulator training room.
Now, we can teach and learn the basic endoscopy skills in the box simulator training room before the sunset.
A few days ago, box simulator training session was held for the foreign doctors in the KINGCA Master Class in the BOXIM training room.
All the education materials for endoscopy beginners are available at my personal homepage at endotoday.com. The next course after BOXIM training is description exercise.
The beginners make a description for the endoscopy cases following the SMC style, which means location, size, major finding, minor findings, impression and classification. Teachers usually give personalized feedback.
[ПмАњ МБЛ§Дд СњЙЎ]
РњШё БтАќПЁМДТ МіМњ ШФ ШЏРк ГЛНУАцРЛ ПмАњПЁМ ЧЯАэ РжНРДЯДй. ОюЖВ АцПьПЁ СЖСїАЫЛчИІ ЧиОп ЧеДЯБю?
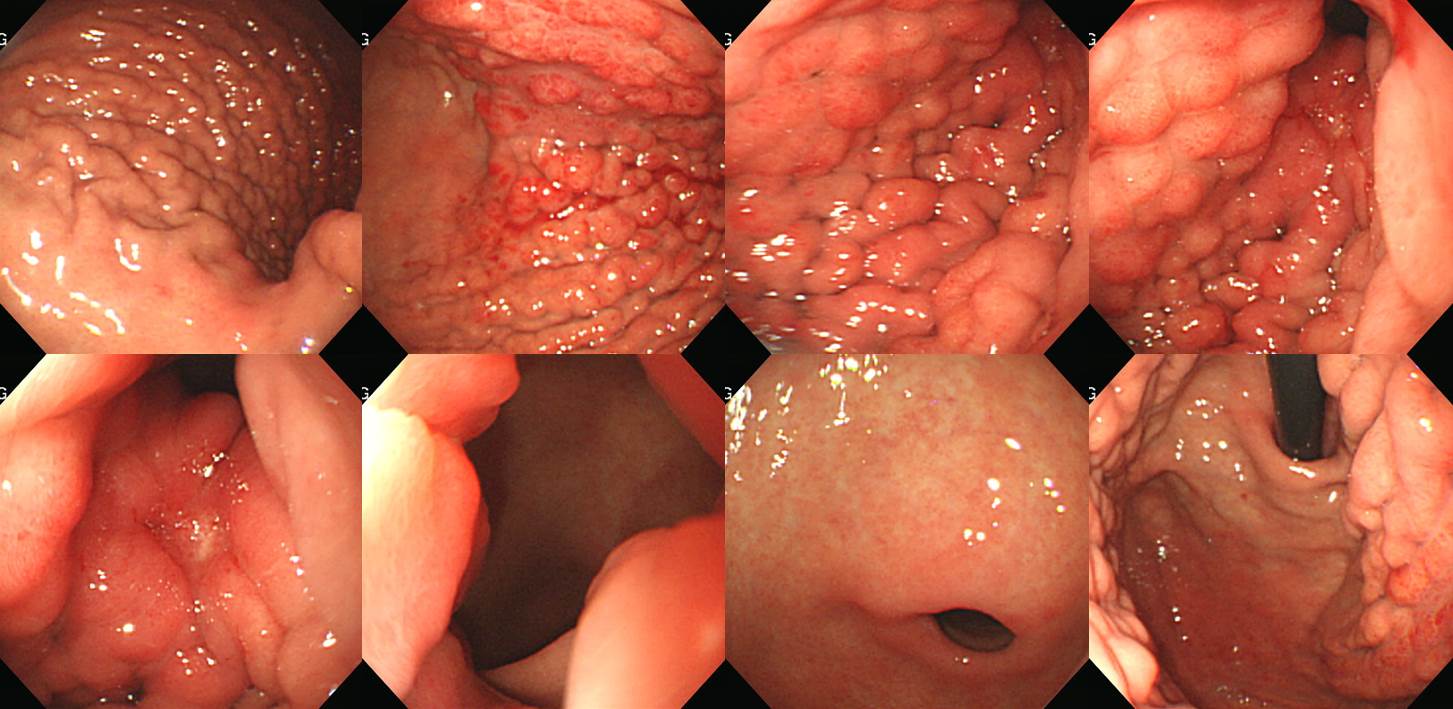
[РЬСиЧр ДфКЏ]
(1) Subtotal gastrectmoy ШФ remnant stomachРЛ АќТћЧЯДТ АЭРК ИХПь ОюЗСПю РЯРдДЯДй. РЯЙнРћРЮ РЇГЛНУАцПЁ ИХПь РЭМїЧиСј ШФ remnant stomachПЁ ДыЧб ГЛНУАцРЛ ЧЯДТ АЭРЬ ССАкНРДЯДй.
(2) МіМњ КДИЎИІ ШЎРЮЧб ШФ АЫЛчЧЯДТ АЭРЬ ССНРДЯДй. Undifferentiated histologyРЬАэ resection marginРЬ УцКаЧЯСі ОЪРК АцПьДТ anastomosis site recurrenceИІ ДѕПэ СжРЧЧиОп ЧЯБт ЖЇЙЎРдДЯДй.
(3) Remnant stomachРЧ КИИИ 4Чќ СјЧрМК РЇОЯРЛ СжРЧЧЯНЪНУПф.
(4) ДйИЅ КЮРЇПЭ ИЖТљАЁСіЗЮ erosion, ulcer, localized tumorДТ СЖСїАЫЛчРЧ ДыЛѓРдДЯДй.
(СЄФЁРћРЮ РЬНДЖЇЙЎПЁ ДйРНРК ИЛЧЯСі ОЪОвНРДЯДй. ВР ИЛЧиСжАэ НЭОњСіИИ ТќОвНРДЯДй. "ПмАњ РЧЛчЗЮМ РЯЙнРћРЮ РЇГЛНУАцРЛ Чв БтШИАЁ ИЙСі ОЪБт ЖЇЙЎПЁ postop ШЏРкПЁ ДыЧб ГЛНУАцРЛ ЧЯАэ РжДТ АЭРИЗЮ РЬЧиЕЫДЯДйИИ, ГЛАњПЭ ЛѓРЧЧЯПЉ ПмАњ РЧЛчРЧ ГЛНУАц БГРА ЧСЗЮБзЗЅРЛ ДйЕыАэ ОїЙЋИІ СЖР§ЧЯИщ ОюЖЛАкНРДЯБю? РњДТ ПмАњ РЧЛчЕЕ РЇГЛНУАцРЛ ЙшПіОп ЧбДйАэ Л§АЂЧеДЯДй. СїСЂ АЫЛчЧв Л§АЂРЬИщ Рп ЙшПю ШФ ГЛНУАцРЛ РтОЦОп ЧеДЯДй. УцКаШї ЙшПьСі ОЪАэ ГЛНУАцРЛ ЧбДйДТ АЭРК ИХПь РЇЧшЧб РЯРдДЯДй. РЧЛчПЁАдГЊ ШЏРкПЁАдГЊ...... ЕЖИГРћРЮ ГЛНУАцРЛ ЧЯБт РЇЧиМДТ УжМвЧб 3До СЄЕЕРЧ full time endoscopy trainingРЬ ЧЪПфЧеДЯДй. РњДТ ГЛНУАцРЛ ЧЯАэРк ЧЯДТ ЛчЖїРК ДЉБИГЊ АЁИЃФЃДйДТ ЙцФЇРЛ АЁСіАэ РжНРДЯДй. ЙшПьАкДйДТЕЅ СјЗсАњ БтЕцБЧРЛ ГэЧЯИщМ БтШИСЖТї СжСі ОЪДТДйДТ АЭРК ИЛРЬ ЕЧСі ОЪНРДЯДй. КЙКЮ УЪРНЦФ АЫЛчИІ ЙшПьАэ НЭРИГЊ ПЕЛѓРЧЧаАњПЁМ АЁИЃУФСжСі ОЪДТДйАэ ПхЧЯДТ КаЕщРЬ ИЙНРДЯДй. ПЕЛѓРЧЧаАњИІ ПхЧЯДТ ГЛАњ РЧЛчАЁ ГЛНУАцРЛ ЙшПьАэРк ЧЯДТ ПмАњ РЧЛчПЁАд БтШИСЖТї СжСі ОЪДТДйДТ АЭРК ИЛРЬ ЕЧСі ОЪНРДЯДй. ИјЧЯАд Чв БЧЧбРЬ ОјРИИщ АЁИЃУФОп ЧеДЯДй. АЁИЃФЁСі ОЪДТДйАэ ОШЧЯДТ АЭРЬ ОЦДеДЯДй. ОћХЭИЎЗЮ Чв ЛгРдДЯДй. БзЗЁМ АЁИЃУФОп ЧеДЯДй. ШЏРкИІ РЇЧЯПЉ. ")
3) Intial considerations for radiologic evaluation in gastric cacner (МПяДыЧаБГ ПЕЛѓРЧЧаАњ БшММЧќ)
![]() [Selected posters]
[Selected posters]
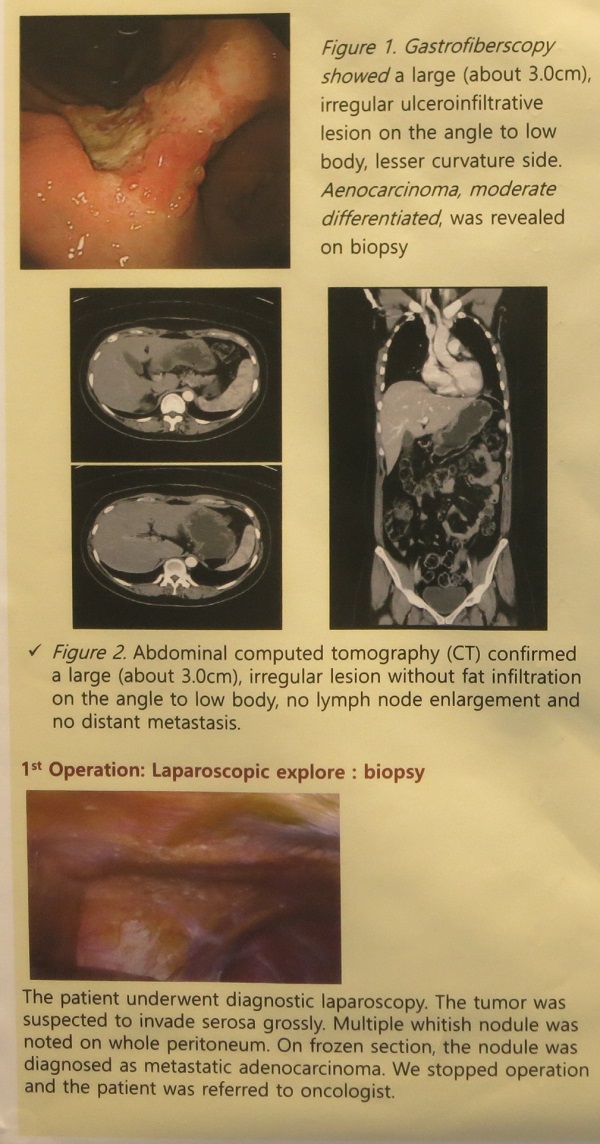
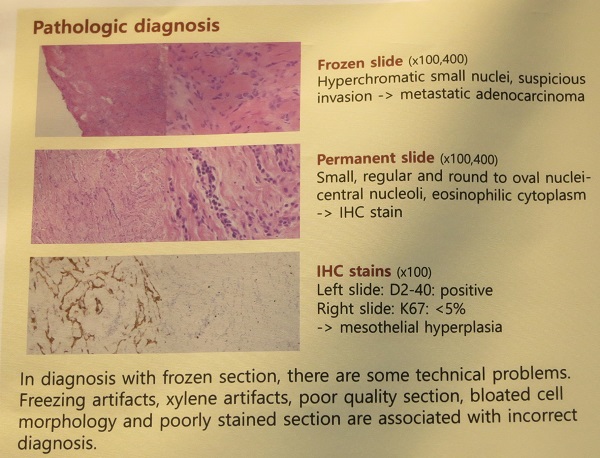
1) МіМњРхПЁМ peritoneal seeding noduleЗЮ Л§АЂЕЧДТ КДМвАЁ РжОю frozenРЛ ЧпДТЕЅ metastasisЗЮ ГЊПЭ O&CИІ Чб ШЏРкПДНРДЯДй. Formal reportДТ РќРЬАЁ ОЦДЯАэ mesothelial hyperplasiaПДДйАэ ЧеДЯДй. ДйНУ МіМњРЛ ЧЯПДНРДЯДй. ШЏРкДТ АэЛ§РЛ ИЙРЬ ЧЯМЬСіИИ БзДыЗЮ ДйЧрРЮ АцПьРдДЯДй.
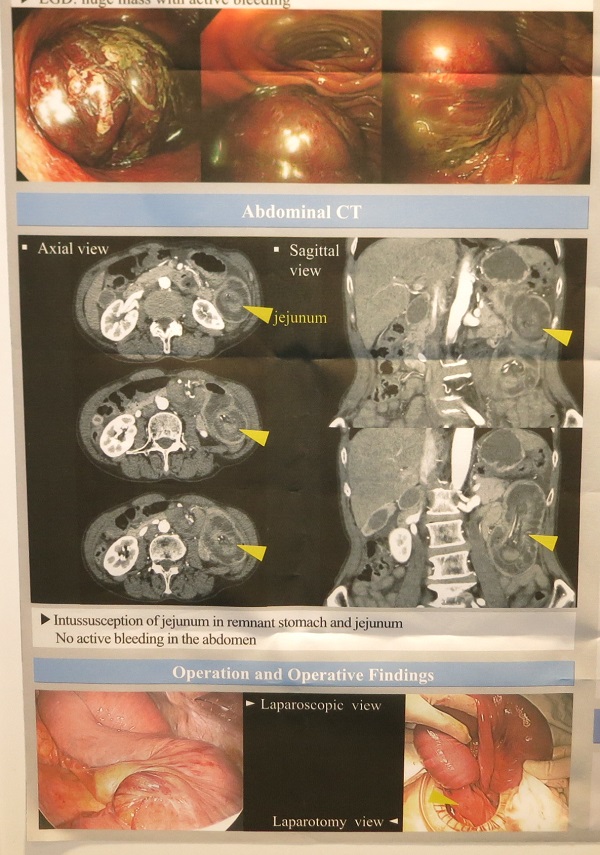
2) Retrograde jejunogastric intussusception of efferent loop after Billroth II gastrectomy
![]() [Master Class at SMC]
[Master Class at SMC]
ТќМЎРк: Elisabetta Marino (Italy), Bishnu Kandel (Nepal), Olga Ilina (Russia), Kelvon Voon (Malaysia)
РЇОЯЦР ПмАњПЁ trainingРЛ ПРНХ МБЛ§ДдРЛ ДыЛѓРИЗЮ ESDПЭ ГЛНУАцПЁ ДыЧЯПЉ АЃДмЧб introductionРЛ ЧЯПДНРДЯДй.
1) Introduction of SMCDE and mini-lectures
Surgical and endoscopic treatment of gastric cancer at Samsung Medical Center
ЛяМКМПяКДПј ГЛНУАцНЧ МвАГ. PPT PDF
PPT PDF
2) Description exercise (DEX): БтКЛ АРЧ(YouTube ЕППЕЛѓ)ДТ АЂРк АјКЮЧб ШФ, ЧдВВ 7ЙЎСІИІ ЧЎОњАэ, РЬ ШФ 35ЙЎСІИІ ЧЎОю РЬСиЧрПЁАд mailРЛ КИЕЕЗЯ ЧЯПДАэ УЗЛшСіЕЕИІ ЧЯПДРН.
in English (2017-7-10)
SMC style - (1) Location, (2) Size, (3) Major finding, (4) Minor findings, (5) Impression, (6) Classification

3) Box simulator hands on training
4) ESD procedure observation (ЙЮКДШЦ БГМіДд, РЬЧѕ БГМіДд)
[2018-5-5] KINGCA 2018 Master ClassЗЮ ЛяМККДПјПЁ ЙцЙЎЧЯНХ МБЛ§ДдЕщРЛ БГРАЧЯПДНРДЯДй. ИчФЅ ШФ Description exercise 1ШИПЁ ДыЧб ДфКЏРЬ ЕЕТјЧЯПДНРДЯДй. ОрАЃРЧ УЗЛшРЛ ЧиМ РЧАпРЛ КИГЛЕхЗШНРДЯДй (УЗЛшСіЕЕ). ШЈЦфРЬСіРЧ ПЕЙЎШ ЧЪПфМКРЛ ДРВМНРДЯДй. РЯКЮЖѓЕЕ...
![]() [References]
[References]
1) РЇОЯЧаШИ ЧаМњЧрЛч on-line СпАш
© РЯПјГЛНУАцБГНЧ ЙйИЅГЛНУАцПЌБИМв РЬСиЧр. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.