EndoTODAY 내시경 교실
EndoTODAY 내시경 교실
Beginner | ESA | Schedule | OPD
Seminars | Atlas | Recent | Links
![]() [위암학회 KINGCA 2017]
[위암학회 KINGCA 2017]
일시: 2017년 3월 23일 (목)- 3월 25 (토)
장소: 부산 Bexco


2017-3-24. Gala dinner
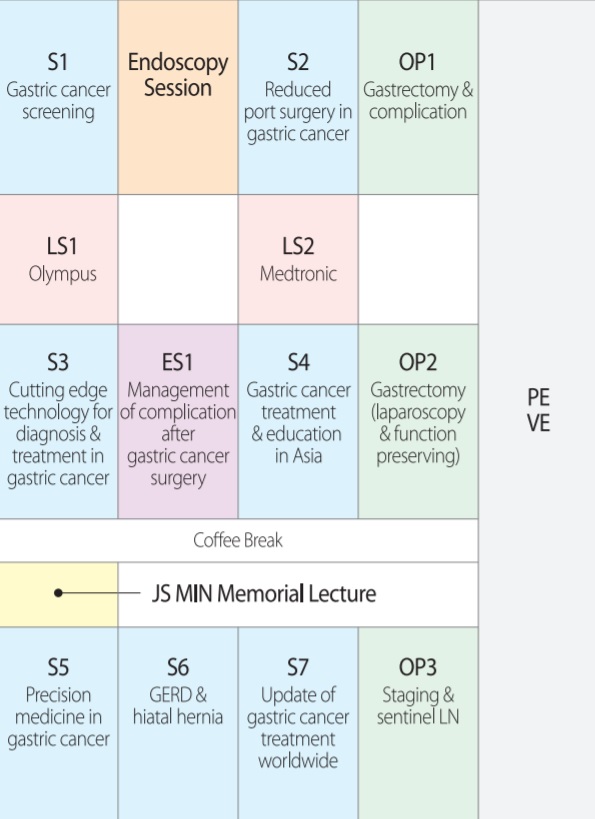
저의 발표와 같은 시간에 room B에서는 Endoscopy session이 열렸습니다. 제목을 소개합니다.
1) Introduction: Korean perspective of upper endoscopy for surgeon (가톨릭대학교 송교영)
2) How to start endoscopy and what we need to do safe procedure (울산대학교 정훈용)
3) Usefulness of surgeon's endoscopy in perioperative evaluation for gastric cancer (경상대학교 박지호)
4) Development and training of endoscopy for surgeons in Hong Kong (Philip Chiu, Hong Kong)
강의를 듣지 못한 것이 너무 아쉬워 정훈용 교수님께 따로 문의하였습니다. 아산병원에서는 초심자를 위하여 3 개월 정도의 introductory course를 운영하고 계신다고 합니다. 제가 운영하고 있는 3개월 코스(아래 table)와 비슷한 것 같습니다. 특이한 것은 (1) image training을 위하여 내시경 검사 과정을 상세히 기술한 문서를 만들고 이를 암기하도록 한다는 점과 (2) 이진혁 교수님께서 개발하신 3-D model을 이용하여 내시경 삽입법 연습을 한다는 점이었습니다. 내시경을 잡기 전 상당 기간 intensive한 교육을 받아야 한다는 점은 인상적이었습니다. 그렇습니다. 시대가 바뀌었습니다. 충분한 교육 없이 내시경을 시작하는 일은 없어야 할 것 같습니다.
SMC basic endoscopy training course (3 months) Program 1st month 2nd month 3rd month On-line lecture 
KSGE lectures 1-10 KSGE lectures 11-20 Staff lecture (1) Insertion
(2) Description
(3) Common GI disordersOne point lesson One point lesson Book & Journal club Textbook reading with tutors Review the review Review the review Description training 1, 2, 3, 4 5, 6, 7, 8 9, 10, 11, 12 Gastric cancers 1,000 Season 1 Season 2 Season 3 Weekly conference Endoscopy conference
GI conferenceEndoscopy conference
GI conferenceEndoscopy conference
GI conferenceObservation and hands-on Weekly observation
Simulator trainingDaily observation Hands-on Others EndoTODAY
Topic presentation 1, 2, 3EndoTODAY
Topic presentation 4, 5, 6EndoTODAY
Topic presentation 7, 8, 9
Quiz 365
![]() 1. [목요일 11:00-12:30, Room A] Gastric cancer screening. Chair: Chisato Hamashima (National Cancer Center, Japan, chamashi@ncc.go.jp), Yong Chan Lee (Yonsei University, Korea, leeyc@yuhs.ac)
1. [목요일 11:00-12:30, Room A] Gastric cancer screening. Chair: Chisato Hamashima (National Cancer Center, Japan, chamashi@ncc.go.jp), Yong Chan Lee (Yonsei University, Korea, leeyc@yuhs.ac)
1) Outcome of National Cancer Screening Program with emphasis on gastric cancer. Il Ju Choi (국립암센터 최일주)
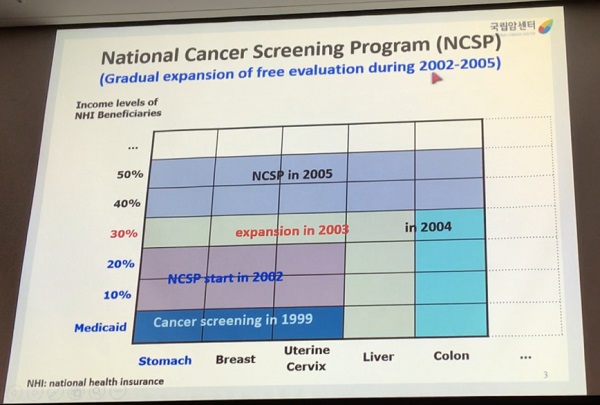
국가암검진프로그램 초기 환자를 대상으로 한 장기 연구입니다. 내시경 검사를 받으면 위암으로 사망할 확률이 절반으로 줄어듭니다. 최근에는 조금 더 좋은 결과를 보일 것으로 예측하고 있습니다. 고령에서는 위암 검진의 효과가 급격히 떨어짐을 보여주고 있습니다.
UGI series는 암사망률 감소 효과가 형편없었습니다.

국립암센터에서는 모든 위암의 30% 정도가 내시경으로 치료되고 있습니다. 국내 대형병원은 거의 비슷한 수준입니다.
2) Management of incidentally found gastric adenoma/dyslasia. Jun Haeng Lee (성균관의대 이준행)
Abstract
There are no generally accepted definitions of dysplasia and adenoma of the stomach. Dysplasia is best defined as an unequivocal neoplastic epithelial alteration. Detailed histological findings of gastric dysplasias have been described in many literatures. However, endoscopic or gross findings of gastric dysplasia need to be studied in more detail. Macroscopically, two types of dysplasias are recognized: elevated dysplasia and flat/depressed dysplasia.
Definition for adenoma is somewhat confusing. In the western countries, adenomas mean elevated or nodular lesions with dysplasia in histology, so only elevated type of dysplasias are considered as adenomas. In the eastern countries, however, both elevated and flat/depressed types of dysplasia are considered as adenomas. Actually, the terms dysplasia and adenoma are thought to be the same thing in the clinical practice. The difference is who prefers what. Usually, pathologists prefer dysplasia, and endoscopists prefer adenoma.
Dysplasias are graded as either high grade or low grade. So, adenomas (= dysplasias) can be divided as adenoma with low grade dysplasia (LGD) and adenoma with high grade dysplasia (HGD). In Korean pathologists' tradition, adenoma usually means adenoma with LGD.
In Korea, gastric adenomas with HGD are usually treated by endoscopic resection. In the final pathology for the resected specimen, 1/3 to 1/2 of adenomas with HGD are upgraded as cancer. Therapeutic approach for adenomas with HGD should be the same for early gastric cancers within absolute indications for endoscopic submucosal dissection (ESD).
Situations for gastric adenomas with LGD are quite different. After endoscopic resection of adenoma with LGD, the risk of histological upgrading is relatively small. About 10-20% of adenomas with LGD are upgraded to adenoma with HGD and 5-10% are upgraded to early gastric cancers. So, the clinical options for adenomas with LGD can be resection (EMR or ESD), ablation, and observation. In the lecture, some data regarding the advantages and disadvantages of each treatment options will be discussed.
Sano 선생님 comment: 일본의 group classification이 upgrade되었고 group 2가 중요합니다.
3) Issues and future directions of Korean gastric cancer screening guideline. 정일권 (Department of Internal Medicine, College of Medicine, The Catholic University of Korea, Seoul, Korea)
2008년에 암검진 quality control 지침이 발표되었습니다.
2014년의 경우 organized screening이 78.5%, opportunistic screening이 21.5%였습니다.
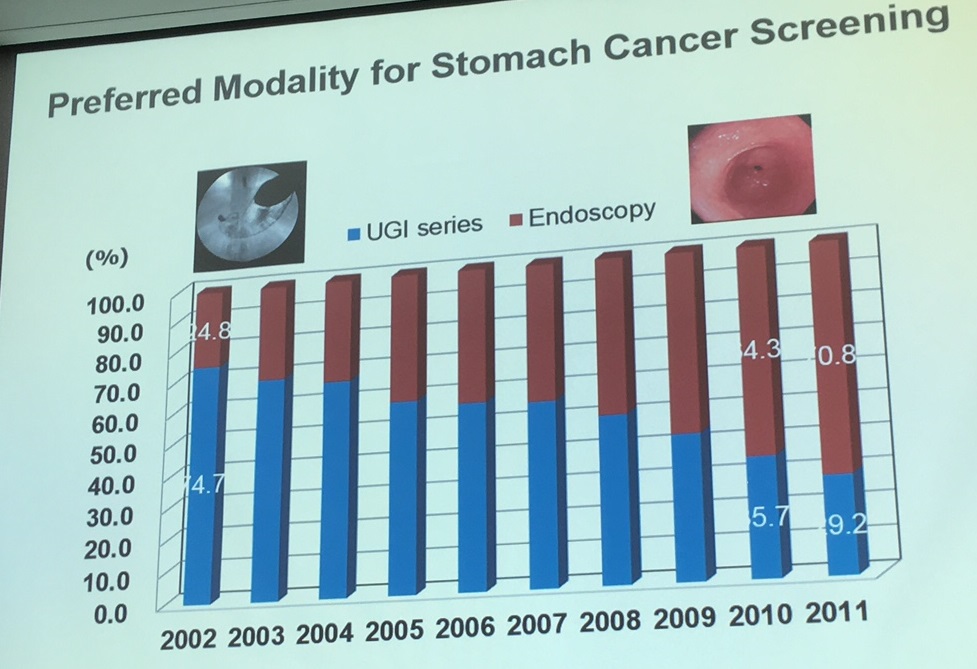
4) Japanese experience of gastric cancer screening. Chisato Hamashima (Division of Cancer Screening Assessment and Management, National Cancer Center, Tokyo)
일본에서 내시경을 사용한 위암 검진이 승인되었으나 '내시경 의사가 부족'하여 널리 보급되지 못하고 있다고 합니다.
Pepsinogen이나 Helicobacter를 이용한 검진은 인정되지 않고 있습니다.
일본에서는 내시경 검사에 73.6분이 걸린다고 계산하고 있습니다. 준비와 설명을 포함한 시간입니다.
건강검진 내시경 검사 관련하여 사망한 환자가 있다는 소중한 자료입니다.
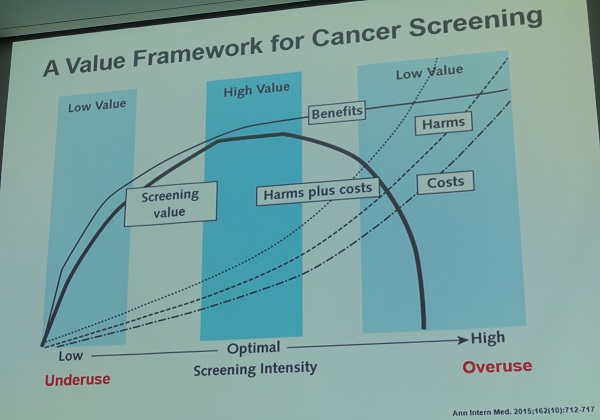
Overdiagnosis는 매우 심각한 문제입니다. 연자는 이 부분에 대하여 상세히 설명을 해 주셨습니다.
유방암의 경우는 overdiagnosis와 screening의 필요에 대한 의문이 계속 제기되고 있습니다.
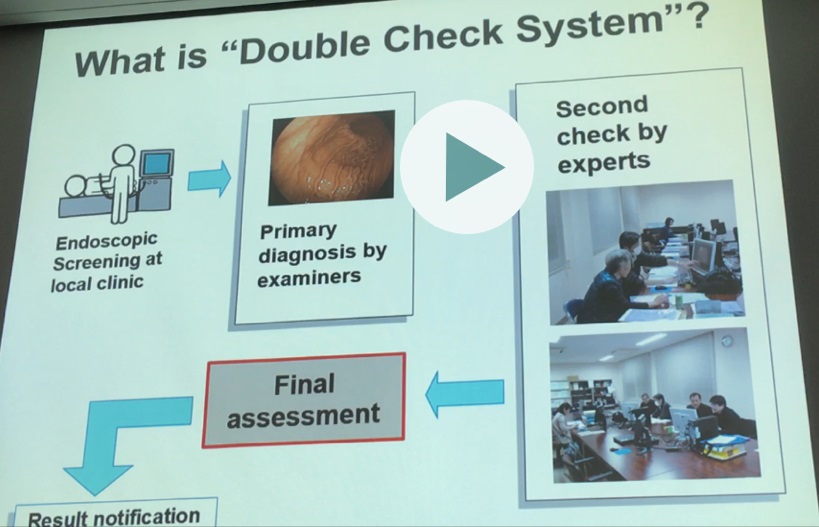
내시경 결과를 바로 제출하지 않고 독립적인 interpretation meeting을 통하여 전문가들의 double check 후 결과를 내는 quality control system을 가지고 있습니다.
일본의 recommendation입니다. 꼭 한 번 읽어보세요.
![]() 2. [목요일 13:30-15:00, Room A] Cutting edge technology for diagnosis and treatment
2. [목요일 13:30-15:00, Room A] Cutting edge technology for diagnosis and treatment
1) Role of MRI - 김세형
Diffusion-weighted image: 종양은 DWI에서 밝게 보이므로 sensitivity가 높다.
Perfusion MR imaging:
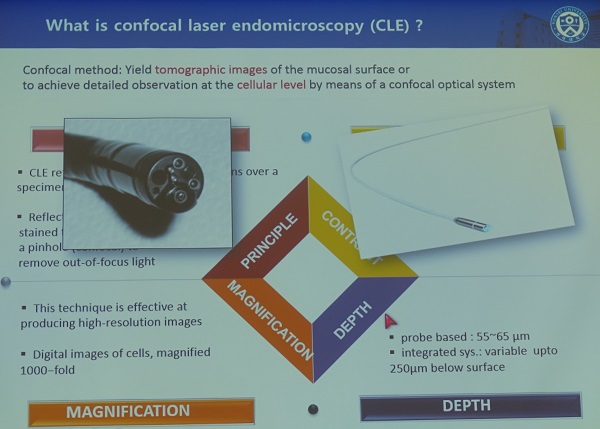
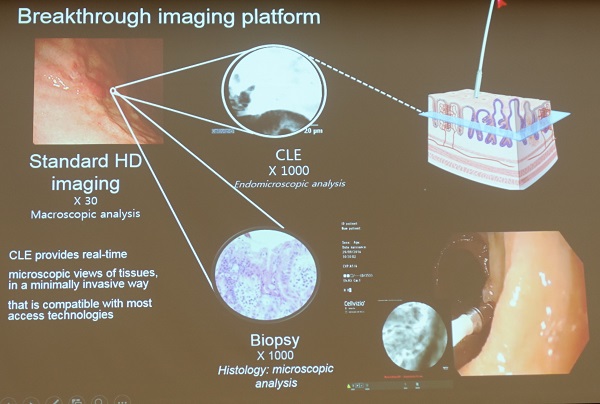
2) Confocal endoscopy - 박준철
3) Near-infrared guided gastric cancer surgery - 공성호 (서울대학교)
![]() 3. [금요일 breakfast session] What to do with the large hiatal hernia - Lars Lundell
3. [금요일 breakfast session] What to do with the large hiatal hernia - Lars Lundell
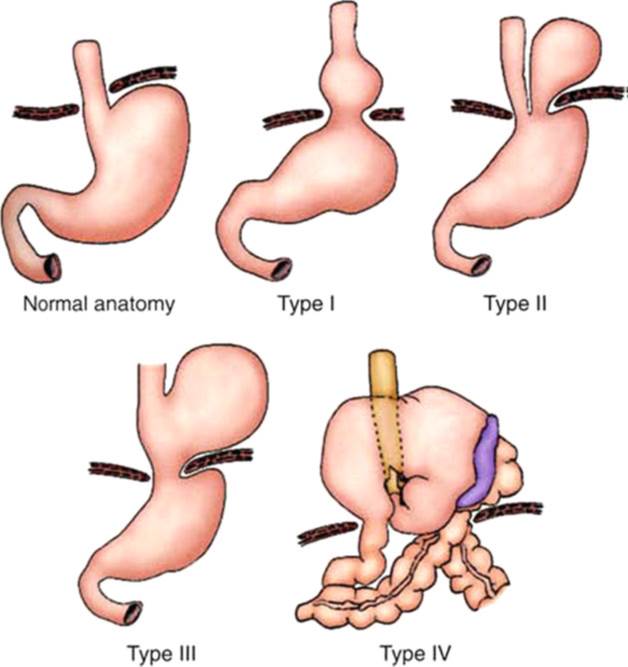
서양은 hiatal hernia와 관련된 short esophagus가 흔한데 동양에서 short esophagus가 자주 언급되지 않는 것 같습니다. 미국에서는 large hiatal hernia, short esophagus가 큰 문제라고 합니다. 특히 strangulation을 보이는 hiatal hernia가 늘고 있다는 것은 큰 문제입니다.
Lundell 교수는 위가 흉강으로 50% 이상 올라간 것을 type 4 hiatal hernia로 불렀습니다. 50% 정도 혹은 그 이하로 올라간 경우는 type 3로 분류하고 있었습니다.
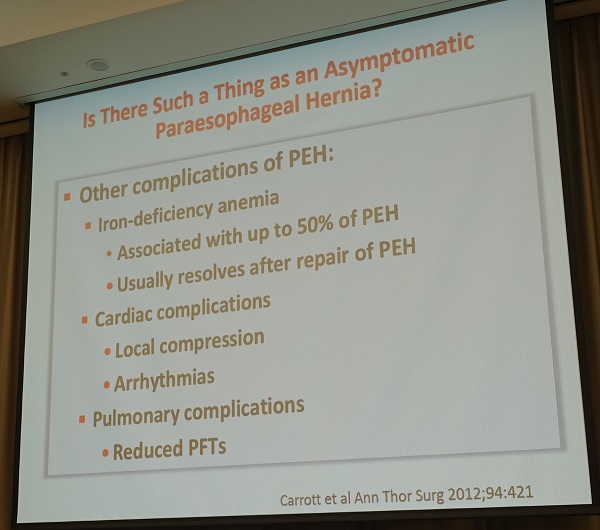
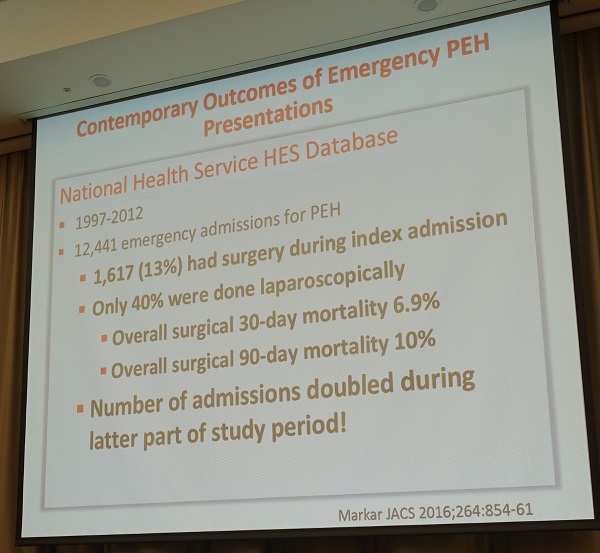
Hiatal hernia로 인한 문제는 빙산의 일각처럼 아직 다 드러나지 않았습니다. Giant hiatal hernia에 대한 응급수술은 사망률이 높습니다.
Giant hiatal hernia는 대부분 symptomatic 합니다. Asymptomatic 한 경우는 있더라도 매우 드물기 때문에 증상을 자세히 평가해야 합니다. 문제는 수술을 할 것인가 혹은 careful observation을 할 것인가의 문제입니다.
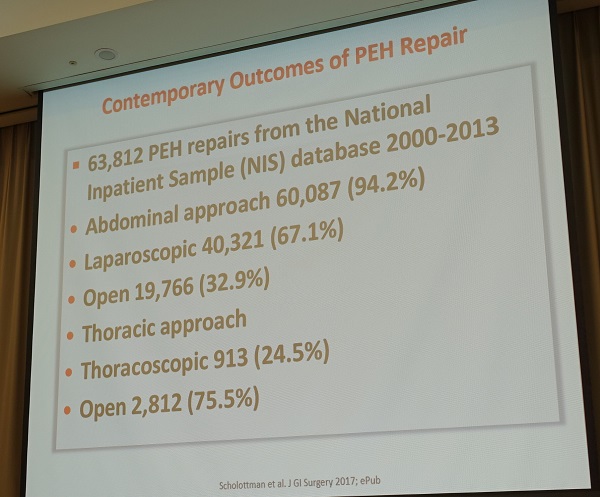
서양에서 hiatal hernia 수술은 대부분 laparoscopic으로 시행한다고 합니다. Thoracoscopic 으로 수술하는 경우는 거의 없는 모양입니다.
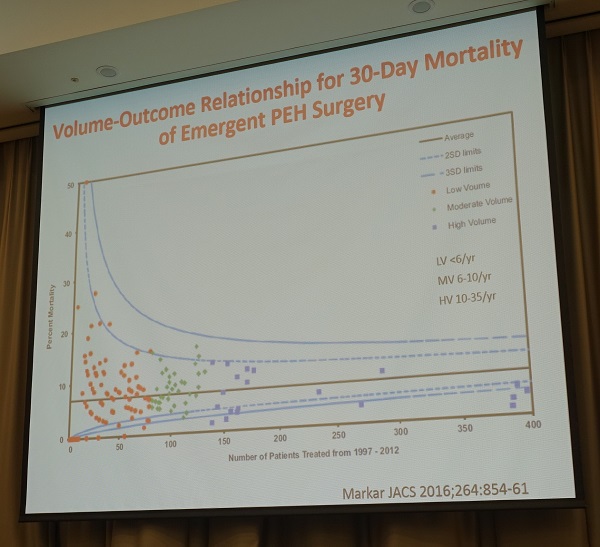
Lundell 교수는 emergent paraesophageal hernia surgery (PEH)의 mortality가 높다는 점에 대하여 오랜 시간 discussion 하였습니다.
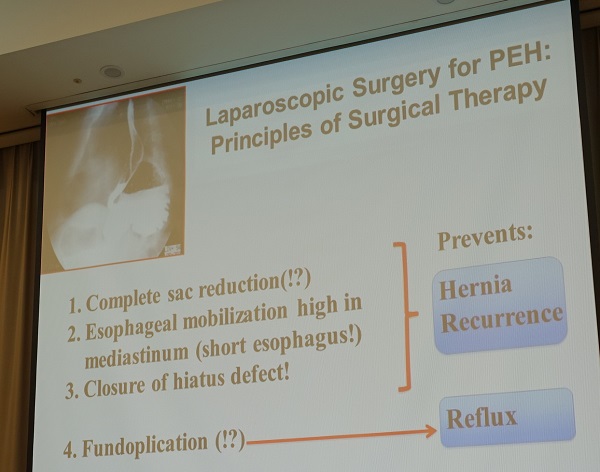
Paraesophageal hernia 수술에서 funduplication이 필요한가? reflux syndrome score로 보면 기술적 논의로 mesh를 사용할 것인가에 대하여 토론이 있었습니다. Mesh를 사용할 때 심각한 합병증이 발생한 경우가 있다고 합니다. 높은 재발률도 중요한 이슈입니다.
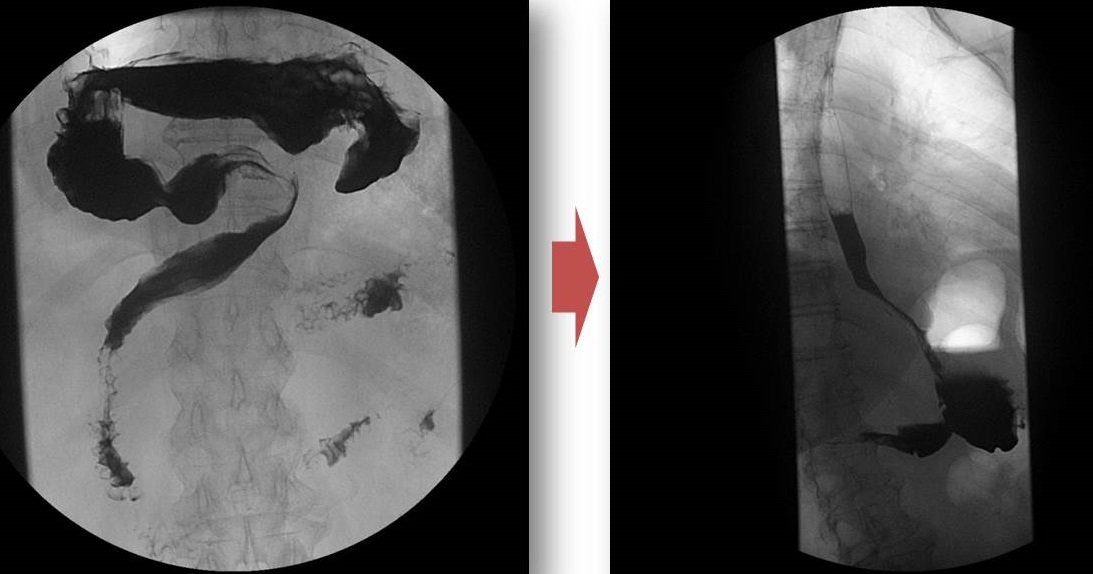
강의를 듣다 보니 recurrent bleeding으로 내원하셨던 large hiatal hernia 환자가 떠올랐습니다. Hiatal hernia가 심하고 Cameron ulcer로 인한 출혈이 발생한 경우였습니다. 수술적 치료를 권했으나 환자가 약물치료를 원하여 상당 기간 PPI를 사용하였습니다. 그럼에도 불구하고 출혈이 반복되었습니다. 처음에는 심한 sliding hernia 상태였으나 시간이 지나고 구토, 복통, 출혈로 환자가 수술을 결심하게 될 무렵에는 위 전부가 횡격막 위로 올라온 type 4 hiatal hernia가 된 상태였습니다.
심한 sliding hiatal hernia with Cameron ulcer bleeding 상태
수술하기 직전. 위 전체가 횡경막 상방으로 이동된 type 4 hiatal hernia 상태
Laparoscopic hernia reduction and partial fundoplication이라는 수술을 하였고 깔끔히 좋아졌습니다.
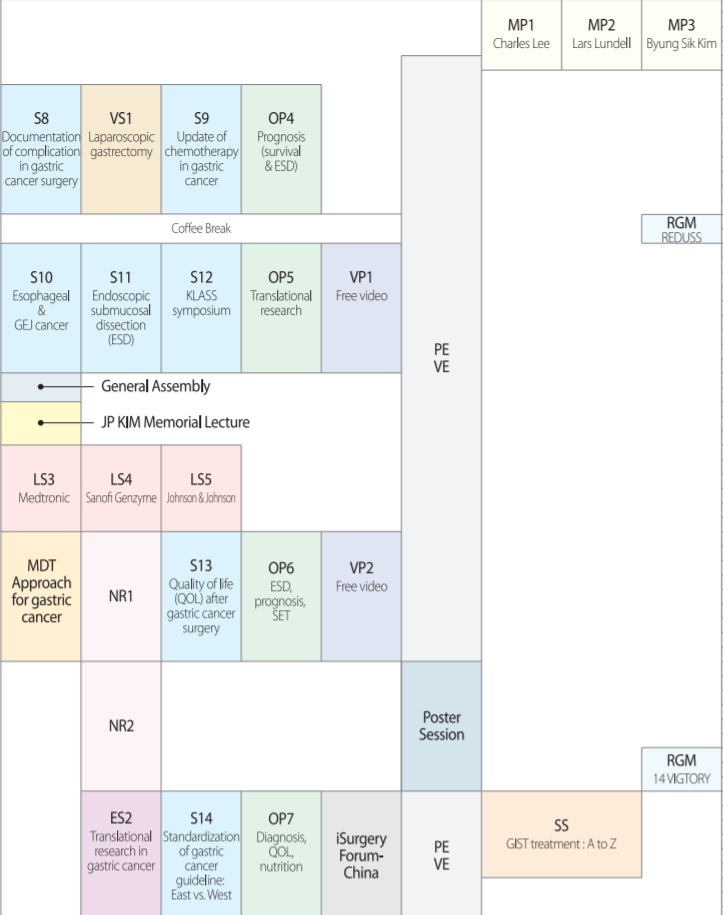
![]() 4. [금요일 10:10-11:40, Room C] Updates on ESD (endoscopic submucosal dissection) for EGC (early gastric cancer)
4. [금요일 10:10-11:40, Room C] Updates on ESD (endoscopic submucosal dissection) for EGC (early gastric cancer)
1. ESD for EGC with uncommon histological subtypes. 김광하 (부산대학교)
Papillary adenocarcinoma는 differentiated-type으로 간주되지만 differentiated-type tubular adenocarcinoma보다는 림프절 전이 위험이 높습니다. Papillary adenocarcinoma로 수술한 환자 중 ESD indication에 해당하는 17예 중 2예 (11.%)에서 림프절 전이가 있었습니다 (World J Gastroenterol 2015;21:3944). ESD로 치료한 papillary adenocarcinoma 중 37.5%가 noncurative resection으로 나왔습니다. 문제는 ESD나 수술 전 정확하게 papillary adenocarcinoma라고 알기 어렵다는 것입니다. 김광하 교수님은 ESD 적응증 관점에서 undifferentiated-type과 비슷하게 간주하는 것이 어떤가 제안하셨습니다. (Gastric Cancer 2017. accepted)
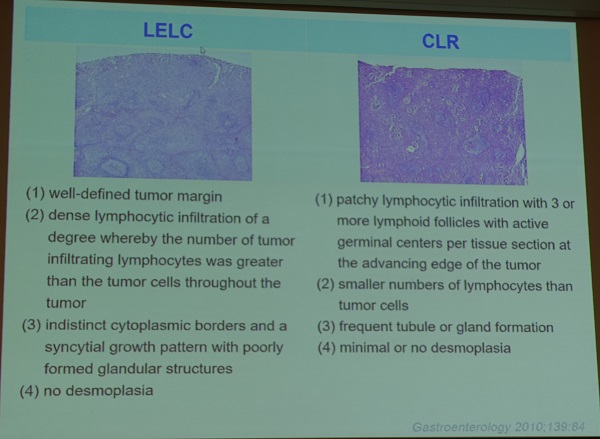
Carcinoma with lymphoid stroma (=lymphoepithelioma-like carcinoma)는 상대적으로 림프절 전이 위험이 낮았습니다. 크론병 비슷한 반응을 가진 암도 여기에 포함되어야 한다고 주장하셨습니다. 김광하 교수님는 carcinoma with lymphoid stroma는 carcinoid 처럼 약간 submucosal invasion이 있어도 내시경으로 치료할 수 있을 것 같다고 의견을 주셨습니다 (Surg Endosc 2017. accepted).

Poster
[2017-3-24. 이준행 질문]
Papillary adenocarcinoma가 LN 전이 위험이 높다면, ESD 후 minute SM invasion을 보인 환자에서는 additional surgery를 권하고 계십니까?
[2017-3-24. 김광하 교수님 답변]
Immunohistochemical staining 등을 통하여 lymphatic involvement 등에 대한 자세한 병리학적 검토를 하고 있습니다. Minute SM invasion 이외의 다른 risk factor가 없으면 careful follow up을 하고 있습니다. 통상의 환자보다 follow-up interval을 짧게 하고 있습니다. 보통의 환자는 ESD 후 6개월에 내시경과 CT 검사를 하고 이후로는 1년 간격으로 하고 있는데, papillary adenocarcinoma에서는 계속 6개월 간격으로 추적관찰하고 있습니다.
* 참고: 위암 분화도. 관찰자간 차이 및 시술 전후 차이 - 주미. 대한상부위장관헬리코박터학회 Summer workshop (2014)
2. ESD for undifferentiated type EGC. Yorimasa Yamamoto (Cancer Institute Hospital, Tokyo)
Yamamoto. Digest Endosc 2010
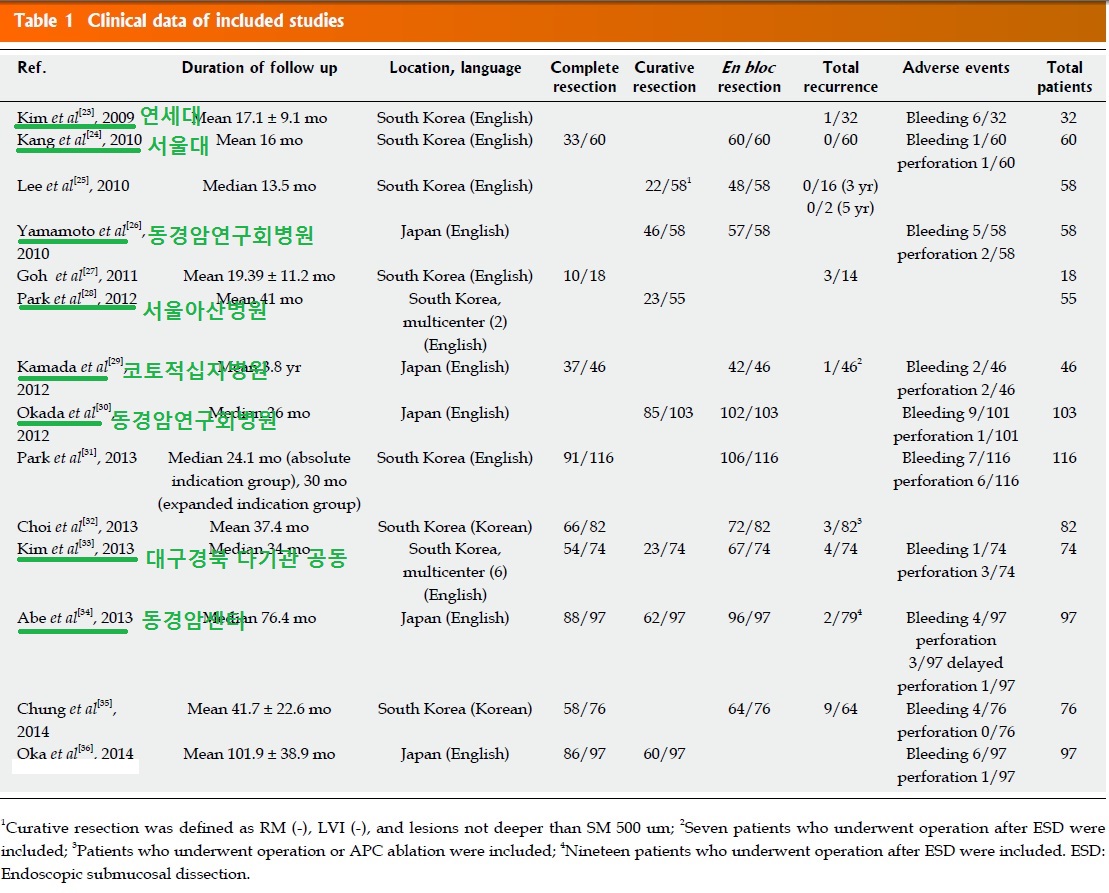
2015년 한림대학교 백광호 교수님 팀에서 발표한 meta-analysis를 소개되었습니다 (Bang CS. World J Gastroenterol. 2015). 14개의 연구(한국 10개, 일본 4개; 2개는 multicenter, 12개 영어, 2개 한국어)가 분석된 자료입니다.
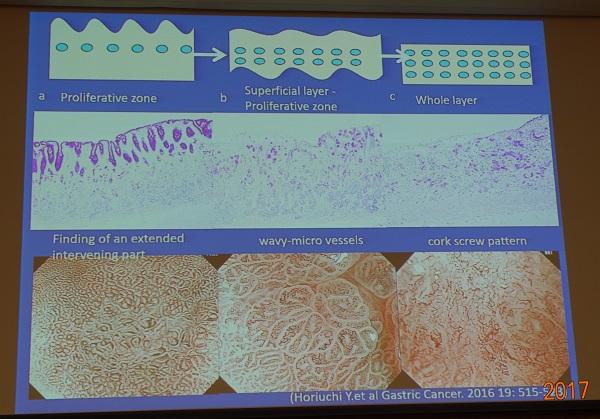
확대내시경을 통하여 undifferentiated-type cancer의 분포 영역을 파악하는 것이 중요합니다. Horiuchi Y. Gastric Cancer 2016;19:515
암연구회병원에서 undifferentiated-type EGC에 대한 내시경 치료의 장기 성적을 보여주셨습니다 .
P/D adenocarcinoma는 SM invasion을 잘 하기 때문에 점막암 상태에서 발견되는 경우가 많지 않습니다.
일본에서는 undifferentiated-type EGC에 대한 내시경 치료에 대한 다기관 임상연구가 진행되고 있습니다 (JOCG 1009/1010).
[2017-3-24. 이준행 질문]
Is there any difference in ESD for undifferentiated type EGC in Hp (+) or Hp (-) patients?
[2017-3-24. Dr Yamamoto 답변]
The demarcation line is more clear in Hp (-) patient, so it is easier to ESD. Hp (-) undifferentiated type cancer is frequently found in GC side of mid to lower body, and the color is pale.
* 참고: EndoTODAY Undifferentiated type EGC
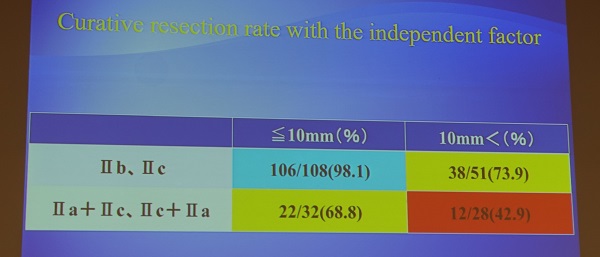
3. Longterm outcome of ESD after curative and noncurative resection. 이완식 (전남대학교)
조기위암 내시경 치료는 continuous process입니다. Indication에 따라 ESD candidate를 선정하고, 치료 후 병리결과에 따라 curability를 결정합니다.
Vertical margin이 양성이면 residual tumor가 40%, lymph node involvement가 10% 정도이므로 수술은 mandatory입니다.
Lateral margin 양성에서는 다양한 선택을 할 수도 있는데 second ESD를 할 수도 있고 수술을 권하기도 합니다 (EndoTODAY 절제변연 양성).
Non-curative resection에서 수술을 하지 않아도 disease specific survival에 차이가 없다는 자료가 많습니다.
* 활발한 discussion이 있었습니다. 김광하 교수님과 정훈용 교수님은 proximal location 병소의 non-curative resection의 경우 (1) 재발 우려는 좀 더 높다 점과 (2) total gastrectomy 후 삶을 질 저하 문제를 동시에 고려해야 한다는 입장에서 의견을 주셨습니다. 김광하 교수님은 조심스러운 follow up을 언급하셨고, 정훈용 교수님은 외과의사와 잘 상의하는 것이 중요하다고 말씀하셨습니다. 가톨릭대학교 외과 송교영 교수님께서는 (1) curability를 더 중요하게 생각해야 하고, (2) 좀 더 적극적으로 접근해야 한다는 의견을 주시면서 (3) proximal gastrectomy와 같은 또 다른 option이 있다는 점을 강조하셨습니다.
* 참고: EndoTODAY ESD curative resection 장기 성적
* 참고: EndoTODAY ESD non-curative resection 장기 성적
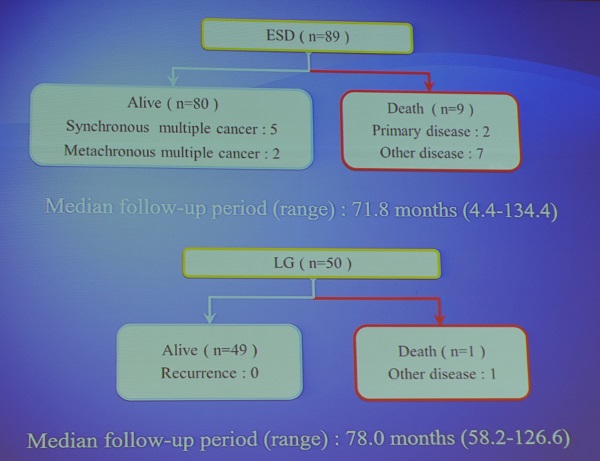
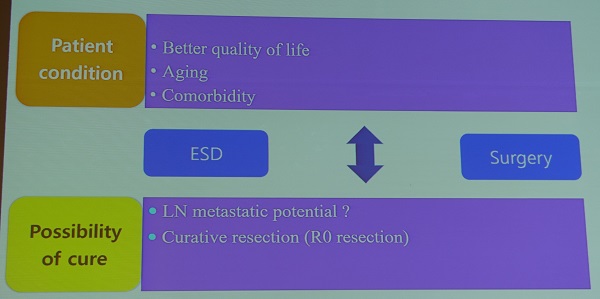
4. Survival benefit of surgery after ESD. 엄방울 (국립암센터)
Surgery rate가 낮은 이유는 '환자 factor' 못지 않게 '의사 factor'도 있습니다. 수술 후 no residual tumor가 나오면 환자에게 "축하합니다. 위암에 대한 모든 치료가 끝났고 당신은 cure 되었습니다'라고 말하지만, over-treatment를 한 것은 아닌가하는 생각을 하지 않을 수 없습니다.
6개의 연구를 보면 모두 upper line이 additional surgery입니다.
국립암센터의 propensity matching data 자료를 소개하여 주셨습니다. (Surg Endo 2017)
[2017-3-24. 이준행 comment]
Among non-curative resection groups in your institution, four patients died of metastatic gastric cancer during follow up. I want to know whether the patients was absolute indication, expanded indication or beyond indication cases in the beginning. It's because most of the non-curative resection cases with lymph node metastasis in surgery or death during follow up were originially out of indication cases. I want to see the initial endoscopy picture for non-curative ESD cases. Most analysis was based on post-treatment diagnostic group. Another analysis based on pre-treatment diagnostic group can give another insight.
* 참고: EndoTODAY ESD non-curative resection 장기 성적
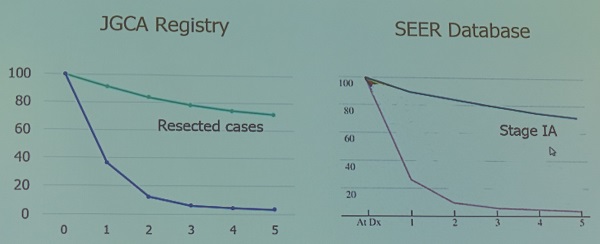
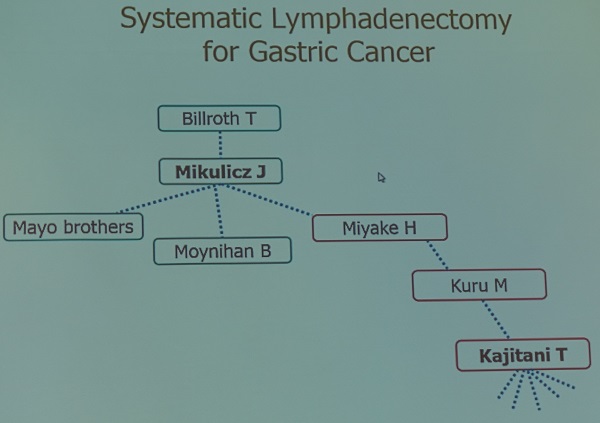
![]() 5. [금요일 점심. 김진복 교수님 기념 강연. Bridging between east and west in gastric cancer management. Professor Takeshi Sano (Japan)]
5. [금요일 점심. 김진복 교수님 기념 강연. Bridging between east and west in gastric cancer management. Professor Takeshi Sano (Japan)]
미국에서 수술한 환자의 성적은 일본에서 stage Ia 환자와 비슷한 성적을 보여주고 있습니다. 왜 이런 차이가 나올까요?
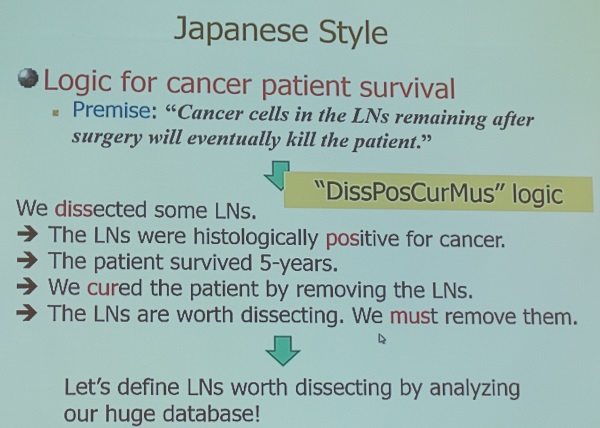
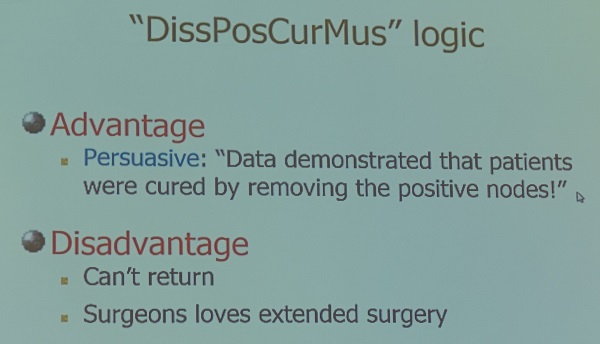
Japanese style이라는 제목의 슬라이드는 정말 인상적이었습니다.
서양과 동양을 bridging 하기 위해서는 (1) 용어를 통일해야 하고 (2) RCT를 해야 합니다.
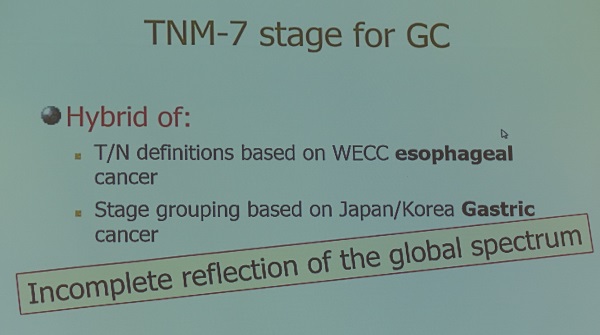
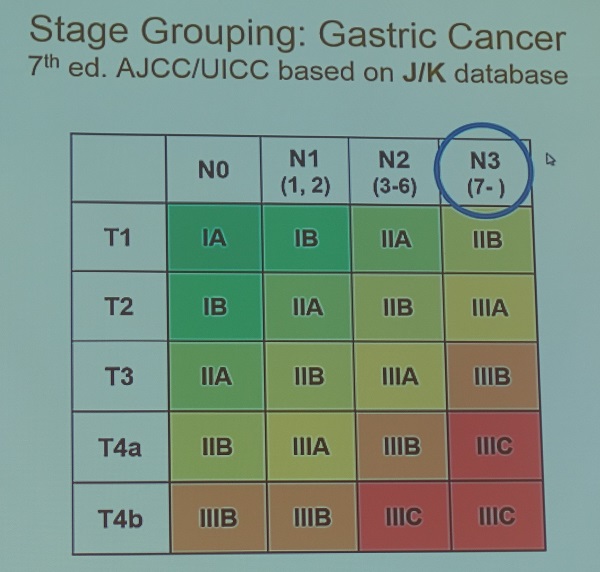
(1) 용어 통일을 위한 노력 (= TNM staging): TNM-7은 식도암과 위암의 hybrid인데 N3 node의 정의가 문제입니다. 식도암에서 7개 이상의 림프절 전이가 있으면 매우 예후가 나쁩니다. 그러나 위암에서는 7개 이상의 림프절 전이가 있어도 cure할 수 있습니다. IGCA staging을 새로 제안하였습니다.
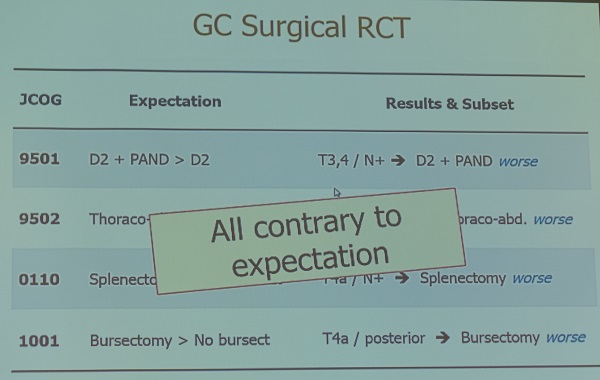
(2) RCT: 몇 가지 extended surgery에 대한 RCT는 negative 결과를 보였습니다. 그러나 subset analysis에서는 몇 가지 중요한 의미있는 소견이 있었습니다. 이러한 결과는 예상과 반대되는 것이었습니다. 많은 lesson 들이 있었습니다.
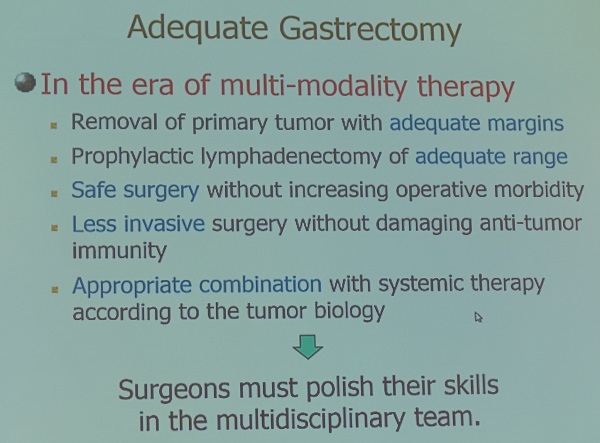
이제는 많이 가까워졌습니다.
![]() 6. [금요일 13:30-15:00, Room A] MDT approach for gastric cancer
6. [금요일 13:30-15:00, Room A] MDT approach for gastric cancer
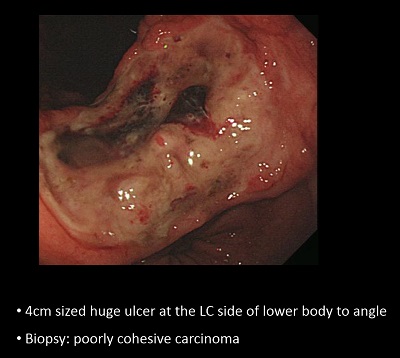
Case 1. AGC Borrmann type IV with peritoneal seeding.

Explo lapa를 하였으나 peritoneal seeding nodule이 있어 일단 항암치료 후 (리가타 trial에서 peritoneal seeding이 있는 경우 gastrectomy는 survival gain이 없었습니다.) 영상 소견이 좋아고 있었으나 obstruction 증상으로 stent 후 다시 explo를 하였는데 peritoneal seeding이 좋아져서 surgical resection을 하였고 no residual tumor로 나왔습니다. Peritoneal seeding이 short-term chemotherapy로 호전되었더라도 대부분 곧 재발하기때문에 항암치료를 계속하는 것이 좋겠습니다.

Case 2. AGC Borrmann type IV
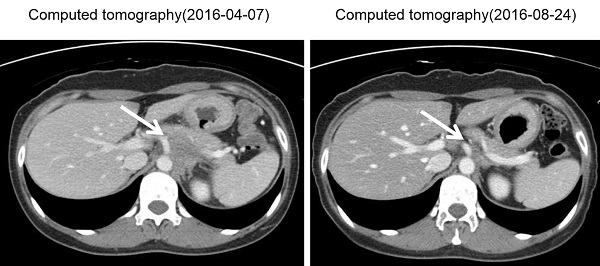
Imaging workup에서 definitely unresectable이었고 조직검사에서 c-ErbB +1, EGFR 2+ 였습니다. Preop chemotherapy (TS-1/Cisplatin) 후 left adrenal gland 주변의 soft tissue가 확실히 줄어들었습니다. 형우진 교수님은 peritoneal seeding 여부를 보기 위하여 explo lapa가 필요하다고 comment 하였습니다. Peritoneal seeding이 없다면 수술을 시도해 볼 수 있을 것 같습니다.
수술 (extended total gastrectomy + splenectomy + omentectomy + IP chemotherapy) 후 항암치료를 추가하였습니다.
Case 3. 임신 18주 위암.
복강경 수술을 하였고 수술 후 병기는 T4aN3M1였습니다. 수술 후 항암치료가 필요한데 태아를 어떻게 할 것인지 고민입니다. (1) Early delivery 혹은 (2) 임신을 유지하면서 항암치료.
일반적으로 임신 2기에는 가능하면 항암치료를 피하지만, 임신 3기에는 필요하면 임신을 유지하면서 항암치료를 하고 있습니다.
Case 4. Multiple ESD 후 협착
biopsy: tubular adenoma with HGD and suspicious for carcinomatous focus. ESD: M/D, 2.4cm in lamina propria.
biopsy: tubular adenoma, ESD: 9mm tubular adenoma
biopsy: atypical epithelium, favor W/D adenocarcinoma
ESD를 하였고 3.9cm lamina propria cancer with one resection margin involvement로 나왔습니다. 경과관찰, 추가 내시경 시술, 수술 중 어떤 방법을 택하시겠습니까?
Gastric outlet obstruction이 발생하여 여러번 balloon dilatation을 하였으나 증상이 지속되어 결국 subtotal gastrectomy를 하였고 residual tumor는 없었습니다.
[이준행 comment]
When more than half of the antral mucosa is removed by ESD, there is a chance of obstruction. In that case, we have 3 possible preventive options. (1) Oral steroid therapy for 4 to 8 weeks, (2) intralesional triamcinolone injection, and (3) histamine 2 receptor antagnosist rather than usual PPI, which is the most commonly used anti-acid medication after ESD. PPI seems to be too potent that it can induce overhealing.
[정훈용 교수님 comment]
다른 학술모임에서 한 번 논의했던 환자입니다. Clinical course가 길고, 합병증이 있었고, 결국 수술을 받았기 때문에 다소 의아해 하실 수 있을 것 같습니다. 그러나 이 환자의 경우는 수술을 무척 꺼려하셨다고 합니다. 진행성 위암이 아닌 상황에서 치료 방침의 선택에 있어 환자의 의견을 존중하지 않을 수 없을 것 같습니다.
* 참고: EndoTODAY ESD 후 협착
* 참고: EndoTODAY ESD 절제 변연 양성
![]() 7. [금요일 16:30-18:00. Room C] Standardization of gastric cancer guideline: East vs West
7. [금요일 16:30-18:00. Room C] Standardization of gastric cancer guideline: East vs West
1) Experience of development for Korean gastric cancer guideline - 김용일 (이화여대)
PDF 0.5M
[이준행 혼잣말] 제가 간사로 참여하여 만들었던 우리나라 위암 가이드라인(근거 기반 위암 진료 권고안, PDF 0.5 M)에 대한 내용인지라 감회가 새로웠습니다. 영국의 방법론을 그대로 사용하였고, 정치적 고려도 지나쳤기 때문에 날카로움을 잃고 모호한 가이드라인이 되어버린 것 같아 반성하고 있습니다. 여하튼 별로 인용되지 않는 결과를 낳고 말았습니다. 우리나라에서는 서양의 방법론을 그대로 따르기보다는 우리에게 도움되는 방향으로 우리 생각대로 일해야 한다는 것을 배웠습니다.
* 참고: EndoTODAY 가이드라인
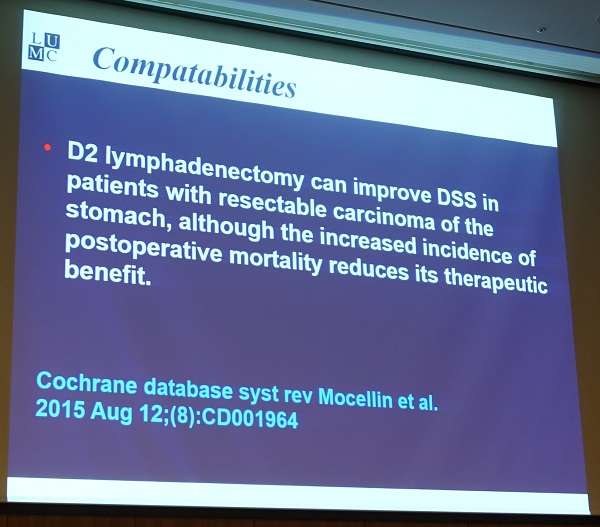
2) How to standardize gastric cancer management globally: expected difficulty and proposal - "western view" - Henk Hartgrink (Leiden University, Netherlands)
D2 lymph node dissection에 대한 서양인의 생각을 코크레인을 인용하여 보여주었습니다. 표준치료로 마지 못해 accept 하지만 여전히 걱정이 사라지지 않은 것 같습니다.
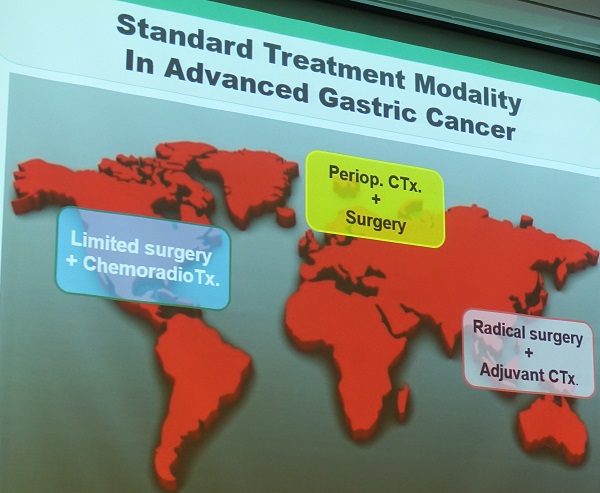
미국, 일본, 동양의 치료방법이 다르다는 것을 보여주는 슬라이드입니다.
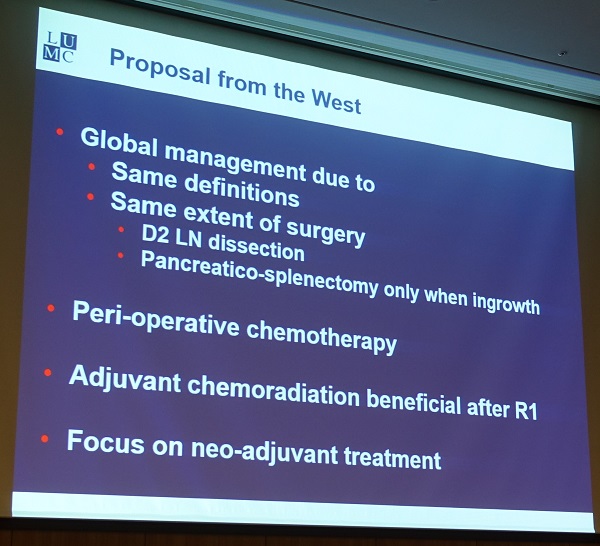
* Floor에서 한 서양인의 comment: "Adjuvant chemotherapy의 효과는 주로 proximal gastric cancer 혹은 GE junction cancer에서 현저하였습니다. Distal gastric cancer, pure gastric cancer에서는 그 효과가 명확하지 않았습니다. Distal gastric cancer 는 수술 alone으로 치료할 수 있는 것 아닌가요?"
3) How to standardize gastric cancer management globally: expected difficulty and proposal - "Japanese view" - Takeshi Sano (암연구회병원, 일본)
2017년 5번째 가이드라인이 발표될 예정입니다. 2010년 3번째 revision이 큰 변화를 가져왔습니다.
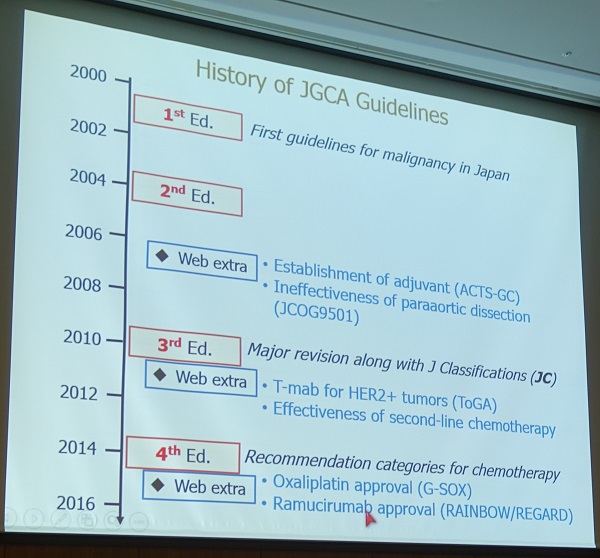
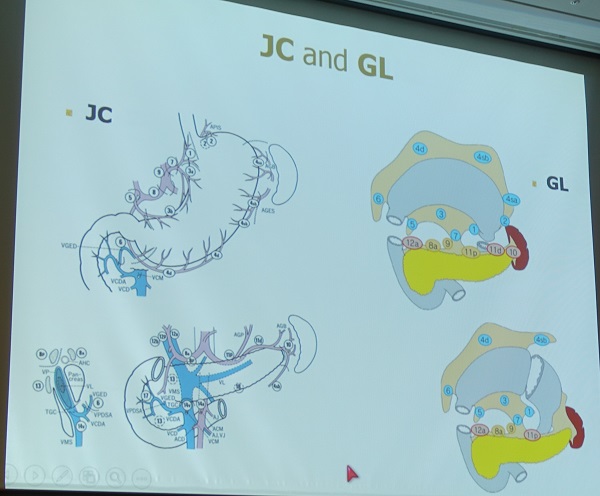
Japanese classification (JC)와 guideline (GL)을 구분해야 합니다.

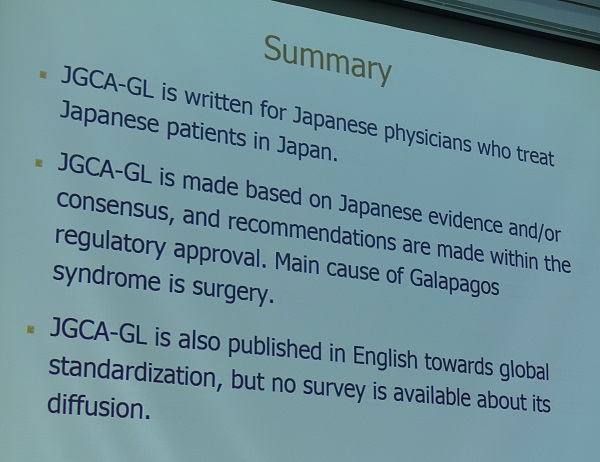
일본 가이드라인은 evidence-based guideline의 형식이 아니고 textbook format인 점이 가장 큰 특징입니다. Evidence level을 제시하지 않고, consensus-based임을 명확히 밝히고 있습니다.


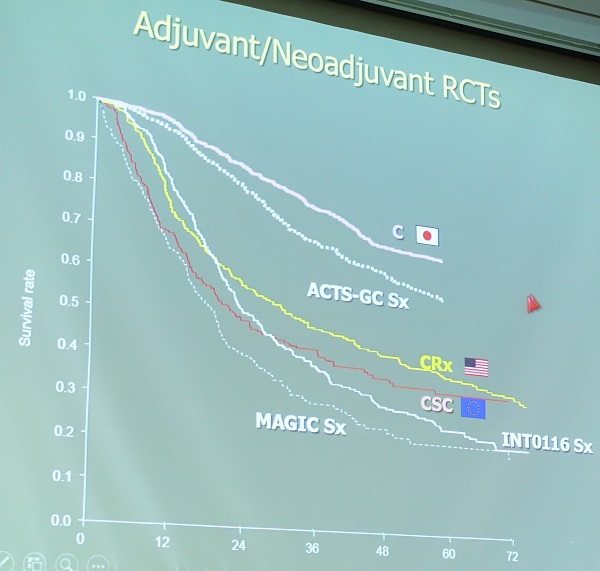
갈라파고스화 현상을 이야기 하였습니다. 일본 가이드라인은 일본에서 사용하기 위한 것입니다. 국제적으로 유명한 자료 조차도 사용되지 않고 일본에서 이루어진 연구 결과에 의존한 가이드라인이라는 것입니다. 예를 들어 유명한 MAGIC trial도 curative surgery가 드물었다는 이유로 일본 가이드라인에서 accepted 되지 않는다는 것입니다. 일견 비슷한 RCT라고 하더라도 survival curve가 너무 달라서 해외의 자료를 일본 가이드라인에 반영하기 어렵다는 것입니다.

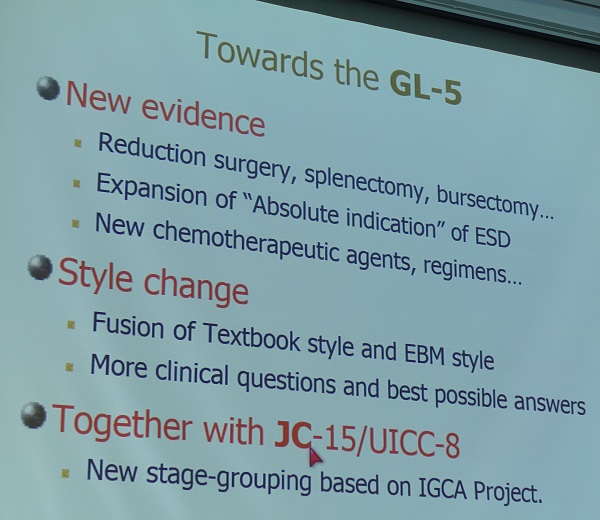
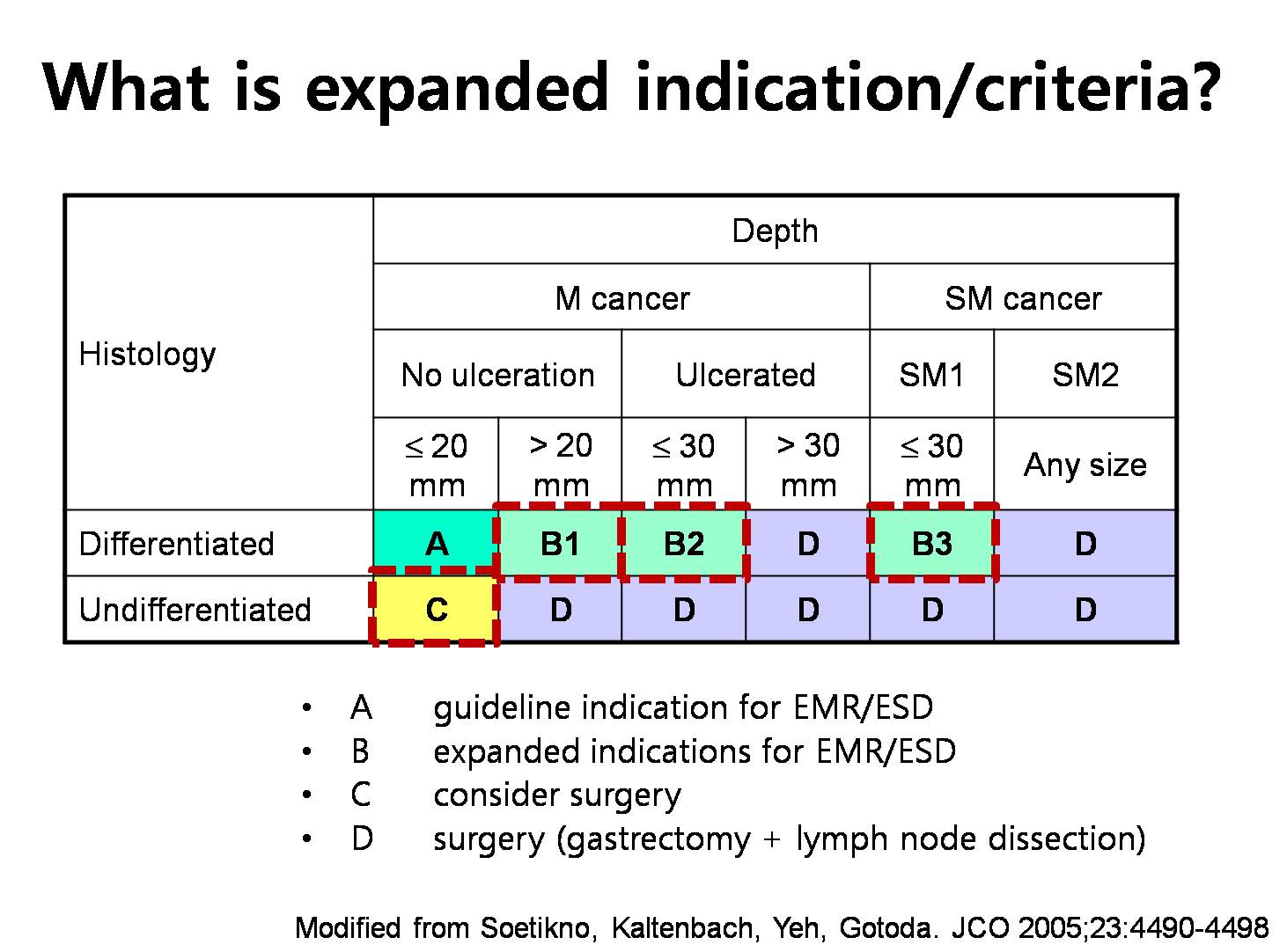
2017년 말에 일본가이드라인 5판이 발표될 예정이라고 합니다. 저의 관심을 끄는 부분은 "expansion of absolute indication of ESD"이었습니다. ESD에 대한 일본의 최근 견해가 반영될 것 같습니다. 가이드라인 위원회에는 내시경의사는 Dr. Ono (시즈오카 병원)와 Dr. Fujishiro (동경대학교)가 참여하고 있습니다. Some of expanded indication이 absolute indication으로 포함될 것이라고 합니다.
* 강의 후 다른 일본인 의사에게 문의하였을 때 점막하암이나 undifferentiated-type은 포함되지 않을 것이라고 합니다. Ulcer finding이 없으면 크기 제한이 없는 점막암, ulcer finding이 있으면 3 cm 이하의 점막암이 포함될 것 같다는 전언입니다. 아래 그림에서 B1과 B2만 absolute indication으로 포함될 것이라는 이야기 같습니다.
![]() 8. [토요일 7:30-8:20. Breakfast meeting] Palliative surgery for gastric cancer - Henk Hartgrink (Leiden University, Netherlands)
8. [토요일 7:30-8:20. Breakfast meeting] Palliative surgery for gastric cancer - Henk Hartgrink (Leiden University, Netherlands)
Palliation should foucus on (1) quality of life and (2) quantity of life.
Selection of words in this situation is important. 예를 들어 'fighting'이라는 단어를 쓰는 수가 많은데... 환자들은 싸울 기운이 없는 경우도 있습니다.
Stent vs surgery. 일반적으로 bypass가 유리하고 stent는 2개월 이상의 life expectancy가 예상될 때 선택할 수 있습니다 (Jeurnink SM. Gastrointest Endosc 2010). → (이준행 註) 이 연구는 malignant gastric outlet obstruction 환자를 대상으로 하였으므로 위암에 의한 gastric outlet obstruction에 대한 수술과 stenting의 효과를 비교한 RCT는 아직까지 발표된 바 없다고 보는 것이 맞습니다.
Chemotherapy는 약간의 survival gain이 있습니다. 4.3 vs 11 months
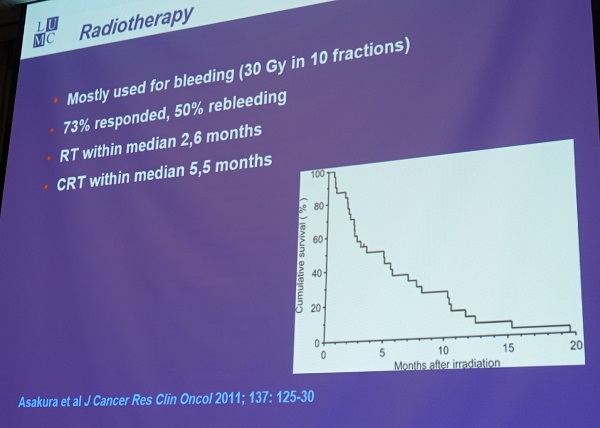
Radiation might be a good option for bleeding.
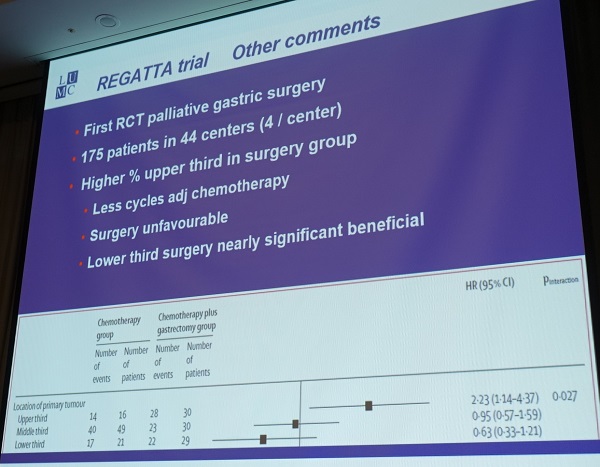
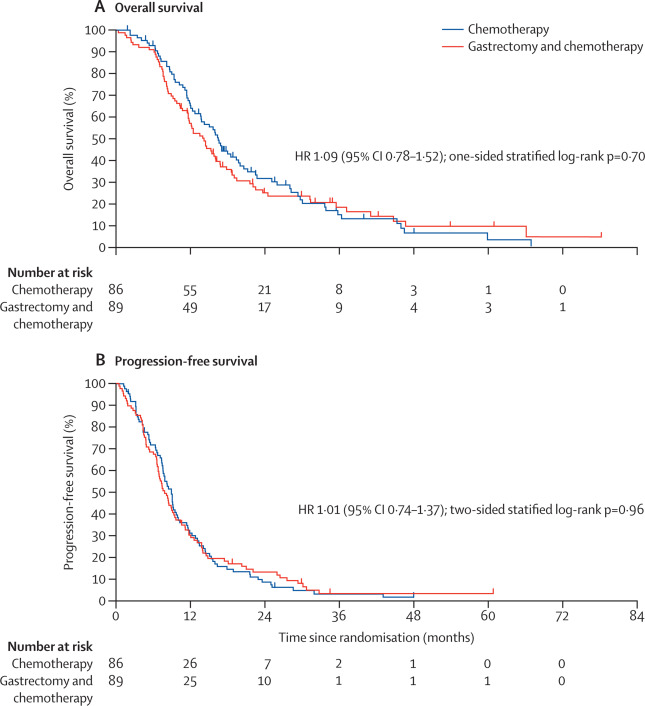
REGATTA trial 에서는 "Since gastrectomy followed by chemotherapy did not show any survival benefit compared with chemotherapy alone in advanced gastric cancer with a single non-curable factor, gastrectomy cannot be justified for treatment of patients with these tumours."라고 결론짓고 있으나 대부분의 환자는 peritoneal seeding이 있었고, 수술 환자에서 proximal cancer가 많았고, 한일 양국의 너무 많은 병원에서 너무 장기간 환자가 enrolled 되었다는 점이 지적되었습니다. 강사는 editorial을 보여주며 REGATTA trial의 한계점을 다시 한번 지적하였지만, major non-curative surgery should be discouraged라는데는 동의하였습니다.
(이준행 註) REGATTA trial은 한국과 일본 외과 의사들의 첫 공동 RCT입니다 (Fujitani K. Lancet Oncology 2016). 단일 전이가 있는 환자가 대상이었습니다. "We did an open-label, randomised, phase 3 trial at 44 centres or hospitals in Japan, South Korea, and Singapore. Patients aged 20-75 years with advanced gastric cancer with a single non-curable factor confined to either the liver (H1), peritoneum (P1), or para-aortic lymph nodes (16a1/b2) were randomly assigned (1:1) in each country to chemotherapy alone or gastrectomy followed by chemotherapy." 등록된 환자는 175명이었으나 참여 기관이 44곳이나 되었던 연구입니다. 한 기관에서 4명만 등록되었으니 상당한 우여곡절이 있었을 것 같습니다. 게다가 23명 (13.1%)은 항암치료도 받지 못하였읍니다. 여하튼 결과는 명확했습니다. "Median overall survival was 16·6 months (95% CI 13·7-19·8) for patients assigned to chemotherapy alone and 14·3 months (11·8-16·3) for those assigned to gastrectomy plus chemotherapy (hazard ratio 1·09, 95% CI 0·78-1·52; one-sided p=0·70)." 결론은 다음과 같았습니다. "Since gastrectomy followed by chemotherapy did not show any survival benefit compared with chemotherapy alone in advanced gastric cancer with a single non-curable factor, gastrectomy cannot be justified for treatment of patients with these tumours." 쓸모없는 수술은 하지 말자는 것 같습니다.
* 서울대 외과 이혁준 교수님 comments:
* 아산병원 외과 유문원 교수님은 palliative surgery와 stenting의 radomized trial을 하고 있는데 환자 enroll 하기가 매우 매우 어렵다고 말씀하셨습니다. 1년에 한 명 enroll도 쉽지 않다고 하네요.
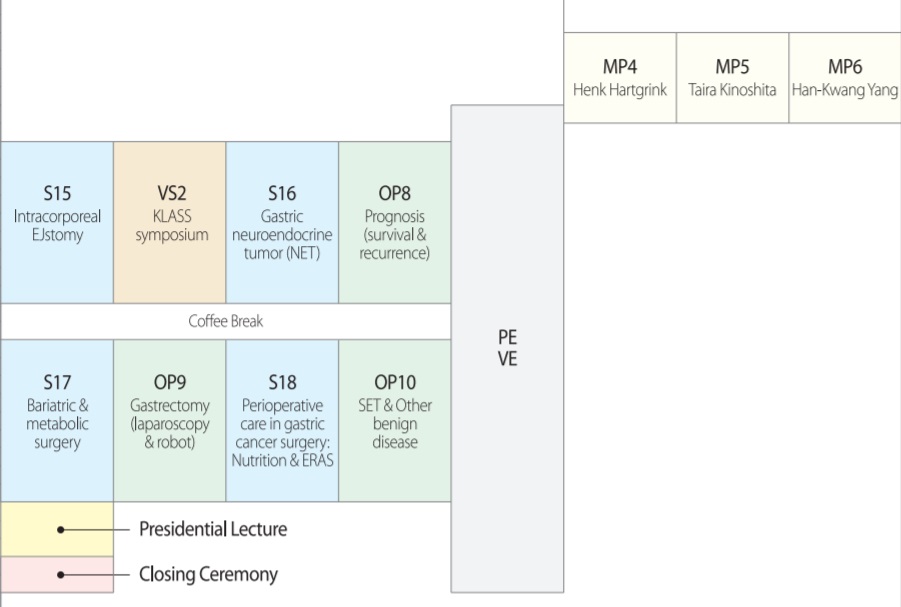
![]() 9. [토요일 8:20-9:50. Room C] Gastric NET
9. [토요일 8:20-9:50. Room C] Gastric NET
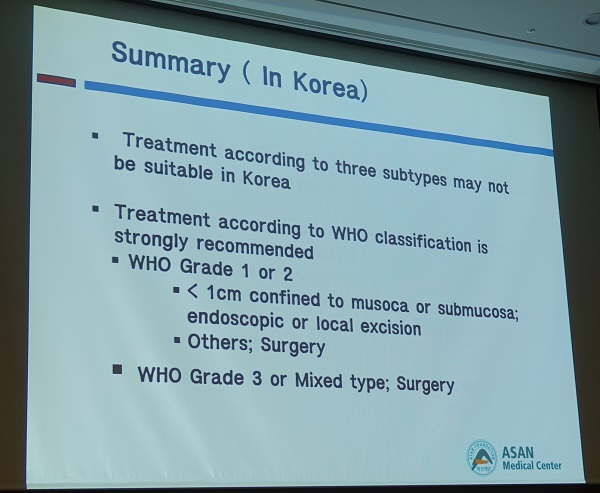
1) Management of gastric NET - 김범수
다양한 분류가 있습니다. Rindi, 2010-WHO 등

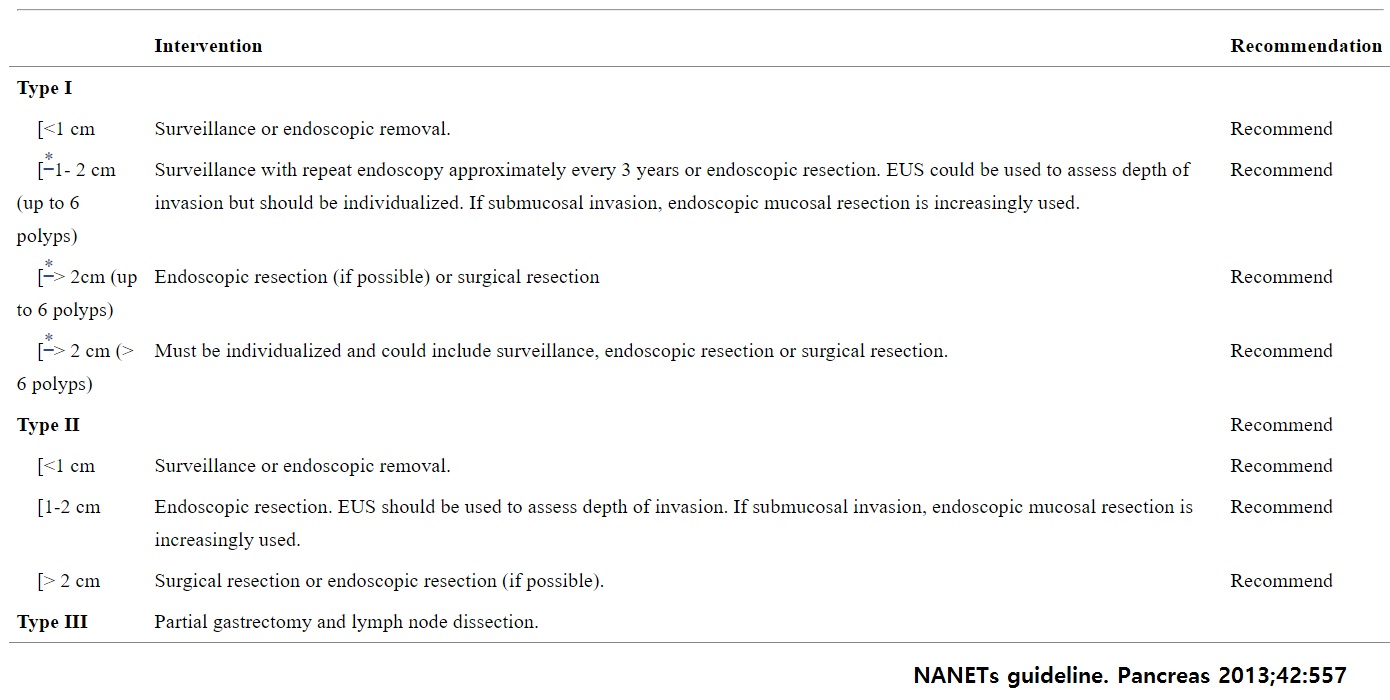
다양한 가이드라인이 있습니다. ENETS (유럽), NANETs (North America) , Nordic, Canadian, Turkey, Brazil 등. 한국 가이드라인이 없다는 것은 아쉽습니다.

아산병원 자료를 정리하여 발표한 자료를 소개해 주셨습니다
- Typical carcinoids and neuroendocrine carcinomas of the stomach: differing clinical courses and prognoses. Kim BS. Am J Surg 2010
- Prognostic significance of neuroendocrine components in gastric carcinomas. Kim BS. Eur J Cancer 2014
- Prognostic significance of neuroendocrine components in gastric carcinomas. Kim BS. Medicine (Baltimore) 2015
- Comparison of the prognostic values of the 2010 WHO classification, AJCC 7th edition, and ENETS classification of gastric neuroendocrine tumors. Kim BS. Medicine (Baltimore) 2016
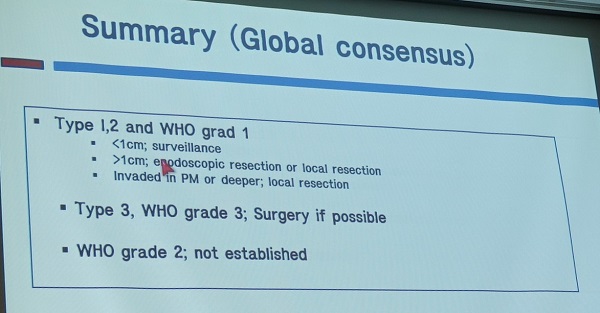
* Floor에서 배재문 교수님께서 lymph node dissection에 대한 질문을 하셨고, 김범수 선생님께서는 "Advanced type grade I-2 and all grade 3에 대해서는 D-2 dissection이 필요하다"고 답하셨습니다.
* 참고: EndoTODAY 위 신경내분비종양
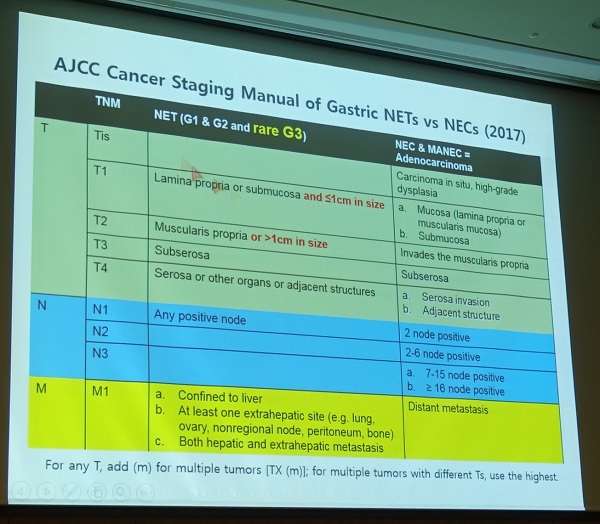
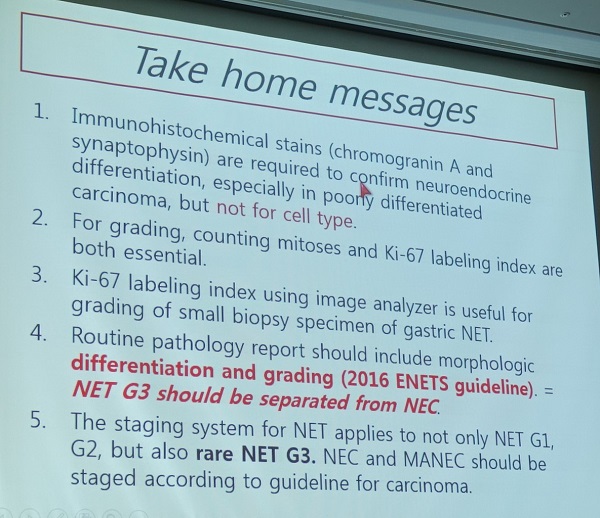
2) Pathologic findings of gastric NET - 조미연

Atrophic gastritis에 의한 ECL cell hyperplasia가 dysplasia로 되기 위해서는 몇 가지 추가적인 변화가 필요합니다.
Atrophic gastritis에 작은 neuroendocrine nodule을 만들었을 때에는 그 크기에 따라 hyperplasia와 dysplasia로 정의합니다.
Poorly-differentiated NEC와 NET G3는 비슷해 보일 수 있습니다.
Differentiation (well differentiated vs. poorly differentiated)과 grading (G1, G2, G3)은 어떤 관계가 있을까요?
Ki-67과 mitosis는 어떤 상관관계가 있을까요? 둘 다 중요하다는 것이 일반적이지만, Ki-67 labeling index 검사법 자체에 상당한 limitation이 있습니다. 최근에는 digital image analyzer의 도움을 받으면 검사의 성적을 향상시킬 수 있다고 합니다. NET에서는 mitosis 측정이 매우 어렵습니다. 아주 짧은 시간에 cell cycle에서 escape를 할 수 있으므로 NET에서는 Ki-67이 중요합니다. 반면 GIST에서는 mitosis가 중요하고 Ki-67은 routine하게 측정하지는 않고 있습니다.
G3 NENs에는 NET G3 (세포형: well differentiated) 와 NEC (세포형: poorly differentiated)가 있습니다.
G3 NENs에는 속하는 NET G3와 NEC는 예후가 다르다는 매우 중요한 연구입니다.
2010년에는 G3를 carcinoma로 분류하였습니다. 그런데 well-differentiated NET 중 grade 3인 경우는 poorly differentiated와 확연히 다르다는 것이 알려졌습니다 (특히 췌장에서). 따라서 2017년에는 well differentiated G3를 NEC로 부르지 않고 NET G3로 부르도록 하고 있습니다.
3) Chemotherapy for gastric NET - 오성용
치료방법 선택을 위해서는 differentiation과 resectability를 고려해야 합니다.
Response rate가 survival과 직접적으로 연결되지 않는다는 점이 특이합니다. Ki-67 labeling index가 높은 환자에서 response rate는 높지만 survival은 낮았습니다.
결론 슬라이드에서 "no indication for adjuvant treatment"가 다시 한번 강조되었습니다. 그러나 서울대 김형호 교수님께서 "실제로는 어떻게 하고 있는가?" 질문하였을 때, 연자는 NEC의 경우 근거는 거의 없지만 실제 임상에서는 항암치료를 하는 경우가 대부분이라고 답했습니다. 강의 내용과 실제 임상에서의 환자 치료가 다르다는 것은 큰 문제입니다. 연자들은 강의 중 이 점을 잘 밝혀야 할 것 같습니다. Neuroendocrine carcinoma (NEC)는 위암보다 나쁜 경우가 많기 때문에 특히 림프절 전이가 있었던 경우는 대부분 항암치료를 하고 있는 것 같습니다.
Gastric cancer with neuroendocrine differentiation에서는 어떻게 할 것인가 질문이 있었습니다. 조미연 선생님께서는 mixed type의 정의가 명확하지 않고 poorly differentiated carcinoma는 어는 것으로도 분화할 수 있습니다. Neuroendocrine carcinoma component가 30% 이상인 경우 mixed type으로 분류하고 있습니다. 이보다 더 적은 경우는 어떤 의미가 있는지 명확하지 않습니다. 30% 미만인 경우는 통상의 adenocarcinoma처럼 치료되고 있는것 같습니다.
![]() 10. [토요일 10:10-11:40. Room A] Bariatric and metabolic surgery
10. [토요일 10:10-11:40. Room A] Bariatric and metabolic surgery
1) Update of metabolic surgery from the Asian viepoint - Kazunori Kasama
일본에서도 metabolic surgery는 주로 private clinic에서 진행되는 모양입니다.
2) Results for the onco-metabolic surgery - 김종한 (고려대학교)
당뇨를 가진 위암 환자에서 위암 수술을 하면서 long limb bypass를 함께 하여 암도 치료하고 당뇨도 치료하는 효과를 얻을 수 있습니다.
3) Comparative study of non-reinforced staple line and reinforced staple line during laparoscopic sleeve gastrectomy - Hana Al Homoud (쿠웨이트)
쿠웨이트에서 태어나 오만에서 의대를 나오고 우리나라 고려대 안암병원에서 fellowship training을 받고 현재 쿠웨이트에서 surgeon으로 일하고 있는 여자 선생님이셨습니다.
부유한 아랍 국가에서 모든 healthcare는 공짜인데 bariatric surgery만은 cover되지 않는다고 합니다. 정부 공무원들이 bariatric surgery는 미용 수술로 간주하기 때문입니다. 그럼에도 불구하고 쿠웨이트에서는 bariatric surgery가 매우 흔하게 시행되고 있다고 합니다.
4) Korean prospective multicenter cohort study for morbid obesity: KOBESS (Korean OBESity treatment Study) trial - 허윤석 (인하대학교)
보건복지부에서는 2018년부터 비만 수술에 대한 보험급여를 시행할 계획을 가지고 있다고 합니다 (확정되지는 않음).
KOBESS trial에는 4개의 substudy가 있습니다.
![]() 11. [토요일 11:40-12:10. Room A] Presidential lecture - Where are we standing? Conclave for gastric cancer surgeons. 최승호 (연세대학교)
11. [토요일 11:40-12:10. Room A] Presidential lecture - Where are we standing? Conclave for gastric cancer surgeons. 최승호 (연세대학교)
우리나라에서 위암에 대한 최초의 (서양의학적) 보고는 세브란스 병원의 Dr. Ludlow가 하였습니다.
한국 전쟁 동안 처음으로 위암 수술이 시행되었습니다. 그러나 아쉽게 official record는 없습니다.
1961년에 연세대와 서울대에서 위암 수술에 대한 첫 보고를 하였습니다.
![]() 12. [Selected posters]
12. [Selected posters]
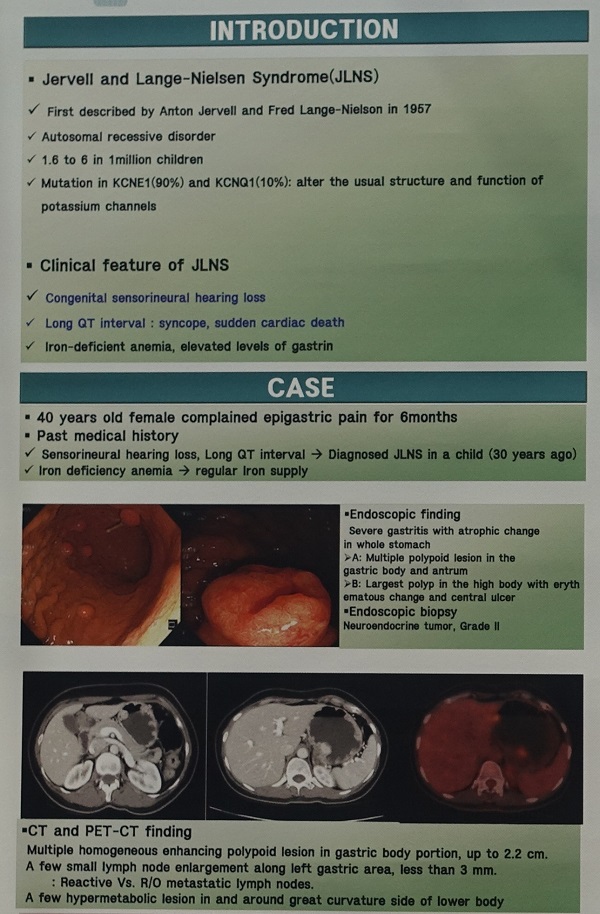
1) Jervell and Lange-Nielsen syndrome. Jee Ye Seob (단국대학교)
2) Early gastric cancer with lymphoid stroma (부산대학교)
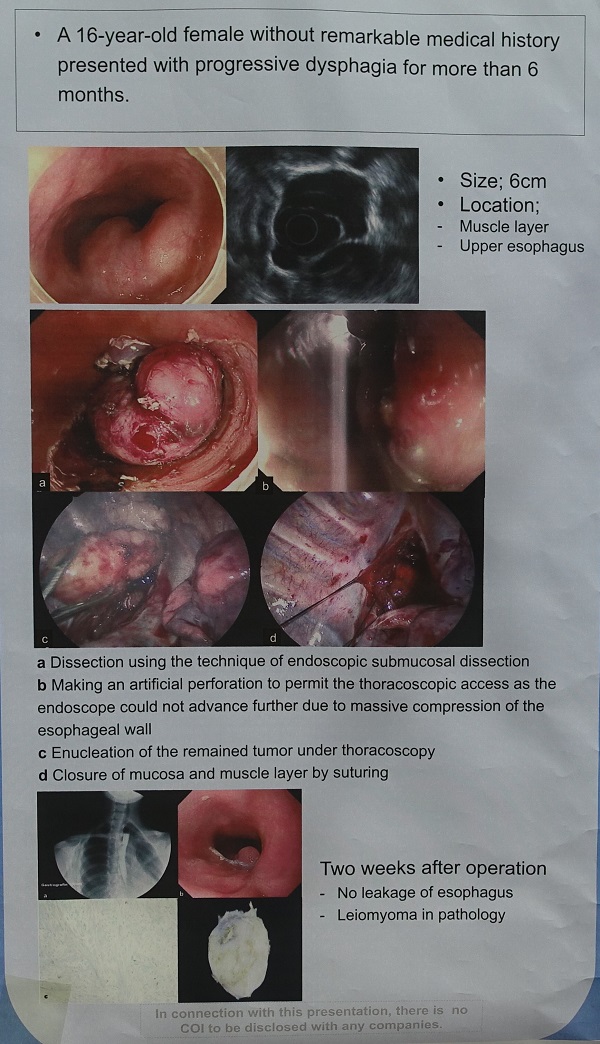
3) Thoracoscopic and endoscopic cooperative surgery (CHA university) - 청소년에서 발견된 식도 근종
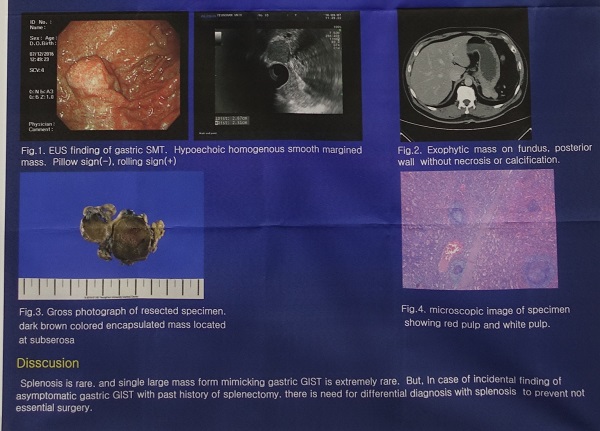
4) Splenosis mimicking GIST (영남대학교)
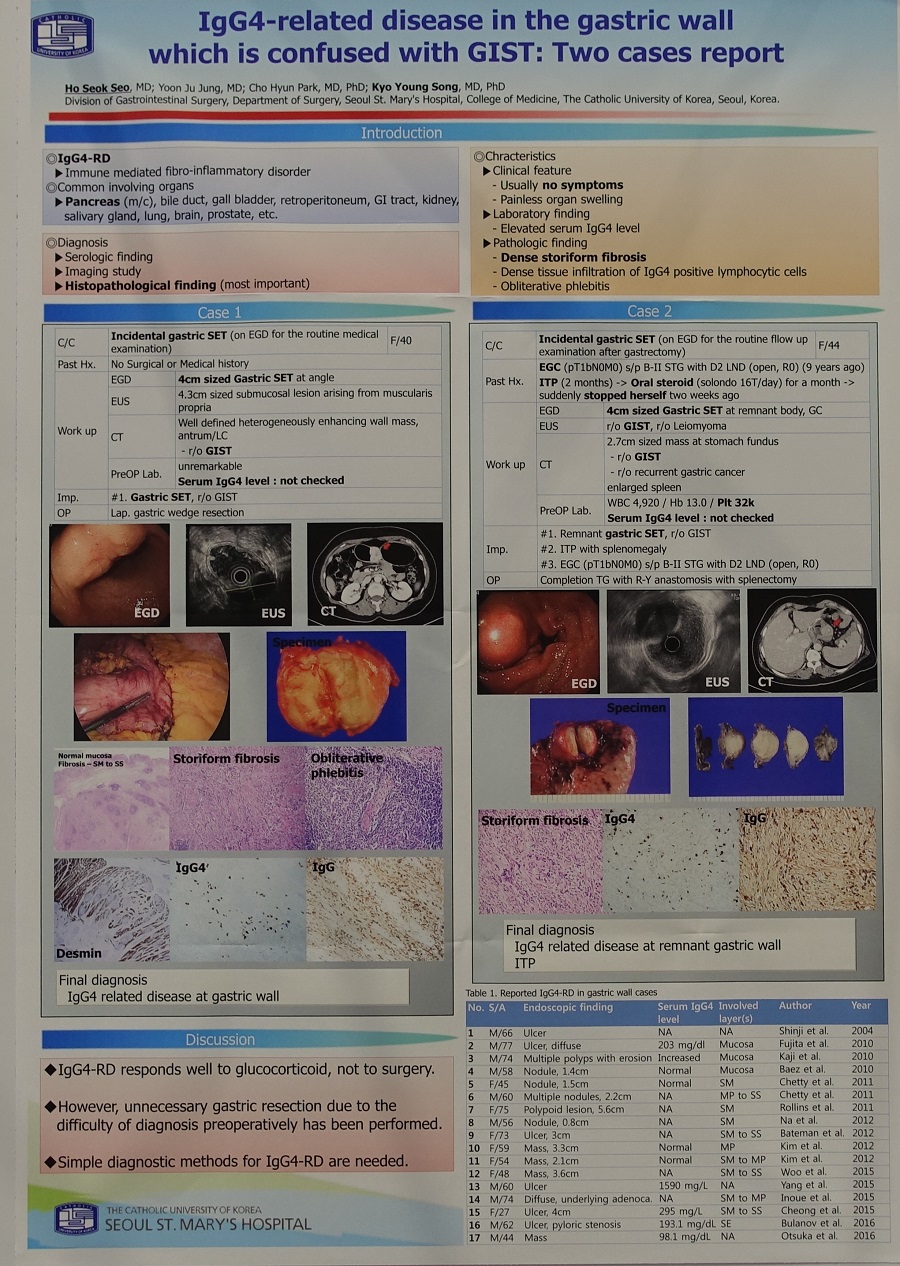
5) IgG4-related disease mimicking GIST (가톨릭대학교)
![]() 13. Management of gastric adenoma/dysplasia (이준행 강의)
13. Management of gastric adenoma/dysplasia (이준행 강의)
PPT PDF 3.0M
Thank you chairman for your nice introduction. It’s a great honor for me to talk in this wonderful meeting today.
When I talk about gastric adenoma or dysplasia, I always feel that there are similar limitations between dysplasia in the Barrett’s esophagus, and gastric adenoma/dysplasia. I would quote some comments from doctor Spechler’s review in 2005 on Barrett’s dysplasia. Ideally, the management of a disorder is based on / an unequivocal diagnosis / a firm understanding of the natural history / and definitive data regarding the risks and benefits of the treatment options. Unfortunately, none of these prerequisite factors may be available to guide the management of patients with dysplasia in Barrett’s esophagus. And I think the situation is exactly the same for gastric adenoma/dysplasia.
First of all, let’s see whether we have unequivocal diagnosis.
What is dysplasia? There are many definitions, but dysplasia usually means an unequivocal neoplastic transformation of the epithelium.
Then, what is adenoma? This is a Korean pathology guideline. It says that “In western countries, well demarcated elevated lesions are called as adenomas, and others as dysplasias. In eastern countries, not only elevated, but also flat/depressed lesions are called as adenomas.” Practically speaking, in Korea, gastric adenoma is the same meaning as gastric dysplasia.
These are two well-demarcated elevated type gastric adenomas.
This is a flat type gastric adenoma.
This is a depressed type adenoma with elevated margin.
Regenerating atypia can mimic gastric dysplasia and there is a significant overlap between them.
Conceptually, regenerating atypia is an inflammatory change, and dysplasia is a neoplastic change.
However, in clinical practice, it is not easy to discriminate between them.
This is an example. It is a huge benign gastric ulcer, which is a typical inflammatory change. But, initial pathology report was adenoma with low grade dysplasia.
The next issue is the inter-national variation in the pathological evaluation of gastric dysplasias. Historically, many grading systems have been proposed.
In Japan, group classification seems to be quite popular until now.
However, it is not easy to interpret the group classification into Vienna or other western classifications.
This is a very famous data showing western and Japanese pathologists have quite different point of view in the diagnosis of gastric dysplasias or early gastric cancers.
Korean pathologists and Japanese pathologists seem to have different criteria for gastric dysplasias and early gastric cancers. This issue is very complex and out of the scope of my presentation. But I want to tell you that we Korean endoscopists are treating a lot of patients with gastric adenomas, and some of them may be considered as well-differentiated gastric adenocarcinomas in Japan.
The third issue is inter-observer variation. This old man was referred with the histological diagnosis of adenoma with high grade dysplasia. When our in-house pathologist reviewed the outside biopsy slide, the diagnosis was changed into well-differentiated tubular adenocarcinoma. Because of this kind of inter-observer variation, we always review the outside pathology slides before deciding initial treatment plan.
Let’s move on to the second topic. Do we have a firm understanding of the natural history of gastric adenomas?
This is a typical understanding of the natural history of gastric dysplasia.
However, not all gastric adenomas progress into gastric cancers. In this case, there was no interval change as long as 8 years.
However, high grade dysplasias may progress into invasive carcinomas within quite short time interval.
When we perform endoscopic resection for gastric dysplasias, the final pathologic diagnosis can be changed into gastric cancers. So, it is not certain whether progression into gastric cancer in relatively short time interval means true disease progression or just under-evaluation due to small forceps biopsy specimen.
In this case, for example, pathology of the forceps biopsy was adenoma with low grade dysplasia. However, the final pathology of the ESD specimen was small well-differentiated tubular adenocarcinoma within lamina propria. So, what is important is not a progression of adenoma, but limitations of forceps biopsy.
One unique aspect of endoscopic treatment of gastric neoplasms in Korea is that the number of gastric adenomas are very high.
This slide shows how we are doing at my institution. Excluding palliative surgeries, we have endoscopically or surgically treated more than seventeen hundred gastric cancers in the year 2012. In this pie graph, you can see 263 adenomas with low grade or high grade dysplasia. All of them were treated endoscopically. Patients with small adenomas, which were treated by endoscopic ablation, were not included in this graph. So, endoscopic treatment of gastric adenoma is a huge workload for Korean endoscopists.
Practically speaking as an endoscopist, gastric neoplastic lesions can be divided into 6 groups, such as LGD, HGD, AI-EGC, EI-EGC, BEI-EGA and AGC. Diagnostic group classifications before the treatment can be changed after the treatment. The relationship is very complex. So the outcome analysis can be based on either pretreatment diagnostic groups or posttreatment diagnostic groups.
This flow diagram shows how we handled absolute indication early gastric cancers by the pretreatment diagnostic groups. This kind of analysis is more realistic. Among 355 early gastric cancers initially treated by ESD, 120 cases, this is 34 percent, belonged to the beyond absolute indication group. Ten percent of patients in the absolute indication group were initially treated by surgery, and you can see the reason in the box at the right hand-side corner. Suspicious lymphadenopathy is the most common reason for surgery. I think this kind of analysis based on the pretreatment diagnostic group has a lot of clinical meanings in the decision making among the treatment options.
We reviewed the discrepancy between pre-treatment diagnostic groups and post-treatment diagnostic groups in terms of histology, depth of invasion and absolute indications for ESD. As you can see in this slide, the rate of discrepancy is more than expected. When you see the cases with high grade dysplasia in the forceps biopsy, the rate of cancer in the final resected specimen is almost 34%.
Surgery was done before ESD era.
A majority of gastric adenomas is treated by ESD or EMR.
Adenoma with low grade dysplasia can be treated by either endoscopic resection or ablation. If there are some worrisome findings like central depression, or large size, endoscopic resection is usually done.
Doctors at Yonsei University reviewed the outcome of endoscopic resection for gastric adenomas with low grade dysplasia. They proposed that endoscopic resection is necessary for low grade dysplasias larger than 2 cm and don’t have pale discoloration. So, endoscopic resection is not necessary for all low grade dysplasias.
Small, flat, and pale adenoma with low grade dysplasia is treated by ablation in my clinic.
Ladies and gentlemen, I’d like to conclude my presentation by saying that adenomas with low grade dysplasia can be treated by either endoscopic ablation or resection depending on the clinical characteristics. Adenomas with high grade dysplasia should be resected due to the very high risk of cancer.
Thank you for your attention.
![]() [보도자료]
[보도자료]
위암은 우리나라에서 가장 흔하고 중요한 암 중 하나이다. 3월 23일 오전 위암 검진 심포지엄에서는 1999년 시작된 우리나라 위암검진사업의 장기 성적이 발표되었다 (국립암센터 최일주). 전국민을 대상으로 한 대규모 자료를 통하여 위암 검진을 받은 사람은 그렇지 않은 사람에 비하여 위암으로 인한 사망률이 현저히 감소된다는 것이 입증되었고 이러한 자료는 최근 미국소화기학회지에 발표되었다. 40세부터 74세 성인 중 위암 검진 내시경을 한번이라도 받은 경우 위암 사망률이 49% 감소되었다. 이러한 효과는 내시경 검사를 반복적으로 받은 경우 더욱 현저하였는데, 내시경 검사를 1번 받은 사람에서는 위암 사망률이 37% 감소되는 것에 비하여, 내시경 검사를 2번 받은 경우는 68%, 내시경 검사를 3번 이상 받은 경우는 81% 감소되어 정기적인 검진 내시경이 위암 사망률을 현저히 낮춘다는 것이 입증되었다. 그러나 이와 같은 위암 사망률 감소 효과는 위장조영술 (위장 촬영)에서는 나타나지 않았다. 향후 위장조영술을 이용한 위암 검진은 사라지고 위내시경이 주로 이용될 것으로 예측된다. 암검진 사업의 효과를 높이기 위하여 2008년 암검진 질관리 지침이 발표되었고 이에 따른 질향상 노력이 지속되고 있다. 향후 위암 검진 분야의 보다 큰 발전이 기대된다.
위암 검진 내시경을 받는 사람이 많아지면서 조기위암의 비중이 높아지고 있으며 개복수술 혹은 복강경 수술을 받지 않고 내시경치료를 받는 환자도 많아지고 있다. 한 대형 병원의 자료에 의하면 2016년의 경우 전체 위암의 71%가 조기위암이었고, 전체 위암의 30%가 내시경으로 치료되었다.
위암 검진 내시경을 받는 동안 위암 이외의 다른 질병도 발견되고 있다. 이 중 위암의 전구병소인 위선종(腺腫)은 내시경치료를 통하여 치료될 수 있다 (성균관의대 이준행 교수). 위 선종은 그 중증도에 따라 저도 선종과 고도 선종으로 나누어지는데, 저도 선종은 내시경 절제술 혹은 내시경 소작술로 치료될 수 있는 반면 고도 선종은 대부분 내시경 절제술로 치료되고 있다. 선종의 내시경 치료 후 최종 병리결과에서 위암으로 진단이 바뀌는 경우가 많기 때문에 선종에 대한 적극적인 치료가 필요하다.
![]() [References]
[References]
© 일원내시경교실 바른내시경연구소 이준행. EndoTODAY Endoscopy Learning Center. Lee Jun Haeng.