 EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [APDW 2016]
[APDW 2016]
내용이 매우 좋고 잘 준비된 학회였습니다. 다만 우리나라 참석자가 적다는 점이 아쉬었고, 중국 사람이 너무 많다는 점이 위협적이었습니다. 인도 사람도 엄청 늘었습니다.
APDW 등록비가 4만엔 (약 44만원)으로 다소 비싼 편입니다. 김영란 법의 영향으로 학회 참석 지원이 대폭 축소되어 APDW에 참석한 우리나라 의사가 줄어든 것 아닌가 생각되었습니다. 저도 학회 지원을 받으려고 신청서를 냈다가 탈락하여 자비로 참석하였습니다.
저는 마지막 날 Poster presentation 세션 좌장을 할 예정인데, 일본 학회 측에서는 좌장에 대한 수고료도 주지 않습니다. 이번에 강의하신 선생님들에게는 강의료도 없다고 합니다. 해외 유명 학회는 다들 비슷합니다. '불러서 강의할 기회를 준 것을 영광으로 알아라. 강의료는 없다.' 뭐 이런 식입니다.
다음 APDW는 2017년 홍콩, 2018년 우리나라입니다.
일본인의 준비 정신은 대단합니다. 2017, 2018, 2019, 2020년 JDDW 일자와 장소가 벌써 공지되었습니다.
2017년 10월 12일 - 10일 15일. JDDW (Fukuoka)
2018년 11월 1일 - 11일 4일. JDDW (Kobe)
2019년 11월 21일 - 11일 24일. JDDW (Kobe)
2020년 11월 5일 - 11월 8일. JDDW (Kobe)
이번 APDW를 준비하면서 일본 학회 측에서는 funding에 상당한 어려움을 겪었다고 합니다. 일본 학회인 JDDW에는 funding이 충분했지만 국제학회인 APDW에는 funding이 별로 없었기 때문입니다. 국내 학회는 무시하고 국제 학회만 중시하는 우리의 모습과는 정반대의 모습입니다. 우리나라가 더 발전하려면 우리 자신에 좀 더 집중할 필요가 있다고 생각됩니다. 사대주의를 극복해야 합니다.
일본에는 참 학술 모임도 많습니다. 우리나라와 비슷하게 sub 학회가 흥하고 main 학회는 망해가는 분위기라고 합니다.
Digital poster presentation. 차병원 조주영 교수님 팀 발표
Koken에서 새로운 내시경 훈련 모델을 선보였습니다. 문제는 가격입니다(5,000 달러). 참고: EndoTODAY Simulator를 이용한 내시경 교육
Satellite symposium
APDW 마지막 날 포스터 세션 (Digital Poster, Stomach and Duodenum "Neoplasia 8" Booth No. 2)의 좌장을 보았습니다. 함께 하신 분은 Jichi 대학의 Hiroyuki Osawa 선생님이었습니다. 직접 제가 발표한 한 개의 포스터(DP-0844)를 포함하여 8개의 연제가 있었는데, 그 중 한 발표자가 나타나지 않았습니다. No Show! 우리나라 사람이었습니다. 너무 창피해서 쥐구멍이라도 찾고 싶었습니다. 저의 좌장/발표의 앞 세션에서도 9명 중 한 명의 발표자가 나타나지 않았는데, 그 또한 우리나라 사람이었습니다.
이번 학회 기간에 구연과 포스터를 여럿 제출하여 열심히 발표하고 토론하신 우리나라 선생님들이 많았습니다. 보기 좋은 모습이었고 무척 흐뭇했습니다. 그러나 여전히 예정된 포스터 발표 현장에 나타나지 않아 국가적인 망신을 자초하는 사례가 적지 않았습니다. 물론 이해합니다. 바쁘게 일하다 모처럼 외국에 나오셨을 것이고, 학회 마지막 날이고, 날씨는 너무 좋았고, 가까운 곳에 오사카와 교토가 있으니 가보고 싶었을 것입니다. 가족들 선물도 사야 했을 것입니다. 빨리 귀국하여 한국에서 당직 근무를 해야 하는 사정이 있었을 수도 있습니다. 다 이해합니다.
그러나... 약속은 지켜야 합니다. 포스터 발표를 하겠다고 초록을 제출했으면 예정된 시간에 현장에 나타나 발표를 해야 합니다. 학회측에서 여러번 메일을 보냈기 때문에 몰랐을 수 없습니다. 약속을 지키지 않으면 한 걸음도 앞으로 나갈 수 없습니다. 약속을 지키는 것은 모든 윤리의 시작이니까요. 우리나라 의료가 지금처럼 왜곡된 이유 중 하나도 서로 약속을 지키지 않았기 때문입니다.
김영란법 영향으로 학회 지원으로 APDW에 참석한 사람은 많지 않습니다. 적어도 그분들은 정상적으로 구연 혹은 포스터 발표를 했을 것으로 믿고 싶습니다. 자비로 참석했더라도 no show는 안되는 일이지만, 남의 돈으로 외국에 나와 약속을 지키지 않은 것은 있을 수 없는 일입니다.
지난 봄 일본소화기내시경학회(동경)에서 우리나라 사람들이 포스터 발표에 no show를 한 적이 있어서 공개적으로 문제제기를 하였습니다. 학회 지원으로 외국에 와서 no show는 말이 되지 않는다고 큰 목소리로 외쳤던 기억이 생생합니다. 그러나 아직 고쳐지지 않았습니다. 우리 모두 크게 반성해야 합니다. 다 우리 교수들 잘못입니다. 잘 못 가르친 탓입니다. 제 스스로 크게 반성하였습니다.
기분 좋게 출발하여 기분이 엉망인 상태로 귀국하였습니다. 너무 창피했습니다. 다시는 no show를 하지 맙시다. 약속을 지킵시다.
해외 학회에서 사전 통보 없이 예정된 발표를 하지 않아 우리나라의 위신을 크게 추락시킨 사태를 알리는 편지를 드린 바 있습니다 (관련 링크). 학회 발표를 빵꾸내는 것은 중국 사람들이나 하는 일로 알았는데, 우리나라 의사 중 no show를 가볍게 여기는 분들이 계신다는 것은 개탄스러운 일입니다. 차라리 요즘은 중국사람들이 더 열심히 발표하는 것 같습니다.
개인 돈으로 학회에 참석하였더라도 용서하기 어려운 일인데, 혹시 공금을 지원받은 분이 '발표 빵꾸'를 한 것은 아니었는지 궁금합니다. 이번 학회에서는 발표 직후 현장에서 '발표 인증서(certificate of presentation)'를 나누어주었습니다. 학회에서 회원의 해외 학회 발표를 지원한 경우에는 적어도 '발표 인증서' 정도는 제출케 하는 것이 어떨까 싶습니다. 인증샷도 좋구요.
이준행 포스터 구연 발표 인증서
다시는 이와 같은 창피한 일이 없기를 바랍니다. (2016-11-7. 이준행)
![]() 1. PG course - upper GI
1. PG course - upper GI
학회장에 도착하니 상부 PG course가 벌써 절반 정도 진행된 상태였습니다.
4) GI cancer and diet (함기백)

(1) Helicobacter 제균, (2) diet intervention, (3) COX inhibitors, PPIs, natural products를 통하여 tumor microenviornment를 조절할 수 있습니다.
PPI가 위암 세포의 apoptosis를 유도할 수 있습니다 (Yeo M. Clin Cancer Res 2004).
Revaprazan이 anti-inflammaotry 효과가 있습니다 (Lee JS. J Clin Biochem Nutr 2012).
Cancer preventive kimchi에 대해서 잠깐 언급하셨습니다 (Jeong M. Oncotarget 2015),
![]() 2. PG course - lower GI
2. PG course - lower GI
1) Current issues in biological therapy for IBD (양석균, 울산대학교)

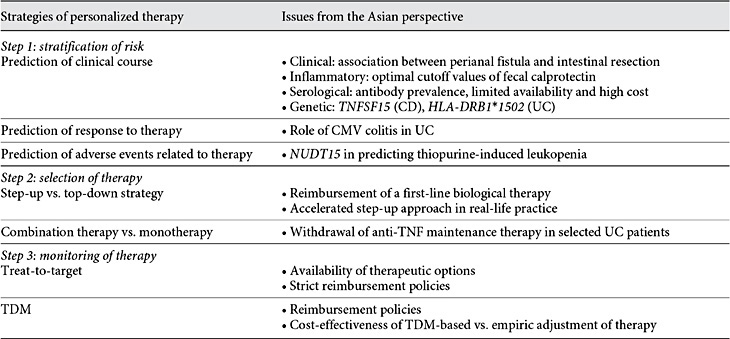
양교수님은 기존 방법의 장단점을 요약한 후 early introduction of anti-TNF agents, combination therapy with immunomodulators, therapeutic drug monitoring (TDM), treat-to-target strategy, personalized IBD therapy (Yang. Dig Dis 2016)를 설명하셨습니다.
이어서 새롭게 개발되고 있는 integrin antibdody나 small molecule inhibitor를 설명하셨습니다. (강의는 멋졌는데 제가 요약할 능력이 없어 죄송합니다.^^ 사진도 못 찍게 해서...)
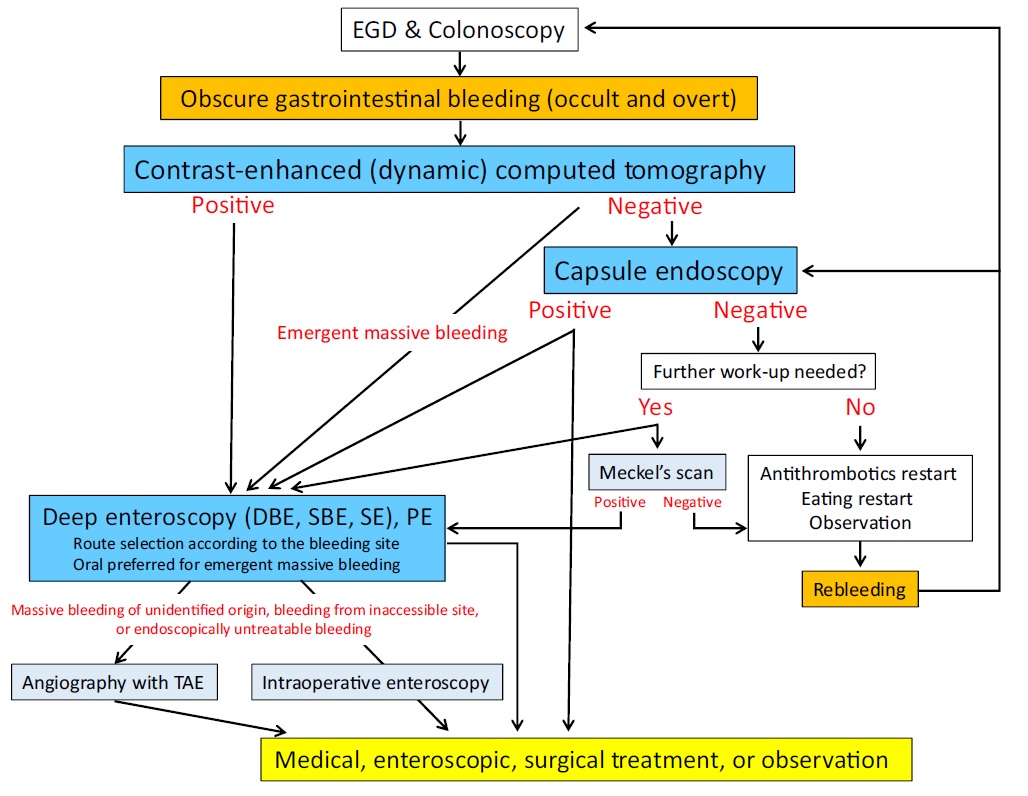
2) How to find and treat small bowel bleeding (Naoki Ohmiya)
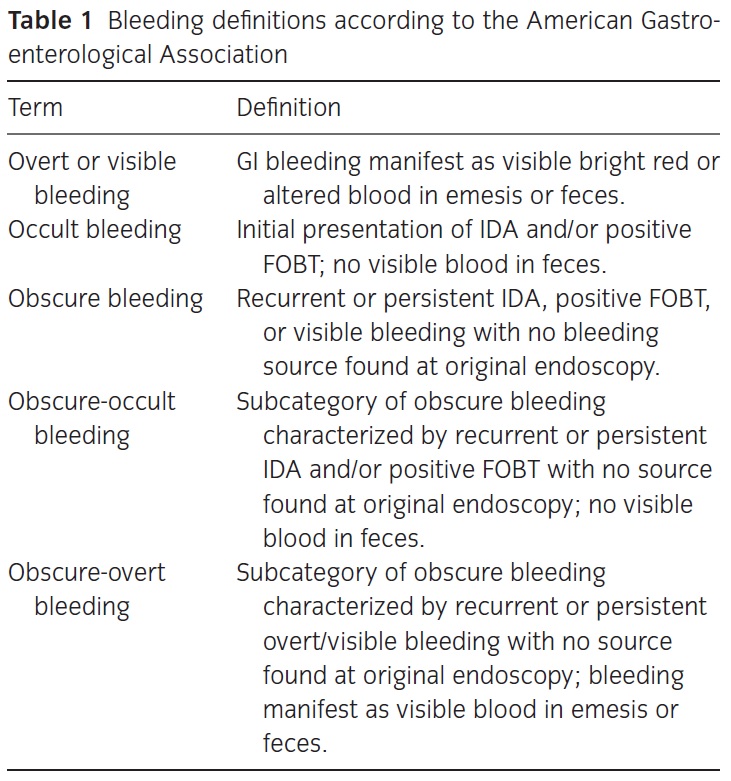
Occult와 overt GI bleeding의 원인이 크게 다르지 않으므로 Ohmiya 선생님은 둘을 구분하지 않는 algorithm을 제안하였습니다. Obscure GI bleeding (overt and occult)에서 가장 먼저 chest-pelvic plain X-ray & contrast-enhanced CT를 첫번째 검사로 제안하였습니다.
저는 다음과 같은 질문을 했습니다. "In my opinon, the role of abdominal CT has been underestimated in the evaluation of obscure GI bleeding. So, I am very happy to see your algorithm. My question is what kind of CT do you recommend; just routine contrast-enhanced CT or CT angiography." 연자는 같은 생각을 가지고 있다고 답하면서, 자신도 capsule endoscopy나 enteroscopy 전에 CT를 시행하고 있다고 답하였습니다.
Active bleeding의 경우에는 small bowel enteroscopy를 바로 시행하는 것이 더 좋지 않은지 floor에서 질문이 있었습니다. 연자는 CT는 다소 고가이지만 쉽게 시행할 수 있다고 답하면서 "CT is the first diagnostic tool in Japan." 이라고 주장했습니다. 상부 내시경과 하부 내시경에 이상이 없을 때 capsule endoscopy나 small bowel enteroscopy로 넘어가기 전 CT부터 찍자는 연자의 주장에 전적으로 동의합니다.
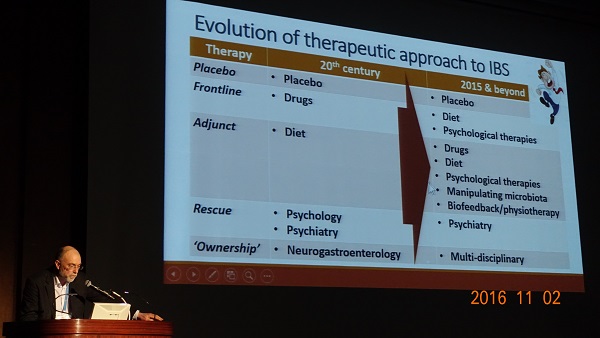
3) Progress in IBS treatment (Peter Gibson)
Gibson 박사는 FODMAPs으로 유명한 분입니다. 역시 강의 내내 IBS 관리에 있어서 음식의 중요성을 강조했습니다. 다만 지나친 음식 조절은 food-related quality of life를 나쁘게 할 수 있다고 하네요.^^
Psychotherapy, behavioral modificaiton, gut-directed hypnotherapy 등을 잠깐 다룬 후 microbiota에 대해서는 rifaximin, probiotics, prebiotics, fecal transplantation을 언급했습니다.
'Don't forget other contributors to chronic diarrhea'라는 슬라이드에서는 exocrine pancreatic insufficiency, bile salt malabsorption 등을 강조하였습니다.
4) Management of colon diverticular disease (Nobuyuki Matsuhashi)
일본에서는 과거 diverticulum이 주로 우측 대장에서 발견되었으나 최근에는 서양과 비슷하게 좌측 대장에서 발견되는 예가 점차 증가하고 있다고 합니다 (NTT 병원 자료를 보여주셨습니다. Left alone 과 left + right가 거의 절반이었습니다. Right alone은 여전히 절반이지만.)
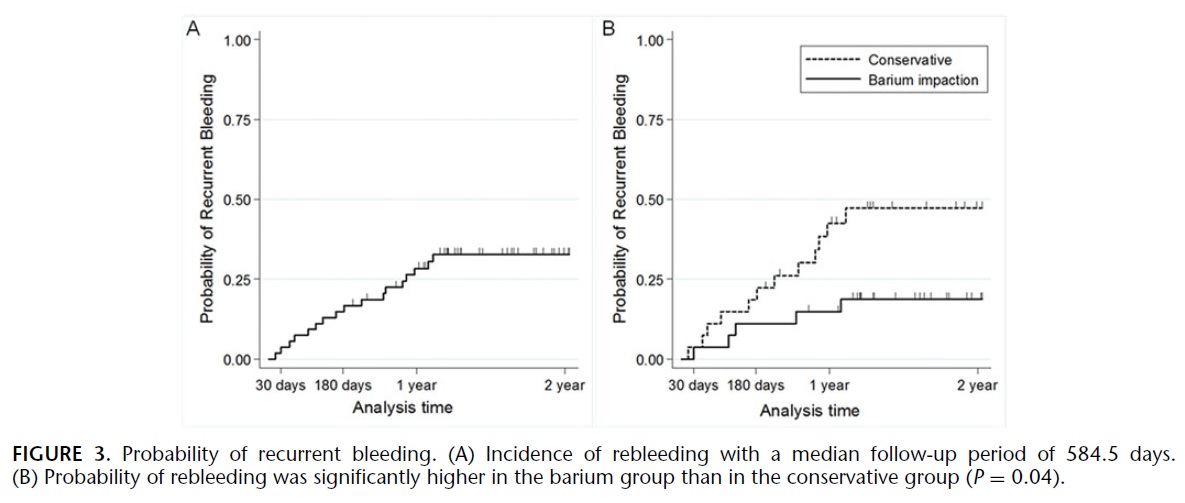
출혈 위치를 알 수 없는 환자에서 barium impaction이 도움이 된다고 합니다 (Nagata N. Ann Surg 2015). 무척 신기한 치료입니다. 게실을 고농도 바륨으로 filling 해버린다는 발상같은데요...
High-dose barium impaction therapy for the recurrence of colonic diverticular bleeding: a randomized controlled trial. (Nagata N. Ann Surg 2015)

Median follow-up period was 584.5 days. The probability of rebleeding at 30-day, 180-day, 1-year, and 2-year follow-up in all patients was 3.7%, 14.8%, 28.4%, and 32.7%, respectively. By group, probability at 1 year was 42.5% in the conservative group and 14.8% in the barium group (log-rank test, P = 0.04). After adjustment for a history of hypertension, the hazard ratio of rebleeding in the barium group was 0.34 (95% confidence interval, 0.12-0.98). No complications or laboratory abnormalities due to barium therapy were observed. Compared with the conservative group, the barium group had significantly (P < 0.05) fewer hospitalizations per patient (1.7 vs 1.2), units of blood transfused (1.9 vs 0.7), colonoscopies (1.4 times vs 1.1 times), and hospital stay days (15 days vs 11 days) during the follow-up period. No patients died and none required angiographic or surgical procedures in either group.
NSAID와 opoid는 게실 천공을 유도할 수 있고, 반대로 calcium channel blocker는 천공을 막는 효과가 있다고 합니다.
* 참고: EndoTODAY 게실염
![]() 3. State-of-the-art lecture (2016-11-3. 8:30am)
3. State-of-the-art lecture (2016-11-3. 8:30am)
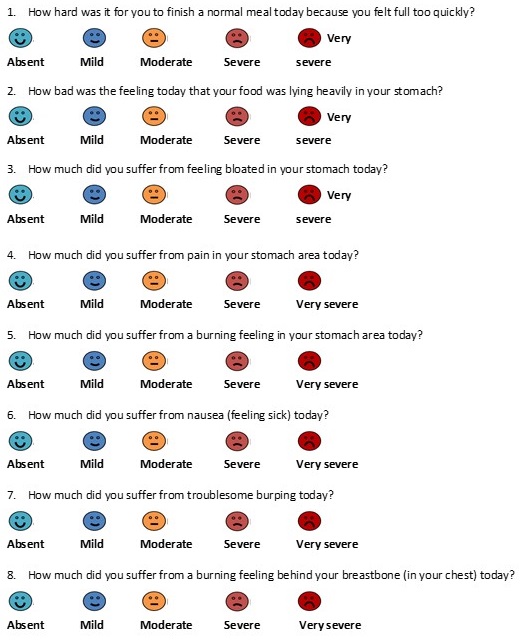
1) Functional dyspepsia (Jan Tack)
증상 평가에서 pictogram을 이용할 수 있습니다 (Tack. APT 2016).
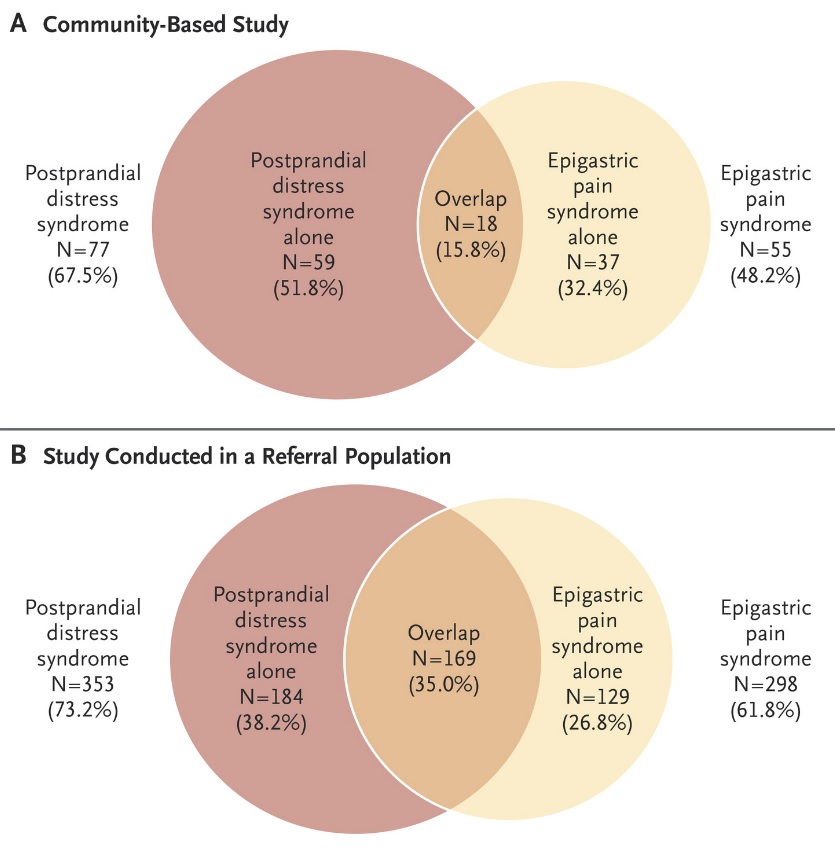
PDS와 EPS은 상당히 구분되는 질환으로 overlaping은 생각보다 적습니다. Recognition of meal-relation should decrease overlap. PDS에도 어느 정도 postprandial pain이 가능합니다.
Postprandial distress syndrome and postprandial distress syndrome/epigastric pain syndrome overlap groups in the validation study of the Leuven Posptrandial Distress Scale. The graph on the left depicts the proportion of the 60 enrolled patients who fulfill Rome III criteria for pure postprandial distress syndrome and those who fulfill both postprandial distress syndrome and epigastric pain syndrome criteria. The graph on the right illustrates that the co-existing epigastric pain syndrome symptoms that are related to meal ingestion in the vast majority of patients. (Tack. APT 2016)
PDS는 prokinetics로 EPS는 PPI로 치료를 시작합니다. EPS group에서는 H. pylori 제균치료가 도움이 됩니다.
탁 선생님은 Kyoto consensus를 소개했습니다. Hp (+) FD에서 모두 제균을 하자는 것이 일본 의견이지만 (아래 그림), 탁 선생님은 Hp (+) FD 중 EPS subgroup에서만 제균치료를 하자는 슬라이드를 보여주었습니다.
(Gut 2015)
[이준행 주] 관련하여 최근 NEJM 리뷰 중 FD에서 Helicobacter 치료에 대한 부분을 옮깁니다.
Although 5% of the cases of dyspepsia in the community are attributable to infection with H. pylori, the effect of eradication therapy on the symptoms of functional dyspepsia is modest. In a meta-analysis of 17 randomized trials, involving 3566 patients, the relative risk of persistent symptoms was 0.90 (95% confidence interval [CI], 0.86 to 0.94), with a number needed to treat of 15. Nevertheless, economic modeling that was based on these data suggests that eradication therapy is a cost-effective strategy for managing functional dyspepsia. Evidence continues to accumulate that such therapy is beneficial. A trial assessing the effect of eradication therapy according to individual symptoms reported by the patient showed a significant effect on epigastric pain and burning but not on early satiety or postprandial fullness. These data suggest that the benefit of eradication therapy may be more pronounced in patients with the epigastric pain syndrome than in others.
Prucalopride는 gastric emptying을 촉진합니다 (정상인에게 prucalopride를 투여하고 barostat 검사를 한 적이 있는데 상당수가 검사를 견디지 못하고 중단했다고 합니다. Nausea, vomiting이 심해서). Prucalopride는 nausea/vomiting, fullness/satiey, bloating/distention를 개선한다는 미발표 자료가 있습니다. 그러나 증상 개선과 gastric emptying 개선과는 상관이 없었습니다.
Gut hypersensitivity가 중요할 것 같습니다. Hypersensitivity도 fasting hypersensitivity와 postprandial hypersensitivity로 나눌 수 있습니다.
탁 선생님은 Accomodation이 중요한데 이 부분에 대한 연구가 부족하다는 점을 지적하면서 강의를 마쳤습니다. Barostat 검사가 너무 힘들어서 연구가 어렵습니다. MRI volemtry가 가능하지만 specialized center에서만 적용할 수 있습니다. Drink test가 간단하고 유용합니다. Intragastric pressure monitoring이 새로운 방법으로 시도되고 있습니다 (Carbone라는 분의 학위 논문이고 아직 미발표).
2) Gastric motility disorder and dyspeptic symptoms (PJ Pasricha)
An overarching disease model of functional dyspepsia. Talley. NEJM 2015
Gastroparesis clinical research consortium (GpCRS) 연구입니다. 증상 변화의 예측인자 중 overweight/obesity 등 몇 가지 인자는 증상 개선 가능성을 낮춥니다 (Pasricha. Gastroenterology 2015).
파 선생님은 2015 Gastroenterology 연구를 바탕으로 (1) 체중감소, (2) depression 치료, (3) 금연이 중요할 것 같다고 언급하였니다. (이준행 독백: "당연한 것 아닌가요? 그걸 알려고 그 복잡한 registry 연구를 했습니까? 살빼고 금연하면 건강이 좋아집니다.")
NK1 receptor antagonist (aprepitant)가 유망합니다.
Gastroparesis 발생에 macrophage가 중요한 역할을 합니다. Macrophage에는 good macrophage가 있고 bad macrophage가 있습니다. 나쁜 macrophage가 activation되어 ICC loss/dysfunction이 발생하여 gastroparesis가 된다는 설명입니다.
파 선생님은 gastroparesis와 FD의 상관관계에 대하여 Talley. NEJM 2015를 인용하셨습니다.
There is also overlap between symptoms of functional dyspepsia and those of gastroparesis. More than one in four patients with functional dyspepsia have evidence of delayed gastric emptying, and in one study 86% of the patients with gastroparesis met the criteria for functional dyspepsia, which suggests that these conditions share similar pathophysiological features; the degree of overlap of symptoms also means that the capacity of diagnostic tests such as gastric scintigraphy to discriminate between functional dyspepsia and gastroparesis is limited.
Gastroparesis and functional dyspepsia may be part of the same spectrum of pathology. - "a macrophage driven Cajalopathy"
![]() 4. Ultramagnifying endoscopy (Kudo, 2016-11-3. 10:20am)
4. Ultramagnifying endoscopy (Kudo, 2016-11-3. 10:20am)
Barium study로는 subtle depressed lesdion을 찾기 어렵습니다.
1년만에 typical apple core lesion을 보였습니다. 좌측 사진의 좌측 중간 점막이 약간 irregular하다는 것이 첫 검사에서 간과된 경우입니다.
구도 선생님은 35년간 25만예의 colonoscopy를 하셨습니다. 대단합니다.^^
2002년 12월 파리에서 미팅 후 Paris classification을 만드셨습니다.
PPT PDF 0.4 M
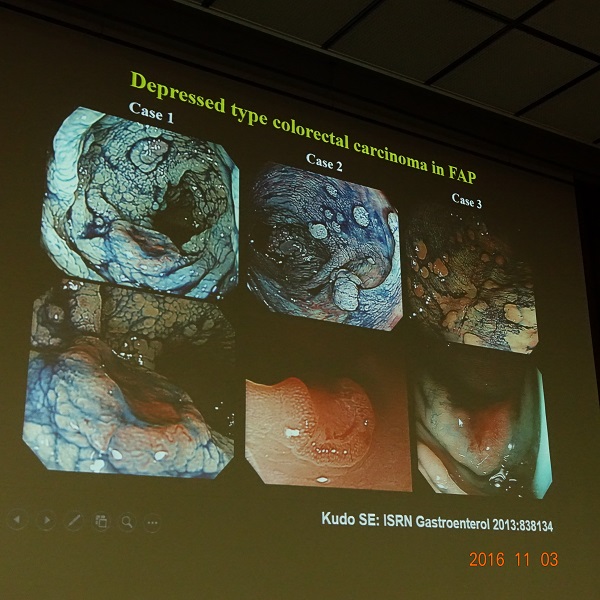
Depressed type colorectal cancer in FAP (Kudo SE. ISRF Gastroenterol)
Ultramagnifying endoscopy에 대한 EC classification을 소개하셨습니다. (Kudo. GIE 2015)
EC-V (endocytoscopic vascular pattern)
EndoBRAIN: 일종의 CAD (computer-aided diagnosis)입니다 (Mori & Kudo. GIE 2015). 향후 병리과 의사를 대처하게 될지도 모릅니다.
구도 선생님은 "Diagnosis of IIc is not yet complete throughout the world."라는 말로 강의를 마치셨습니다. 앞으로도 할 일이 많다는 뜻 같았습니다.
* 참고: EndoTODAY 확대내시경
![]() 5. Role of gastroenterology in the primary prevention of diseases - opportunity and challenge (Kentaro Sugano. Jichi Medical University) - 예정된 좌장(고 선생님)이 나타나지 않아서 다른 분이 대신 좌장을 보셨습니다. 약간 황당한 일입니다.
5. Role of gastroenterology in the primary prevention of diseases - opportunity and challenge (Kentaro Sugano. Jichi Medical University) - 예정된 좌장(고 선생님)이 나타나지 않아서 다른 분이 대신 좌장을 보셨습니다. 약간 황당한 일입니다.
1) Helicobacter and peptic ulcer
Effect of low dose (15mg) lansoprazole. Sugano K. J Gastroenterol 2012
LAVENDER trial. Sugano K. Gut 2014
[이준행 주] LAVENDER tiral에 대해서는 몇 년 전 제가 commentery를 쓴 적이 있습니다. 참고하시기 바랍니다.
2) Helicobacter and gastric cancer
일본에서는 2001년 Hp 제균치료에 대한 보험급여가 시작된 후 매년 60만명 정도가 Hp 제균치료를 받았습니다. 2013년에 제균 적응증이 확대(Hp gastritis가 포함됨)된 후 매년 140만명정도가 Hp 제균치료를 받고 있습니다. 일본에서 현재 제균치료 적응증은 60% 정도가 Hp gastritis입니다. 감염자와 위암 환자가 현저히 줄 것으로 예상됩니다. (Hiroi et al - in submission). 실제로 일본에서는 2011년부터 위암 사망자가 줄고 있습니다.
3) Obesity
수 선생님은 "Visceral obesity should be managed by gastroenterologiests."라고 주장하셨습니다. NSFLD, GB stone, GERD, Barrett, diabetic gastropathy, IBD, colon polyp/cancer, pancreatitis/cancer 등이 모두 obesity와 관련되어 있으므로 소화기내과 의사가 빠질 수 없다는 것이지요. 최근에는 gut microbiota도 이슈가 되기 때문에 더욱 그렇다고 합니다. Dysbiosis라는 용어를 소개하셨습니다 (Wang ISMEJ 2012).
4) Enviornmental gastroenterology
헬리코박터 제균치료를 시작하기 이전부터 헬리코박터 감염률은 감소하고 있었고, 위암 발생률이 줄고 있었습니다. 환경이 개선되었기 때문입니다. 수 선생님은 Enviornmental gastroenterology라는 용어를 쓰셨습니다.
Enviornmental approaches are most costeffecive in disease prevention. (Chokshi DA. NEJM 2012)
Silent Spring (Rachel Carson. 1962)이라는 유명한 책을 소개하셨습니다. 우리나라에서는 '침묵의 봄'으로 번역된 책입니다.
수 선생님은 "Man has lost the capacity to foresee and to forestall. He will end by destroying the earth."라는 Albert Schweitzer의 말을 인용하며 강의를 마치셨습니다. 멋진 강의였습니다. 짝짝짝^^^
![]() 6. [Luncheon symposium - Fujifilm] New endoscopy system to diagnosis for upper GI tract (Ryoji Miyahara. Nagoya University Graduate School of Medicine. Japan)
6. [Luncheon symposium - Fujifilm] New endoscopy system to diagnosis for upper GI tract (Ryoji Miyahara. Nagoya University Graduate School of Medicine. Japan)
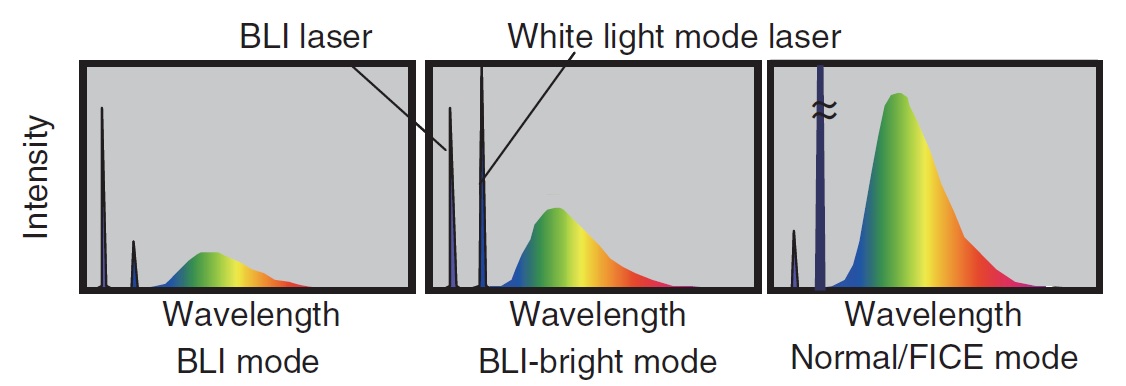
미 선생님은 Fujifilm 사의 LASEREO system을 소개하셨습니다.
PDF 3.4 M
LCI (linked color image) mode
BLI (blue light image) mode - 과거의 blue light laser mode와 약자가 같아서 헷갈리기 쉽습니다.
LED (light emitting diode) - 나고야 대학 소속인 미 선생님은 LED에 대한 연구로 2014년 노벨 물리학상을 받은 일본인 학자 2명이 나고야 대학 출신이라고 자랑스럽게 소개했습니다. Multi-light technology를 적용한 LED light source (Fujifilm 7000 system)는 과거의 표준이었던 Xenon light source와는 상당히 다른 spectrum을 가지고 있습니다. White light에 비하여 short wavelength light가 강화되어 microvascular structure가 더 잘 보인다고 합니다.
Fujifilm 내시경의 손잡이 부분은 G7이라고 부르는데 ergonomic 측면을 많이 고려하여 설계되었기 때문에 내시경을 많이 하더라도 아프지 않다고 합니다.
![]() 7. Image enhanced endoscopy (Tajiri. Jikei University)
7. Image enhanced endoscopy (Tajiri. Jikei University)
식도암 깊이 예측 분류. Oyama. Esophagus 2016
확대내시경은 두 가지 방법이 있습니다. 기존에는 Zoom lever operation (85-110 times) 방식을 사용하였는데 최근 내시경에는 Dual focus (45-65 times) 방식이 적용되고 있습니다. 확대 비율은 조금 낮지만 편하니까.
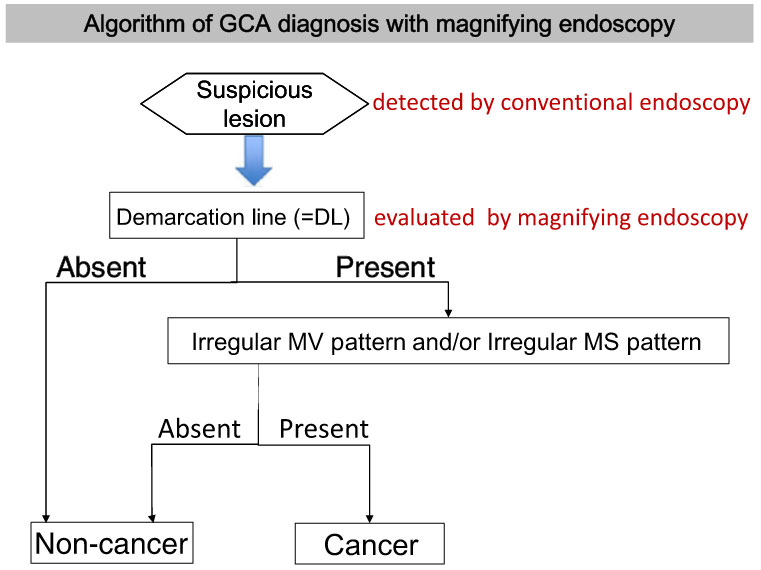 타 선생님은 demarcation line을 자세히 설명하셨습니다.
타 선생님은 demarcation line을 자세히 설명하셨습니다.
White globe appearance (WGA)라는 새로운 개념을 소개하셨습니다.
DRI (Dual Red Image): NBI와 달리 주로 붉은 쪽 스펙트럼을 사용하여 깊은 vessel을 잘 볼 수 있습니다.
LCI (Linked Color Image): 붉은 색은 더 붉게, 밝은 부위는 더 밝게 보여주므로 Helicobacter 감염에 의한 diffuse redness를 더욱 잘 볼 수 있습니다.
PDD (Photo-Dynamic Diagnosis): to visualize cancer porphobilinogen
EndoBRAIN: Endocytoscopy 영상을 컴퓨터로 real time으로 분석하는 CAD (computer-aided diagnosis). 타 선생님은 EndoBRAIN을 통하여 향후 resect and discard 전략을 초보자도 사용할 수 있을 것이라고 전망하였습니다 (그러나 오전 강의에 Kudo 선생님은 아직은 resect and discard 전략은 너무 위험하다고 언급하면서, 절제한 모든 조직을 병리과로 보내고 있다고 말하였습니다).
![]() 8. ESD education
8. ESD education
1) ESD training in Japan (Tsuneo Oyama, Saku central Hospital) - Hook knife의 개발자
외국 의사에게 인간을 대상으로 한 ESD 훈련을 불가능하다고 합니다. 돼지 胃를 이용하여 훈련을 시킬 수 있습니다. 돼지 위를 규칙적으로 눌러주어서 마치 환자에서 ESD를 하는 것과 비슷한 효과를 내야 합니다.
(1) Point, (2) line, (3) plane 개념을 이해하여야 합니다.
Three hand technique: 우측 손으로 내시경 삽입부를 잡으면서 동시에 catheter를 잡는 방법
Jet hook knife: catheter를 교체할 필요가 없는 새로운 Hook knife
Clip with line technique: 오 선생님은 거의 모든 ESD에서 clip with line을 사용한다고 합니다.
식도 게실을 둘러싼 표재성 식도암을 thoracoscopy를 이용하여 게실은 자르고 그 주변 식도암은 ESD로 치료하는 장면을 보여주셨습니다. Deep muscle layer를 ESD 하였기 때문에 큰 천공이 발생하였고 thoracoscopy로 닫아주었습니다. (이준행 독백: 그냥 thoracoscopy로 segmental resection 해도 좋을 것 같은데 왜 이런 고생을 하는지 이해할 수는 없었습니다)
Diagnosis is important.
High quality of pathology is important.
2) ESD training in Korea (이용찬, 연세대학교)
2014년 한국의 tertiary hospital에서 위암의 32.7%가 내시경으로 치료되었습니다. Stage 1A의 45%가 내시경으로 치료되었습니다.
Learning curve에 대한 최근 연구들은 과거보다 더 많은 경험이 쌓여야 proficient 하다고 할 수 있다는 결론을 내고 있습니다.
좌장인 Yahagi 선생님은 isolated pig stomach이 좋은 starting point라고 comment 하셨습니다.
3) ESD training in Taiwan (Wang)
타이완에서는 식도암이 5년 사이에 14.5%가 감소하였습니다.
Taiwan ESD Registry by DEST from 2015 (이준행 독백: 타이완 의료는 사회주의 성향이 강하여 registry가 잘 됩니다. 타이완에서 ESD registry가 시작되었다니 살짝 걱정됩니다. )
Endoscopy training center가 3 곳에 만들어졌다고 합니다. 주로 동물 모델로 연습하는 곳입니다. Procedure를 모두 녹화하여 시술자에게 보내줍니다. 천천히 review 할 수 있는 기회를 주는 것인데 매우 좋은 tip이라고 생각되었습니다.
POEM training을 위해서 certificate 제도를 만들었다고 합니다. 국민들이 webpage에서 certified POEM 시술자를 검색할 수 있다고 합니다.
* 이준행 comment: "So the Taiwan government required certification system for POEM, but not for ESD. The major concern of POEM is complication, but the major concern of ESD is oncological outcome. If certificate system is required, it is ESD not POEM."
4) Europe (Ponchon, Current President of ESGE, Lyon, France)
Systemic training이 시작하기 전 유럽에서 ESD perforation rate는 10-18%에 이르고 있습니다.
Minimal treaining requirements; (1) basic knowledge, (2) visit to experts (observation of a minimum of 15 live procedures). (3) Hands-on training on a model of islated pig stomach (minimum of 30 resections), (4) Hands-on training on liver pigs (minimum of 5 resections), (5) Minimal case load: 10-20 cases/year
Pioche M. Endoscopy 2016 - Yahagi 선생님이 제공한 software를 이용하여 훈련받은 trainee들이 complete resection에서 훨씬 좋은 결과를 보였습니다.
포 선생님은 "Not genetic but training"을 세번 강조하였습니다. (이준행 독백: genetic은 아닐지 몰라도 social factor를 무시하면 안 것 같습니다. 극단적으로 꼼꼼한 문화를 유지하고 있는 일본의 ESD를 서양 사람들이 완전하게 배우는 것은 불가능할 것 같습니다.)
![]() 8. Maastricht V Florence Consensus Report (Malfertheiner P. Gut 2016 on-line )
8. Maastricht V Florence Consensus Report (Malfertheiner P. Gut 2016 on-line )
Contributor에 동양 사람이 많았습니다. 그런데 아쉽게도 한국인은 없었습니다. 지나치게 strict한 Helicobacter 제균치료 적응증으로 관련 의사/연구자를 제약해온 정부 정책이 중요한 원인 중 하나라고 생각합니다. 국가 위상에 비하여 Helicobacter 관련 연구가 너무 부족한 실정입니다. 오늘 강의에서 많은 논문이 인용되었는데, 우리나라 논문은 하나도 없었습니다. 빨리 심평원 적응증이 확대되어야 할 것 같습니다.
적응증 Statement 2: A test-and-treat strategy is appropriate for uninvestigated dyspepsia. This approach is subject to regional H. pylori prevalence and cost-benefit considerations. It is not applicable to patients with alarm symptoms or older patients.
: 가장 근심스러운 문장이었습니다. 일본 가이드라인과 Maastricht 5의 차이점입니다. 일본에서는 내시경 검사 없이 치료하는 것을 인정하지 않고 있습니다. 우리나라에서는 test-and-treat는 너무 위험하다고 생각합니다.)
적응증 Statement 5: H. pylori gastritis is a distinct entity and causes dyspeptic symptoms in some patients. H. pylori eradication produces long-term relief of dyspepsia in about 10% of patients in comparison to placebo or acid suppression therapy.
: FD 환자에서, 특히 EPS subtype FD에서 제균치료는 어느 정도 효과가 있습니다. Maastricht V에서는 FD의 subtype과 무관하게 제균치료를 하도록 권하고 있습니다.
진단 Statement 3: In clinical practice when there is an indication for endoscopy, and there is no contraindication for biopsy, the rapid urease test (RUT) is recommended as a first-line diagnostic test. In the case of a positive test, it allows immediate treatment. One biopsy should be taken from the corpus and one from the antrum. Rapid urease test (RUT) is not recommended as a test for H. pylori eradication assessment after treatment.
: H. pylori를 보기 위한 조직검사는 두개를 하라는 것입니다 (전정부에서 하나 위체부에서 하나). Rapid urease test는 첫 내시경에서 H. pylori 감염 여부를 검사할 때에는 사용하지만 제균 여부를 확인하기 위해서는 사용하지 말 것을 권하고 있습니다. Rapid urease test에 대해서는 좀 더 자세한 설명이 있어서 옮깁니다. H. pylori가 아닌 urease producing bacteria에 의한 false positive가 가능하다는 이야기입니다. "False-negative tests are more frequent than false-positive tests and thus a negative
result should not be used to exclude H. pylori. False-positives are rare and when present may be due to the presence of other urease containing bacteria such as Proteus mirabilis, Citrobacter freundii, Klebsiella pneumoniae, Enterobacter cloacae and Staphylococcus aureus.")
진단 Statement 4: For assessment of H. pylori gastritis, a minimum standard biopsy setting is two biopsies from the antrum (greater and lesser curvature 3 cm proximal to the pyloric region) and two biopsies from the middle of the body. Additional biopsy from the incisura is considered for detection of precancerous lesions.
: 헬리코박터 위염을 평가하려면 조직검사는 좀 더 많아야 합니다. 전정부에서 두개, 위체부에서 두개, 그리고 angle에서 하나입니다. 우리 실정에 가장 맞지 않는 statement 중 하나입니다.
진단 Statement 6: It is recommended to perform clarithromycin susceptibility testing when a standard clarithromycin-based treatment is considered as the first-line therapy, except in populations or regions with well documented low clarithromycin resistance (<15%). This test can be performed either by a standard method (antibiogram) after culture or by a molecular test directly on the gastric biopsy specimen.
: Clarithromycin-base triple therapy 전에 clarithromycin 내성 검사를 꼭 하도록 권하고 있습니다.
치료 Statement 4: In areas of high (>15%) clarithromycin resistance, bismuth quadruple or non-bismuth quadruple, concomitant (PPI, amoxicillin, clarithromycin and a nitroimidazole) therapies are recommended. In areas of high dual clarithromycin and metronidazole resistance, bismuth quadruple therapy (BQT) is the recommended first-line treatment.
: 우리나라의 경우 bismuth quadruple therapy를 초치료로 선택하라는 이야기입니다.
치료 Statement 5: The treatment duration of bismuth quadruple therapy should be extended to 14 days, unless 10 day therapies are proven effective locally.
: 게다가 2주 치료가 필요합니다.
연자는 다음과 같이 외쳤습니다. Sequential is out!!! 더 이상 sequential therapy와 같이 복잡하고 효과가 모호한 치료는 시행되지 말아야 한다는 이야기입니다.
어떤 전문가의 comment: Maastricht V 역시 서양인의 시각에서 씌여졌습니다. 일본이나 한국과 같은 동양의 사정은 충분히 반영되지 못하였습니다. 예를 들어 심한 위축성 위염이 있는 경우에 대한 고려는 없습니다. 아직 정립되지 않은 부분도 서양 의사들이 관심을 가졌다는 이유로 중요하게 다뤄진 부분이 있습니다.
![]() 9. POEM (Inoue)
9. POEM (Inoue)
Vigorous achalasia에서는 myotomy를 길게 할 필요가 있습니다. Inoue 선생님은 23 cm myotomy를 시행하였던 증례를 보여주었습니다. 수술로는 이런 긴 myotomy를 할 수 없기 때문에 긴 myotomy를 할 수 있다는 것이 내시경 치료의 장점 중 하나입니다.
Jackhammer esophagus에서도 긴 myotomy가 필요합니다. 지금까지 1000여명의 POEM 중 5증례의 Jackhammer esophagus가 있었다고 합니다. Jackhammer esophagus에서 body myotomy와 함께 LES myotomy가 필요한지는 아직 불명확합니다. Inoue 선생님은 첫 Jackhammer esophagus 환자에서 body myotomy만 했는데 3년 후 achalasia가 발생하여 다시 POEM을 했습니다. 그 이후로는 body myotomy와 LES myotomy를 함께 하고 있는데 GERD가 문제라고 합니다 .
Inoue 선생님은 two endoscopy method를 자주 사용한다고 합니다.
POET (Peroral endoscopic tumor resection): aberrant pancreas in the esophagus 치료 예를 보여주었습니다. 수개월에 한번 반복적인 증상이 생기는 환자고 식도에 pancreatic duct opening이 있었습니다. POEM과 비슷한 방법으로 치료했다고 합니다.
Inoue 선생님은 laparoscopic Heller myotomy의 적응증은 더 이상 없다고 말하면서 historical 시술이 되었다고 언급하였습니다.
Anterior myotomy의 유일한 문제는 이 부위에 big perforating artery를 가진 환자가 있다는 것입니다.
Lateral myotomy는 좋지 않습니다. 식도의 lateral 영역은 폐와 닿는 부위이므로 음압으로 인하여 POEM 후 큰 diverticulum이 발생할 수 있기 때문입니다.
* 참고: EndoTODAY 식도이완불능증과 POEM
![]() 10. Mild to moderate active Crohn's disease (Yasuo Suzuki. Toho University Sakura Medical Center)
10. Mild to moderate active Crohn's disease (Yasuo Suzuki. Toho University Sakura Medical Center)
크론병의 원인은 아직 명확하지 않지만 최근에는 enviornmental factor가 강조되고 있습니다.
상부위장관 크론은 3-5% 정도입니다.
흡연은 크론병 flare의 중요한 위험인자입니다.
![]() 11. Recent topics on small intestinal and colorectal diseases in Asia
11. Recent topics on small intestinal and colorectal diseases in Asia
1) Celiac disease in Asia (Govind K. Makharia, India)
아시아 지역에서 celiac disease의 seroprevalence는 1.6%이고, celiac diease의 prevalence는 0.5%입니다. 인도에는 상당히 흔한데 지역차는 큰 편입니다.
저는 다음과 같은 질문을 했습니다. "There is only one case of celiac disease reported in Korea. However, there seems to be a lot of cases with non-celiac gluten sensitivity. They have gluten or wheat sensitivity but no selorogic evidence of celiac disease or no IgE to gluten. Could you common on the prevalence and management of non-celiac gluten sensitivity in India?" 청중 중 한 선생님께서 non-celiac gluten sensitivity는 misnomer라고 지적해 주셨습니다. 원인이 gluten이 아니기 때문입니다. 올바른 이름은 non-celiac wheat sensitivity라고 합니다.
2) Intestinal tuberculosis (Ari Fahrial Syam, Indonesia)
장결핵은 (1) ulcerative, (2) hypertrophic, (3) ulcerohypertrophic varities로 나눌 수 있습니다.
* 참고: EndoTODAY 결핵성 위장질환
3) Giardiasis, intestinal amebiasis, irritable bowel syndrome and functional dyspepsia (Ujjala Ghoshal)
출처: CDC
Giardiasis 후 IBS가 발생할 수 있습니다. FD도 발생할 수 있습니다.
Giardiasis의 진단은 어렵습니다. 검사의 sensitivity가 낮기 때문입니다. 가장 이상적인 경우에 1회의 대변 검사는 30%, 3번의 대변 검사는 60-70%의 sensitivity를 보입니다. ELISA는 50%의 sensitivity를 보입니다. High index of suspicion이 필요합니다.
Available evidence suggest that intestinal amoebiasis is not associated with IBS.
![]() 12. Novel diagnostic and therapeutic approaches to IBD
12. Novel diagnostic and therapeutic approaches to IBD
1) Novel endoscopic technique in IBD (Rubert W Leong)
Chromoendoscopy가 dysplasia 발견율을 높힙니다.
Full spectrum endoscopy (FUSE)도 dysplasia 발견율을 높힙니다.
Target biopsy면 충분합니다 (Watanabe T. Gastroenterol 2016). Random biopsy를 추가하는 것은 도움이 되지 않았습니다.
CLE (confocal laser endoscopy)로 fluorescence leak나 cell drop out 등을 통하여 mucosal healing을 살필 수 있습니다. Leaky gut을 평가할 수 있는 일종의 functional imaging입니다.
IBS-like symptoms in mucosal healing. Leaky gut은 설사의 빈도와 연관관계가 있었습니다.
2) The role of serum and fecal biomarkers in IBD management (Ida Normiha Hilmi, Malaysia)
힐 선생님은 "I Love CRP."이라는 슬라이드를 보여주었습니다.
Serology: ASCA in CD, ANCA in UD - ASCA is positive mainly in small bowel CD, conversely pANCA is commonly positive in CD colitis.
Fecal biomarkers: calprotectin, lactoferin, S100A12, M2PK, FIT, lipocalcin 2 ...
Fecal calprotectin: pooled sensitivity and specificity is 93% and 94%, respectively. 가격이 비싸고, 검사 kit에 따라 수치가 5배 정도 다르게 나온다는 한계가 있습니다.
Mucosal healing is now the 'holy grail' of IBD treatment.
3) Combination therapy with fecal microbial transplantation (FMT) and antibiotics for ulcerative colitis (Dai Ishikawa, Juntendo University, Tokyo)
이 선생님은 UC 환자에서 FMT (fecal microbial transplantation) 이전에 항생제를 투여하는 임상연구를 발표하였습니다. 항생제 투여 후 Bacteroides가 거의 없어졌다가 FMT 후에는 회복되는 경과를 보였습니다. 임상상도 호전되었다고 합니다.
UC 환자에서 FMT alone은 도움되지 않았다고 합니다.
4) Surveillance colonoscopy for ulcerative colitis-associated neoplasia (Toshiaki Watanabe, The University of Tokyo)
UC-associated colorectal cancer (CRC)와 sporadic CRC를 비교하였을 때, Stage III에서는 UC-CRC가 sporatic CRC보다 예후가 나빴습니다. Watanabe Inflamm Bowel Dis 2011
동경대학교에서는 지난 36년간 289명을 추적했습니다 (2276 대장내시경). Dysplasia는 10년에 12.1%, invasive CRC는 10년에 3.2%였습니다. St Mark UK의 결과와 비슷했습니다 (Cho CH Am J Gastroenteorl 2015;110:1461). 즉 일본의 환자와 서양의 환자의 위험성은 비슷했습니다. 33명의 dysplasia가 발견되었습니다 (12 HGD, 21 LGD). 21명의 low grade dyplasia를 추적관찰하였을 때 2명의 암, 2명의 high grade dysplasia가 발생하였습니다.
갑자기 2015년 내시경세미나의 양동훈 선생님의 강의가 생각납니다. 사실 오늘 강의보다 훨씬 훌륭했습니다. 다시 읽어봅니다.
저는 "암감시를 위하여 panchromoendoscopy나 segmental random biopsy 둘 중 하나를 하라고 권하셨는데 실제 임상에서 둘 중 어느 것도 보질 못했습니다. Panchromoendoscopy라면 시간도 매우 많이 걸릴 것 같습니다. 가이드라인의 권고와 실제 임상 행위가 다른 것을 어떻게 이해해야 할까요?"라는 질문을 했습니다. 양동훈 선생님 강의에 답변이 있었습니다. "Chromoendoscopy prolonged the procedure time by 11 minutes in average."
염증성 장질환 환자에서의 대장암은 stepwise progression을 따르지 않는 경우가 많습니다. 갑자기 암이 되는 수가 많다는 이야기입니다.
대장염의 범위와 이환기간 이외에도 암발생 고위험 인자가 있습니다.
염증성 장질환 환자에서 발생하는 dysplasia를 구분할 때 flat이라는 용어가 부적절하여 최근에는 visible/invisible로 기술하는 방법이 제안되었습니다.
Panchromoendoscopy with target biopsy를 하면서 random biopsy를 하지 않으면 1-1.5%환자에서 dysplasia를 놓칠 것으로 추정됩니다. 그러나 이를 막기 위해서는 매우 많은 조직검사를 해야 하는데 1,000개 조직검사에서 하나 정도의 dysplasia가 발견됩니다. 결국 panchromoendoscopy가 추천되고 있습니다. 색소 대신 NBI를 권하는 가이드라인은 아직 없다고 합니다.
![]() 13. [Satellite symposium] Advanced ERCP techniques (Hiroyuki Isayama)
13. [Satellite symposium] Advanced ERCP techniques (Hiroyuki Isayama)
 SpyGlass DS와 Spybite를 이용하여 CBD cancer에 대한 mapping biopsy를 할 수 있습니다.
SpyGlass DS와 Spybite를 이용하여 CBD cancer에 대한 mapping biopsy를 할 수 있습니다.
Interventional EUS: EUS-CDS with fully-covered Wallflex
EUS-FNA Rendezvous technique: trans-duodenal route: short position (TDS)
EUS-GBD for cholecystitis (bridge to surgery)
Short double balloon endoscope
SEMS placement DBE
Combined therapy of DBE-ERCP and IV-EUS
EUS-guided antegreade removal of CBD stone
연자는 'ESD in the bile duct'가 꿈이라고 말했습니다.^^
![]() 14. [Satellite symposium] Advanced tissue resection (Michael Bourke)
14. [Satellite symposium] Advanced tissue resection (Michael Bourke)
 연자는 adenoma-carcinoma sequence가 없다고 말했지만... 사실 adenoma-carcinoma sequence를 따르는 위암이 매우 많습니다. (참고: EndoTODAY 선종)
연자는 adenoma-carcinoma sequence가 없다고 말했지만... 사실 adenoma-carcinoma sequence를 따르는 위암이 매우 많습니다. (참고: EndoTODAY 선종)
호주에서도 ESD는 cost effectiveness 측면에 잇점이 있습니다.
EMR 후 snare tip으로 marginal ablation을 하였을 때 재발률이 줄어든다는 흥미로운 자료입니다. APC를 이용하여 ablation하는 것보다 조금 더 간단한 방법인데... 과연 효과가 있을지 의문이었습니다. APC로 ablation을 할 때 연자는 40 joule을 사용하였는데 정훈용 교수님께서는 60 joule을 써야 할 것이라고 comment 하셨습니다. Stomach은 80 joule이라고 합니다.
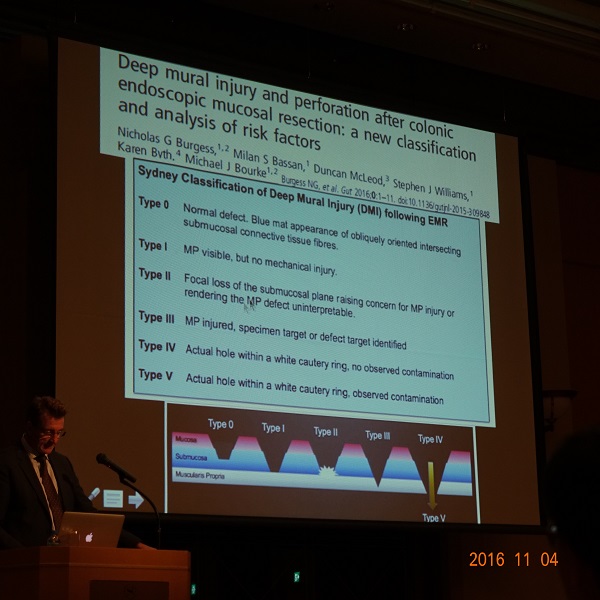 Classification of submucosal injury (Burgess NG. Gut 2016)
Classification of submucosal injury (Burgess NG. Gut 2016)
![]() 15. [2016-11-5. 8:30am] Gastric cancer prevention guideline consensus symposium : Asia-Pacific consensus guideline on gastric cancer prevention 2016
15. [2016-11-5. 8:30am] Gastric cancer prevention guideline consensus symposium : Asia-Pacific consensus guideline on gastric cancer prevention 2016
1) Asia-Pacific consensus on prevention and treatment of gastric cancer (Kaichun Wu, China)
위암 예방에 대한 key note lecture였습니다. 온통 Helicobacter 제균치료 이야기였습니다. (위암 예방을 위한 Helicobacter 제균치료가 불법인 대한민국 의사로서는 할 말이 없었습니다.)
Clinical question: What is the available method of secondary prevention of gastric cancer? Statement: Endoscopy is the optimal test for gastric cancer.
- 내시경 이외에 방사선 방법이나 혈액 검사는 기각되었다는 이야기입니다.Clinical question: What are factors to assist in risk stratification before endoscopy. Statement: Low serum pepsinogen 1 or low PG1/PG2 ratio in the settin gof positive HP infection... Serum MG7-Ag is a potential new marker for gastric cancer.
- 연자는 내시경 전에 pepsinogen 검사를 하는 것이 어떤가 언급하였고, 심지어 결론에서 "Endoscopy (screening, survaillance and resection) plus biomarkers is the best option for secondary preventionof gastric cancer."라고 말했습니다만, 현재 우리나라에서는 불필요한 일입니다. 내시경을 할 것이면 다른 검사는 필요하지 않을 것이기 때문입니다. 내시경 quality를 높이는 것이 더 좋을 것 같습니다.
중국에서 위암의 5년 생존율은 아직 25-30% 수준입니다. 조기위암이 25%에 미치지 못하기 때문입니다.
중국은 큰 나라입니다. 지역에 따른 Helicobacter 감염률 차이가 상당했습니다.
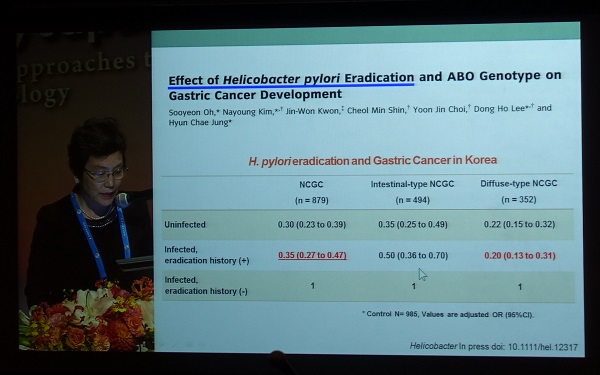
2) Gastric cancer prevention in Korea (서울대학교 김나영)
강의 서두에 "Primary prevention of gastric cancer in Korea: no guideline has been published yet."라는 슬라이드를 보여주셨습니다. 안타깝습니다. 저는 이렇게 외치고 싶었습니다. /헬/리/코/박/터/제/균/치/료/를/허/가/하/라/
위암 예방에 대한 새로운 자료를 보여주셨습니다.
Sugano 좌장께서는 secondary prevention을 위한 medical resource를 어떻게 관리하는가 질문하였습니다. 연자께서는 내시경을 내과 의사 뿐만 아니라 다른 과 의사들도 하고 있으므로 resource는 많은 편이라고 답하셨고, 한국 내시경 의사의 quality도 상당히 좋은 편이라고 덧붙이셨습니다.
Floor에서 El-Omar라는 유명한 서양 의사가 '왜 한국 정부는 위암 예방을 위한 제균치료를 허락하지 않는가?' 라고 질문하였습니다. 연자 답변: "초기에 beneficial effect에 대한 근거가 부족하다는 점에서 hesitation이 있었다. Government is very rigid. 정부에 대한 좀 더 적극적인 설득이 필요한데, international consensus guideline이 very helpful할 것이다."
Floor에서 '한국은 내시경이 싸기 때문에 secondary prevention이 가능할지 모르지만, 다른 나라에서는 내시경이 비싸기 때문에 secondary prevention은 cost-effective한 option이 아니다'라는 comment가 있었습니다.
어려운 여건에서도 꾸준한 연구로 우리나라의 체면을 세우고 계시는 김나영 교수님을 존경합니다.
3) Gastric cancer prevention trials in Taiwan (Yi-Chia Lee)
대만에서도 정부를 설득하는 것이 쉽지 않은 모양입니다. Pilot 연구가 필요하고 cost effectiveness 자료가 필요하다는 점이 여러번 강조되었습니다.
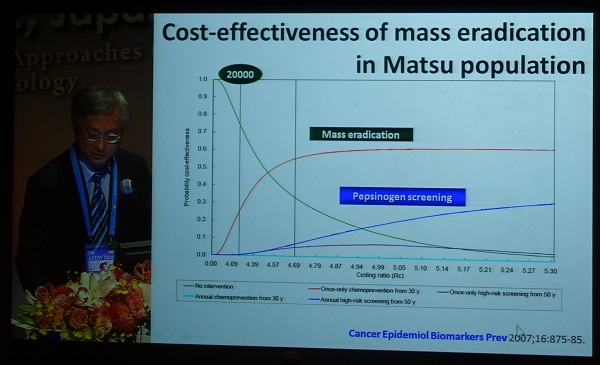
대만에서는 대장암이 가장 많고 가장 빨리 증가하고 있는 암이고, 위암은 6번째입니다. 따라서 정부에서는 대장암에 대한 관심이 더 많다고 합니다. 연자가 메타분석(Lee YC. Gastroenterology 2016;150:1113)을 시행한 가장 큰 이유가 '정부 설득'이었다고 말하였습니다.
대만에서는 정부 정책을 세우기 앞서 일정 지역을 선정하여 pilot 연구를 한다고 합니다. 위암뿐만 아니라 대장암에 대한 연구를 위한 지역이 선정되었습니다. 그리고 pilot 연구에 앞서 표준화를 위한 교육과 대국민 홍보사업을 열심히 한 모양입니다. 중국에서 최고 elite 들이 망명(?)하여 세운 elite 국가다운 모습이 아닐 수 없습니다. 자본주의 입장에서 바라보면 대만의 의료 수준은 생각보다 별로입니다. 그러나 접근 방법은 상당히 reasonable 합니다. 사회주의 냄새가 살짝 느껴집니다.

Hp 제균치료를 하더라도 모든 위암이 없어지는 것은 아닙니다. 이미 작은 암을 가지고 있거나 위축성 화생성 위염이 심한 사람이 있기 때문입니다. 따라서 제균치료 후에도 risk stratification이 중요합니다. 제균치료 후 발견된 위암 7예의 사진을 보여주셨습니다. Pepsinogen 방법이 충분하지 않아 보입니다.
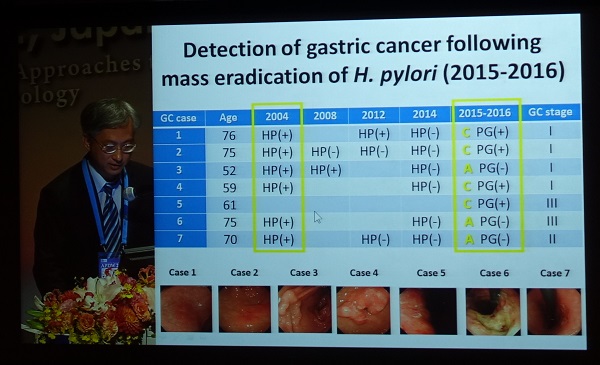
일본에서 Hp 제균치료 후 epigenetic marker를 이용한 risk stratification에 대한 발표가 있었는데 (Asada K. Gut 2015;64:388), 타이완에서도 관심이 있다고 합니다.
4) Prevention of gastric cancer in Japan (Kentaro Sugano)
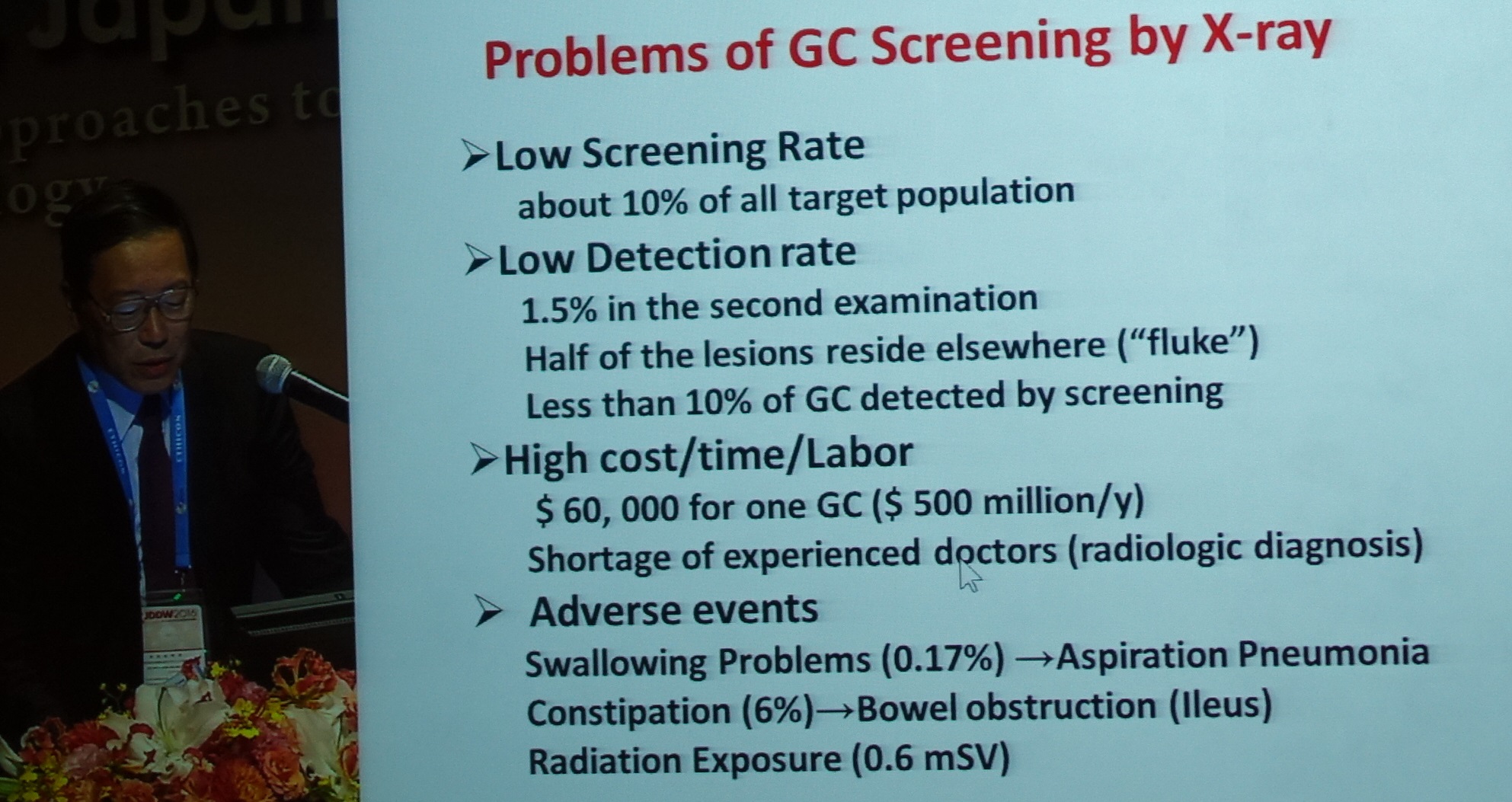
일본에서 screening program (double contrast barium study) 참여율이 2013년의 경우 남자 45%, 여자 35%로 아직 낮은 편이라고 합니다. Double contrast barium study로 검진한 사람의 8%가 내시경을 받게 되고 0.1%가 암으로 진단됩니다. 문제는 무증상 위암 중 정부 screening으로 전체 암의 10%에 불과하다는 점입니다. Private clinic의 역할이 아주 중요합니다.
일본 위암 검진 가이드라인 (2014): 50세에 시작하여 2년에 한번 내시경
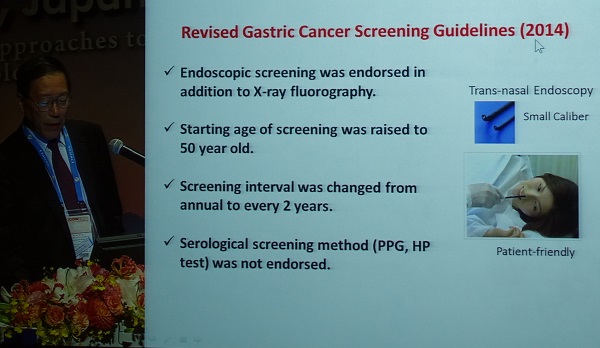
일본 중앙 정부에서는 serological screening을 인정하지 않았습니다. 그러나 일부 지방 정부에서는 serological screening을 인정한 곳도 있다고 합니다.
Asaks 선생님과 Sugano 선생님들이 정부에 지속적으로 Hp gastritis에 대한 제균치료를 요청하였더니, 일본 정부에서는 "Don't bother me any more."라고 말하면서 허락을 해 주었다고 합니다. (데이타가 충분한 것은 아니지만 강하게 push하여 정책 변화를 이끌었다는 고백 같습니다.)
* 참고: 일본검진내시경 개정안 (일본어)
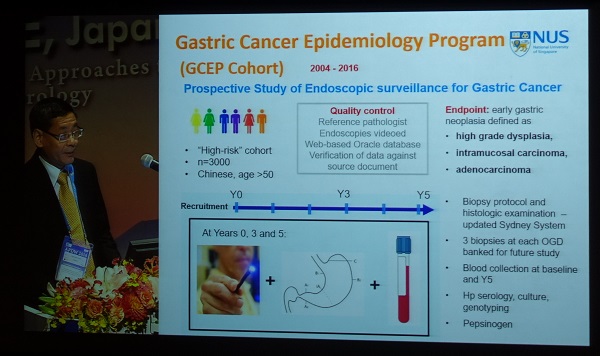
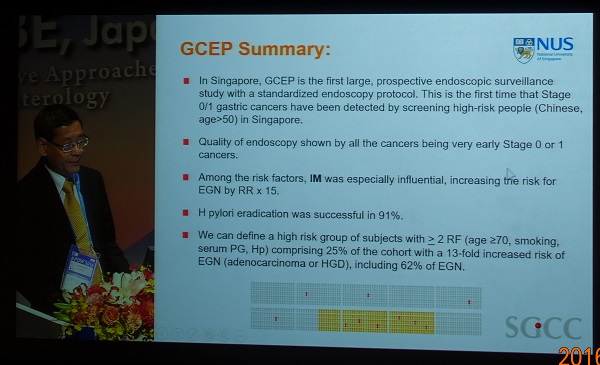
5) Gastric cancer prevention in Singapore (Khay-Guan Yeoh)
2004년부터 Chinese를 대상으로 screening 연구가 진행되고 있다고 합니다. 말레이 출신은 위암 발생률이 낮으므로 Chinese가 대상이었다고 합니다.
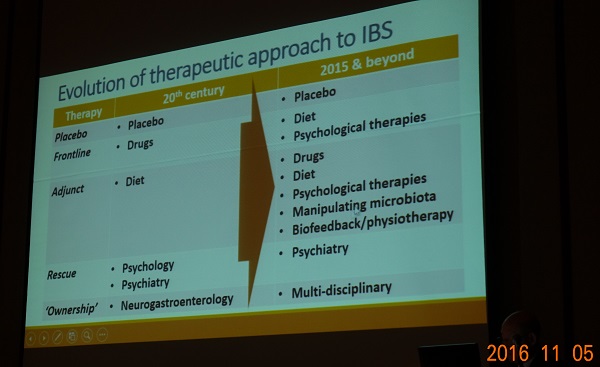
![]() 16. [2016-11-5. 10:20am] Recent advances in irritable bowel syndrome (Peter Gibson)
16. [2016-11-5. 10:20am] Recent advances in irritable bowel syndrome (Peter Gibson)
연자가 젊은 소화기 의사일 때에는 할 수 있는 것이 거의 없어서 very depressing 했다고 합니다. 그러나 최근에는 많은 접근법이 가능합니다.
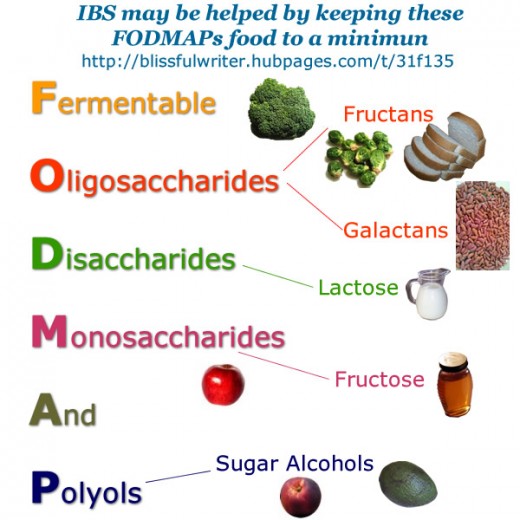
Dietary approaches: gluten free diet와 low FODMAP diet가 핵심입니다. Low FODMAP diet can be highly effective, but requires skills more than just giving the patient a diet sheet.
Low FODMAP diet는 왜 성공적이었는가? (1) luminal distension이 줄어듭니다. (2) 음식에 대한 자료가 축적되고 있습니다. (3) 좋은 교육 방법이 확립되어 있습니다. (4) 연구가 많습니다. (5) App을 통하여 정보가 유통되고 있습니다.
Low FODMAP diet를 하면 대변의 균 종류가 달라집니다. 연자는 이런 질문을 던졌습니다. 이런 변화가 dysbiosis일까요, prebiosys일까요?
Dietary and psychological intervention이 first-line therapy가 되어야 한다는 take-home message로 강의가 끝났습니다. 약에 대한 이야기보다는 음식과 stress 관리에 대한 이야기가 많아서 만족스러운 시간이었습니다. IBS는 약으로 치료할 병이 아닌 것 같습니다.
Food allergy에 대한 질문이 있었습니다. 아직 명확히 확립되지 않은 것 같습니다. 음식에 대한 IgG 항체를 측정하고 이를 바탕으로 음식을 조절하는 접근은 효과가 없고, allergy 학자들은 그런 접근은 하지 말라고 권한다고 합니다.
* 참고: EndoTODAY Celiac disease and gluten sensitivity
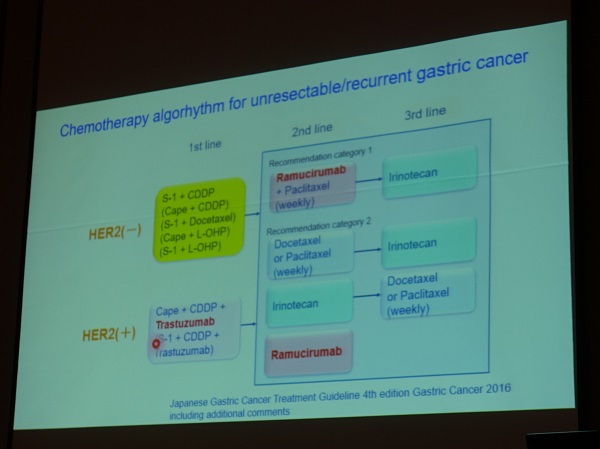
![]() 17. [Luncheon symposium] Gastirc cancer treatment strategy
17. [Luncheon symposium] Gastirc cancer treatment strategy
Prophylatic paraaortic lymph node dissection is not required for all patients.
근위부 위암이 greater curvature를 direct하게 invasion하지 않는 한 splenectomy는 권유하지 않습니다.
Stage II-III에서 Surgery alone 보다 S-1 adjuvant 치료를 하였을 때 생존율이 높아졌습니다 (Sasako. JCO 2011;29:4287). Stage II, IIIa, IIIb에서 lymph node metastasis와 stage II에서 peritoneal metastasis는 줄였지만 hematogenous metastasis는 뚜렷하게 줄이지 못했습니다. S-1은 lymph vessel 내의 암세포에는 작용하지만 lymph node 내의 암세포에서는 작용하지 않는 것 같다고 언급하였습니다. S-1에 의하여 죽지 않은 lymph node 내의 암세포가 커지고 터져서 peritoneal seeding이 된다고 설명하였습니다.
Postoperative body weight loss and S-1 compliance. 체중이 15% 이하 감소한 경우 compliance가 66%인 반면, 체중이 15% 이상 감소한 경우는 36%였습니다.
수술 전후 elementay diet supplement가 수술 후 체중 감소를 줄였습니다.
신체적 performance에 따라 fit, vulnerable, frail로 나눌 때, elderly patient에서는 fit은 감소하고 vulnerable과 frail은 증가합니다.
![]() [FAQ]
[FAQ]
[2016-11-3. 애독자 편지]
이준행 교수님. APDW 2016 하이라이트 잘 보았습니다.
언제나 감탄스러운 점이 같은 강의를 들으면서도 어떻게 이렇게 잘 요약 정리하고, 영상도 챙겨서 정리가 가능하실까 하는 점입니다. 저도 학회에 참석에서 강의들을 때 주의깊게 들으려면 메모를 하기도 하지만, 메모하다 보면, 연자의 다음 설명을 놓치고, 사진을 찍으려면 슬라이드가 벌써 넘어가 있는 등 쉽지 않았습니다. Multi-tasking에 관한 개인적인 역량 차이인가? 하고 자조하기도 하지만, 계속 노력 중입니다.
이 교수님이 강조하신 연속성 있는 컨퍼런스 진행, 전공의/전임의 교육 등의 기치에 공감하여 저도 저희 병원에서 부족하지만 교육적인 부분을 보완하고자 노력 중입니다. 출중한 의사는 남이 가르쳐 주지 않아도 알아서 찾아 공부하지만, 대부분의 의사는(저를 포함해서) 초심자 시절 무엇을 어떻게 접근하고 알아봐야할지 몰라 쩔쩔 맬 때 주위의 뛰어난 선생님들의 모습을 롤 모델로 삼는 것이 도움이 되었던 것 같습니다. 미력하지만, 교육에 정진하여 훌륭한 후배 의사 선생님들이 배출될 수 있도록 노력하겠습니다.
아침에 이 교수님 메일 보고, 감사의 말씀 드려야 할 것 같다는 생각이 들어 적어 보았습니다. 학회 잘 다녀오십시오. 감사합니다.
부산에서 XXX 드림
[2016-11-4. 이준행 답장]
좋은 말씀 감사합니다.
EndoTODAY에 학회 기록을 남기는 것은 여러분의 교육을 위한 것도 있지만 제 자신의 기억을 돕기 위한 것이기도 합니다.
사실 저는 multitasking에 능한 편이 아닙니다. 오히려 한번에 한 가지 일만 잘하자는 생각을 가지고 있습니다. 그리고 컴퓨터 박사도 아닙니다. 옛날 방식으로 홈페이지 만들기를 18년째 계속하고 있을 뿐입니다. 새로운 기술을 배우기보다는 한번 익힌 기술을 아주 오래, 아주 잘 할 때까지 두고두고 사용하고 있을 뿐입니다. 매일 적어도 1시간 이상 홈페이지 update에 시간을 보냅니다. 공부를 겸하여... 그래서 조금 빨라졌습니다. 개인적인 역량 차이가 아닙니다. 선생님도 잘 하는 것을 찾아서 아주 오래, 아주 아주 오래, 남들이 깜짝 놀랄 만큼 오래 하면 잘하게 됩니다.
EndoTODAY를 성원해 주셔서 감사합니다.
고베에서 이준행 드림
[2016-11-4. 애독자 편지]
방금 보내주신 글 잘 읽었습니다. 서양인들이 만든 위염, 위암, 내시경 가이드라인은 우리 현실과 너무 동떨어져서 이번 개정판도 진료에 반영하기 어려울 것 같습니다. 개정판에 대해서 조목조목 따질 수 있는 과학적인 근거들을 마련하는 발판을 다음 한일 헬리코박터학회에서 만들 수 있으면 좋겠습니다.
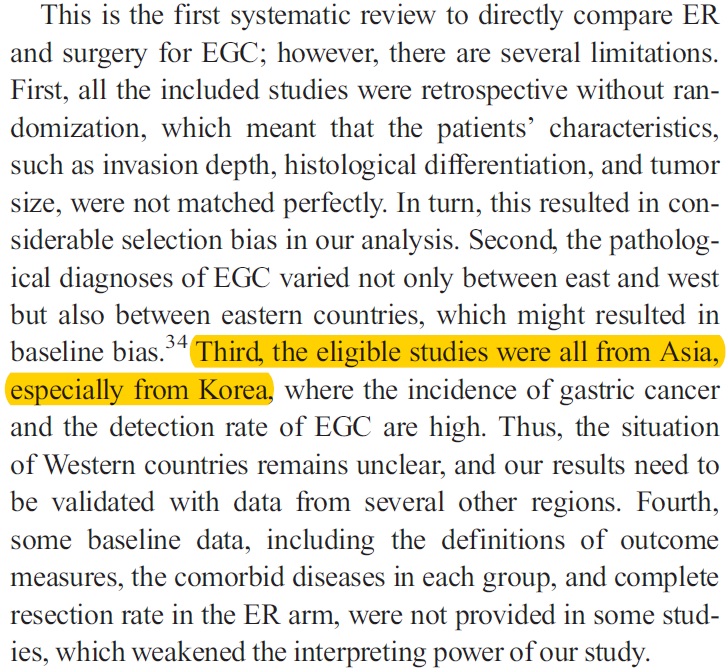
답답해하는 동양의사들이 생각보다 많은 것 같습니다. 오래 전에 처음 보는 중국의사가 "믿을 만한 위암 논문은 한국 데이터 밖에 없다"는 말을 해서 기특하다고 생각한 적이 있었는데, 그 내용이 논문으로 게재되었습니다 (Sun K. Digest Endosc 2016). 고찰 마지막 부분 중 일부입니다.
Second, the pathological diagnoses of EGC varied not only between east and west but also between eastern countries, which might resulted in baseline bias. Third, the eligible studies were all from Asia, especially from Korea, where the incidence of gastric cancer and the detection rate of EGC are high. Thus, the situation of Western countries remains unclear, and our results need to be validated with data from several other regions.
[2016-11-5. 이준행 답변]
좋은 point입니다.
서양 사람은 서양 방식으로 생각하고 서양 방식으로 연구하고 서양 방식으로 살아갑니다. 일본 사람은 일본 방식으로 생각하고 일본 방식으로 연구하고 일본 방식으로 살아갑니다. 우리는 우리 방식으로 생각하고 우리 방식으로 연구하고 우리 방식으로 살아가는 것이 자연스럽습니다. 우리의 문제는 우리가 해결해야 합니다. 우리 생각대로...
지적하신 바처럼, 서양 사람들이 쓴 글이 무슨 진리라도 되는 것처럼 추종할 이유는 없을 것 같습니다. 이번에 발표된 Maastricht V는 그야말로 그네들 생각입니다. 우리에게는 득보다 실이 많을 것 같습니다. 저는 살짝 무시하려고 합니다. 모르는 척^^
중국인이 우리나라 논문을 높게 평가하는 것은 그들의 문제와 우리의 문제가 겹치기 때문이겠지요. 그들의 사고방식과 우리의 사고방식이 겹치는 측면도 있구요. 우리의 논문이 다른 나라 논문보다 좀 더 솔직하기 때문이기도 할 것입니다. 저는 우리의 문제를 있는 그대로 드러내고, 그 속에서 해법을 찾아가는 논문을 좋아합니다.
![]() [고베 산책]
[고베 산책]
일본의 큰 도시에는 어디나 이런 풍경이 있습니다.
숙소 근처 한 공원에서 국민학교 학생들 축구경기가 열렸습니다. 엄마, 아빠들이 많이 와 있었습니다.
石屋川 (이시야카와) 역. 사케도 만들고 음식도 파는 식당 酒心館 (Syushinkan)에 가는 길.
酒心館
![]() [References]
[References]
1) 일본 학회
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.


{kind=link}